
Abstract
Abstract
Background:
Surgical site infection (SSI) is the most common type of healthcare-associated infection, contributing to substantial annual morbidity, costs, and deaths. In the United States it is the number one reason for hospital re-admission after surgery. Relatively little attention has been paid to the proportion of SSIs that occur after discharge. This paper systematically reviews two decades of publications to characterize better the proportion of SSIs that are identified after discharge and the need for better early detection and treatment.
Methods:
A restricted systematic literature search was conducted in PubMed to identify English-language studies published after 1995 that include the occurrence of pre-discharge and post-discharge SSIs. The data abstracted were the date of publication, country of origin, procedure, study design, surveillance system, population size, follow-up rate, and SSI counts and proportions. Descriptive statistics and forest plots were used to characterize the data set, represent the overall proportion of SSIs occurring after discharge, and assess the heterogeneity of the studies.
Results:
A total of 55 articles met the inclusion criteria, with data from 1,432,293 operations and 141,347 SSIs based on studies from 15 countries. The overall proportion of operations leading to SSI was 9.9%. Of the 141,347 infections, 84,984 (60.1%) appeared after discharge. The proportion of SSIs after discharge differed among studies, from 13.5 to 94.8, and was heterogeneous for all studies and for most individual surgery types.
Conclusion:
Post-discharge SSIs constitute the majority of these infections and pose a substantial disease burden for surgical patients globally and for different surgery types. Further examination is warranted to determine the methodologic and clinical factors moderating the proportion of post-discharge SSIs.
S
Despite ample research on the causes, costs, and overall rates of SSI, comparatively little attention has been paid to the proportion of SSIs that are identified after hospital discharge. Characterizing this ratio is important for surgeons, whose assessment of operative risk and discharge plans must account for the likelihood of post-hospital infections, including those in patients lost to follow-up. It is likewise important for patients, who depend on accurate information for pre-operative consent and are largely responsible for their own monitoring after discharge and between follow-ups.
We reviewed two decades of publications systematically to characterize the incidence of post-discharge SSI and the need for better early detection and treatment. The proportion of SSIs identified post-discharge (out of total SSIs) was calculated for all operations and for selected sub-groups through descriptive statistics and data visualization. Meta-analysis was used to ascertain a pooled estimate of the percentage of SSIs that is identified after discharge.
Materials and Methods
Literature search
A systematic literature search was conducted in PubMed for English-language studies published on or after January 1, 1995, that included the pre-discharge and post-discharge incidence of SSIs. Foreign-language studies were not included because relevant data often are presented in untranslated figures and tables.
The dates of analysis were restricted to 1995 and later because of temporal trends in hospital length of stay (LOS), which declined particularly rapidly in the U.S. during the mid-1980s, in step with a global trend toward shorter hospital stays [4–6]. Although LOS continues to decrease, the rate of decline now is less dramatic and thus less likely to affect the proportion of SSIs that are found after discharge [7]. Additionally, restriction to the most recent two decades helps account for subtle changes in hospital policy, surgical approaches, and antibiotic use/effectiveness as a result of cultural, institutional, and paradigmatic shifts.
When necessary, surgery was defined as an invasive procedure using surgical tools, requiring operating room facilities, and not performed strictly as part of routine screening. This excluded minor procedures such as mole removal, abscess incision and drainage, and colonoscopy. However, most studies did not report data for specific procedures, and the definition of surgery was left to the study authors or to the databases from which the studies drew their sample populations.
There is extensive global literature on SSI published in the last two decades, encompassing research studies from diverse fields within medicine and epidemiology. A comprehensive search for manuscripts using non-restrictive keywords yielded search results beyond the resources of the authors to review effectively. For example, a PubMed search for “surgical site infection” after 1995 yielded more than 25,000 articles. Consequently, we worked with a university librarian to create more limited search terms that would have a greater likelihood of returning relevant papers. In particular, because this study was concerned with the proportion of SSIs identified after discharge, rather than the incidence rate of SSI, search terms were chosen to limit returned articles to those that reported data on post-discharge infections. “Re-admission” was included, along with the appropriate MeSH term for discharged patients because we assumed that papers with these terms were more likely to include post-discharge data. In addition to limiting search terms, we restricted our review to the PubMed database.
The first author conducted the literature search using the following terms:
(post-discharge [All Fields] OR readmission [All Fields] OR “patient discharge” [MeSH Terms]) AND (“surgical wound infection” [MeSH Terms] OR SSI [All Fields] OR “surgical site infection” [All Fields] OR “surgical site infections” [All Fields]) AND (“1995/01/01” [PDAT]: “2015/06/08” [PDAT])
Case definition
Briefly, SSI is defined by the U.S. Centers for Disease Control and Prevention (CDC) as an infection that occurs within 30 days after an operation with no implant or within 1 year of an operation if an implant is placed [8]. The infections are further categorized by the CDC as superficial incisional (involving only the skin or subcutaneous tissue), deep incisional (involving deep soft tissues of the incision such as fascia and muscle), or organ/space (involving any part of the anatomy other than the incision). Although the definition of infection differs by type, generally, it is defined by either purulent drainage, isolated organisms, diagnosis by a clinician, or signs/symptoms of infection (e.g., abscess, localized swelling, pain/tenderness).
Some surveillance systems employ modified CDC diagnostic criteria. The U.K.’s Surgical Site Infection Surveillance System (SSISS; previously NINSS), for instance, uses a version that removes clinician opinion and mandates observation of pus cells to distinguish incisions that are infected from those that are simply colonized [9]. The Australian Council of Healthcare Standards defines SSI as “any surgical wound from which purulent material drains or is obtained,” with no requirement for microbiological confirmation and exclusive of local reactions to suture [10]. Other definitional criteria include scoring of the need for
Inclusion and exclusion criteria
Included articles reported the number or proportion of both pre-discharge and post-discharge SSIs to account for different standards in assigning the diagnosis. Studies for which the proportion could be calculated using reported data also were included. To meet the inclusion criteria, papers reported the number of SSIs and either the total patient population or the total number of operations performed.
Studies were excluded if they reported only the number of post-discharge SSIs, only the number of pre-discharge SSIs, or only one SSI subtype (e.g., “deep incisional SSI”). Studies also were excluded if the reason for re-admission or presentation was not explicitly an SSI; if the reported SSI rate was restricted to infections for which a procedure (e.g., “surgery due to SSI”) was performed; and if the reference population was in an obviously underserved or resource-poor country/setting, as determined by the authors. The latter were excluded because of concerns about consistent use of pre-operative antibiotics, poor follow-up, and low generalizability. Studies were not required to report the duration of post-surgical monitoring or to adhere to the CDC-specified 30-day window for diagnosis, because the length of follow-up is a less important moderator of SSI incidence than other factors, including surveillance strategy [8,13]. Furthermore, we did not exclude articles that did not explicitly use the CDC criteria for the diagnosis of SSI, because the definition of SSI used by authors was inconsistently reported, and alternative yet acceptable standards exist, as described above.
We did not employ data quality screens, as there are no published standards for grading uncontrolled studies of post-discharge SSIs.
To screen out articles published in potentially predatory open-access journals, all journal and publisher titles were compared with Beall's List, an open-access site used for monitoring these publications [14].
Data gathering and analysis
After identification of relevant articles, the data were abstracted for date of publication, country of origin, procedure, study design, surveillance system, definition of SSI, population size, follow-up rate, and SSI counts and rates. A forest plot was used to present the overall proportion of SSIs occurring after discharge as well as the heterogeneity of the study data. In studies that reported different population sizes for patients and procedures, the number of procedures was used as the population size, because these studies often included multiple procedures on single patients over a span of several years, making number of procedures the better gauge of the SSI rate. For prospective cohort studies, followup rates were abstracted or calculated when possible.
The proportion of SSIs occurring pre-discharge was not adjusted for patients lost to follow-up, because follow-up was believed to be more likely in patients with a suspected post-discharge SSI diagnosis. In studies of non-implant procedures reporting a 30-day post-operative infection rate in addition to longer periods of follow-up, the 30-day rate was used, consistent with the CDC diagnostic criteria [8]. In studies that either did not report the length of follow-up or reported longer follow-up periods, SSI counts were not adjusted for the duration of follow-up.
Proportion estimates and standard errors were determined using all 55 studies that met the inclusion criteria. We did not attempt to make adjustments for average length of in-patient hospital stay, surgery type, or country of origin. Because the proportion of SSIs identified after discharge was heterogeneous among the 55 studies, we did not attempt meta-analysis and instead present these data as a forest plot without a modeled pooled estimate.
Sub-group analysis was carried out for select surgery types. Sub-groups were chosen on the basis of availability of data, with no sub-group containing data abstracted from fewer than three studies. Sub-groups were eligible for selection if they were either the only surgery type in the study or if they were analyzed as a discrete sub-group of a larger study (e.g., post-discharge colorectal surgery SSI rates within a study of multiple types of surgery). We chose three studies as the threshold because sub-groups of one or two studies were unlikely to yield meaningful results for practicing surgeons, although meta-analysis can be conducted on as few as two studies. Despite making every effort to maximize the specificity of sub-groups, the diversity of operations and reporting of pooled data by included studies prevented analysis more specific than a surgical specialty in some cases (e.g., orthopedics). Studies reporting a single post-discharge SSI rate for multiple surgery types and studies reporting an otherwise-uncategorizable operation were placed in a broad category labeled “other.” Each sub-group was exclusive of all other sub-groups. Studies and patients in the appendectomy sub-group were not counted in the general surgery sub-group, for example.
Sub-groups were analyzed using meta-analysis. Because of the diversity of patient populations, procedure types, and study designs, a random effects model was created to evaluate the proportion of SSIs found after discharge. Tests of non-compatibility also were carried out, using Cochran's Q and the I2 statistic. We chose a Cochran's Q p value >0.10 as a threshold to indicate lack of heterogeneity. The I2 statistic was divided categorically into high (>75%), moderate (25%–75%), and low (<25%) for all meta-analyses [15].
Exploratory analysis was conducted using meta-regression to determine the moderating influence of study design and country of origin and their impact on heterogeneity in the pooled analysis using all 55 studies. Average temporal changes using publication year also were assessed.
All analysis was conducted with R version 3.1.1 using the package metafor [16]. Significance was assumed at p < 0.05.
Results
The systematic literature search conducted between June 1 and June 8, 2015, returned 474 papers whose abstracts were screened for relevance. The full text was reviewed for 180 potentially relevant articles.
In total, 55 articles met the inclusion criteria, having data from 1,432,293 operations and 141,347 SSIs [17–71]. The overall rate of SSI (total SSIs/total operations) was 9.9%. The study by Apte et al. was excluded from calculation of the percentage of SSI after surgery because it did not report the total number of coronary artery bypass graft operations performed [17]. Of the 141,347 SSIs, 84,984 (60.1%) were identified after patient discharge.
The characteristics of the included studies are summarized in Fig. 1, with selected descriptive statistics in Table 1. The studies came from Europe, North America, South America, Australia, and New Zealand (Fig. 2). Study populations, methods of follow-up, and procedures differed. Thirty-nine studies (71%) were prospective.
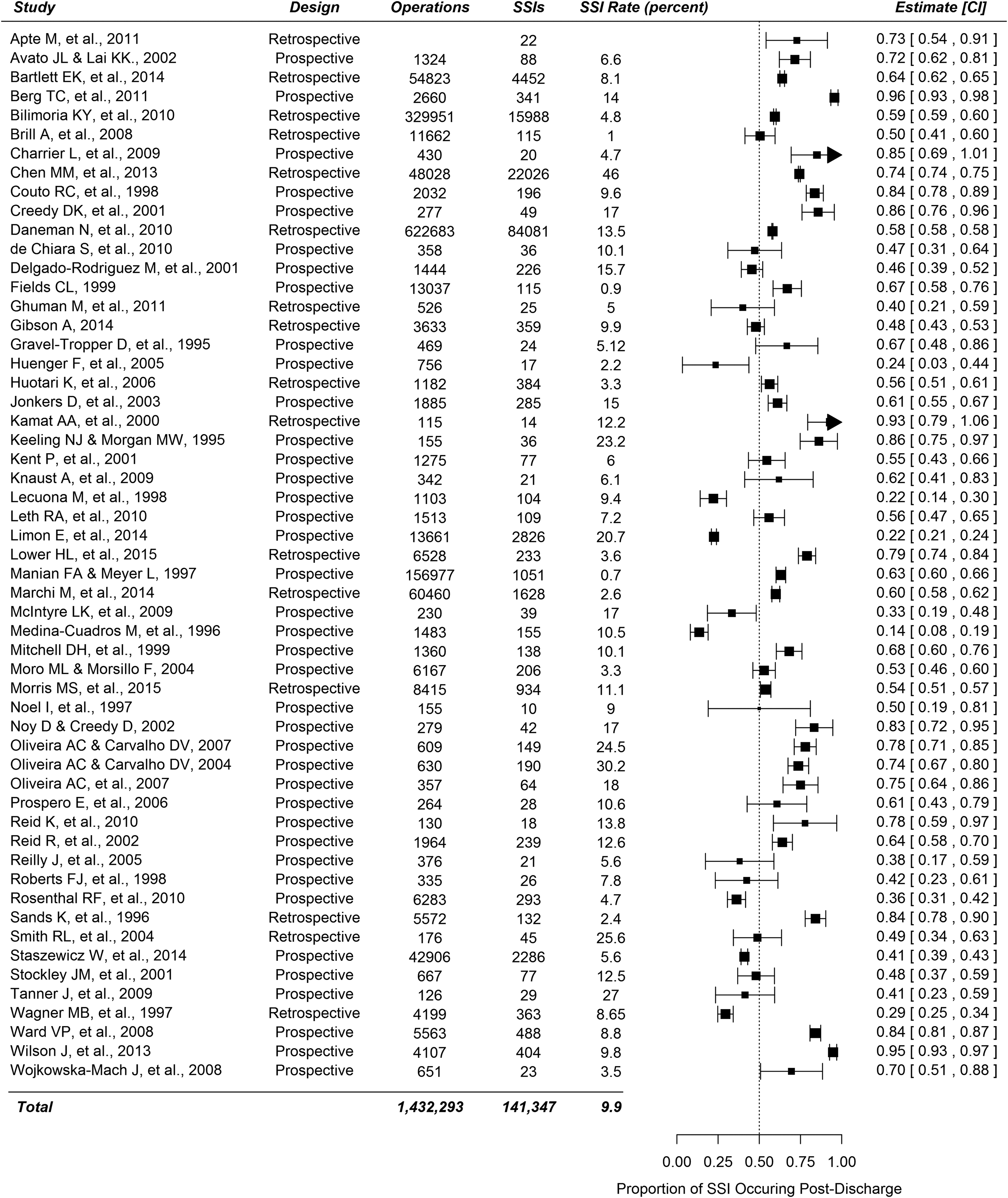
Forest plot of percentage of surgical site infections identified after discharge from the hospital.

Number of publications by country of origin identified during systematic literature review.
SSI = surgical site infection.
We were unable to create a random effects meta-analytical model for all 55 studies because tests of non-combinability showed that the observed proportions were highly heterogeneous (I2 = 99.66; Q = 8383; 54 degrees of freedom; p < 0.0001). Thus, a pooled estimate is not reported for these data; heterogeneity and SSI proportion may be assessed qualitatively in Fig. 1.
Although many studies did not utilize a specific surveillance system, five used the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP), two used the SSISS, two used the Norwegian Surveillance System for Healthcare Associated Infections (NOIS), two used the Australian Council of Healthcare Standards Clinical Indicators Program, and one study each used Polish, Italian, Swiss, and Finnish national surveillance systems. Most studies employed in-hospital surveillance, either alone or in combination with another national or regional surveillance system.
Of the 35 articles that explicitly reported the definition of SSI used for data collection, 32 (91%) employed the CDC or modified CDC criteria. Twenty-six (74%) used the strict CDC definition [8]. Six additional studies (17%) used modified CDC criteria, three of which used the SSISS/NINSS and one of which used the ECDC criteria. The three studies (9%) that did not use CDC or modified CDC criteria used ASEPSIS, ACHS, or a definition provided by the authors. Of the remaining 20 studies that did not report their formal definition of SSI, five were performed using NSQIP and presumably used CDC diagnostic criteria, whereas most of the remaining studies used a 30-day post-operative window for evaluating SSI without implantations (per CDC guidelines) but did not specifically state that the CDC diagnostic criteria were followed.
The three most common methods of follow-up were mailed or take-home questionnaires [24], telephone calls [20], and outpatient encounters/re-admissions [21]. Follow-up methods were variable; most studies employed a combination of in-patient and out-patient surveillance strategies, as well as chart reviews.
Thirteen sub-groups were identified, and each was analyzed independently using a random effects model for proportions. Three sub-groups—appendectomy, hernia repair, and vascular surgery—met the threshold for homogeneity (Cochran's Q p value >0.10). All other sub-groups had high heterogeneity, as quantified by the I2 test statistic. The results of sub-group analysis, namely the number of studies in each sub-group, the total number of SSIs, and the overall rate of infections, are presented in Fig. 3.
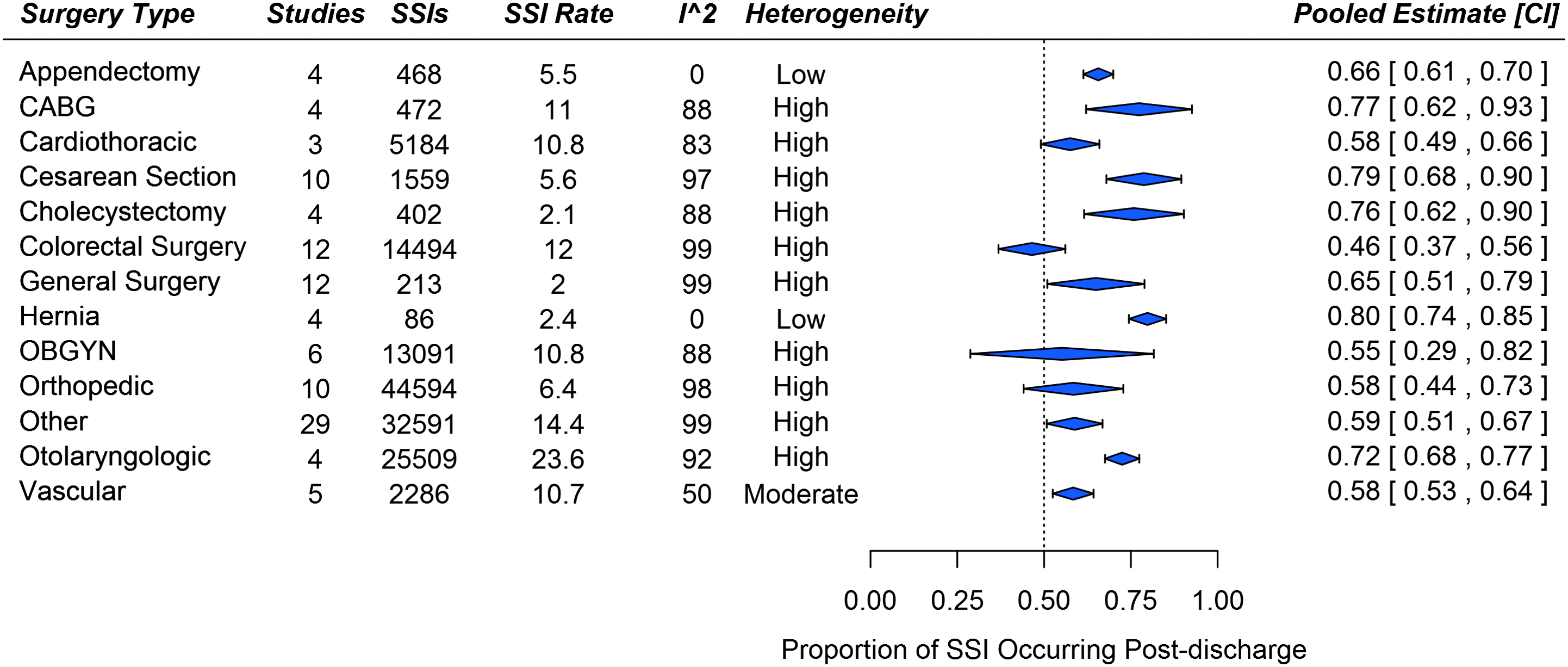
Post-discharge surgical site infections (SSI) by type of surgery. Color images available online at www.liebertpub.com/sur
The results of meta-regression using publication year, country of origin, and study design (prospective vs. retrospective) are shown in Table 2.
Boldface type indicates statistically significant difference.
CI = confidence interval; UK = United Kingdom; USA = United States.
Discussion
Proportion of SSIs identified after discharge
The proportion of all SSIs identified after discharge (60.1%) indicates that post-discharge infection is a major epidemiologic concern in the developed world.
Post-discharge SSI rates—especially relative to overall SSI rates—had a high rate of inter-study and intra-study variability. Meta-analysis of all 55 studies indicated a high degree of heterogeneity across the range of specialties and surgery types, which prevented reporting of a pooled estimate. This problem highlights the need to explore the factors influencing the degree of heterogeneity among studies, including specialty and the operation performed, which were explored in subsequent sub-group analysis.
Other potential moderators of post-discharge SSI proportion that were not modeled include the length of post-discharge hospital stay, the method of follow-up, study definition or subjective assessment of SSI, and the rate of follow-up. The entity (surgeon vs. infection control nurse vs. research team) diagnosing the SSI also has been suggested as a possible confounder [72].
In meta-regression, study design (retrospective vs. prospective) and the year of the study were not significant moderators of post-discharge SSI proportion among the 55 studies (p = 0.30 and 0.89, respectively). Country of origin was a statistically significant moderator for Germany, Spain, and Switzerland (p = 0.048, p < 0.0001, and p = 0.015, respectively) but was not statistically significant for 12 other countries.
Sub-group analysis
Restricted sub-group analysis decreased heterogeneity within only three of 13 sub-groups and did not eliminate heterogeneity in most cases (Fig. 3). Analysis by surgery type is a coarse control for several variables, including the risk of SSI during surgery, operative time, and the length of the in-patient hospital stay because of the relative international consistency in surgical management and operative approach in developed countries. Surprisingly, it was insufficient to explain the observed heterogeneity for most operation sub-types, which may be because the sub-groups were not sufficiently specific. From our results, we suggest that future meta-analysis of post-discharge SSI proportion focus on a specific operation (e.g., appendectomy) rather than a specialty (e.g., orthopedics) or all operations in order to yield proportion estimates that can be used for evaluation of post-discharge SSI risk in surgical practice.
However, even restriction by sub-type of surgery may be inadequate to conduct meta-analysis. Between-study variables such as patient age, surgeon experience, presence of residents, average American Society of Anesthesiologists (ASA) classification, average site classification, country of origin, and surveillance system could violate the assumption that individual study estimates are similar except for random variation. The necessity for restriction at the procedural level has been demonstrated for calculating SSI rates overall but has not yet been demonstrated for calculating the proportion of SSIs that are identified after discharge [73].
Sub-group analysis nevertheless identified three groups that were non-heterogeneous. Of these, the proportion of SSIs that occurred after discharge was 66% for appendectomies, 80% for hernia repairs, and 58% for vascular operations (Fig. 3). It is suspected that the high proportions of post-discharge SSIs after appendectomies and hernia repairs are attributable to the brevity of the post-operative hospital stays, with the exception being operations performed on higher-risk patients and those having more extensive open repairs. It is unclear why appendectomy, hernia repair, and vascular surgery are unique in having a relatively consistent proportion of SSIs after discharge. In particular, vascular surgery encompasses a plethora of procedures for which length of stay, surgical location, and clinical severity make homogeneity of infection rates unlikely; the observed homogeneity may be coincidental in this instance.
For every study included, the proportion of SSI identified after discharge was not adjusted for patients lost to followup. With the assumption that patients often are lost to followup because they do not experience a surgical complication, the modeled percentage of post-discharge SSI is likely an underestimation of the true proportion. Thus, the proportion of SSIs that are identified after discharge may be higher than 60.1%.
Surveillance and definition of SSI
Multiple surveillance systems were used to monitor SSI incidence systematically, and it is important that there is no international standard for methods of data collection used by these systems. This may explain the substantial differences in post-discharge proportions observed for Germany, Spain, and Switzerland during meta-regression. More importantly, it is a plausible source of heterogeneity among all studies and study sub-groups.
Definitional variation in “surgical site infection” also may be a source of heterogeneity. In addition to differences in standardized definitions of SSI, the CDC diagnostic criteria used in a majority of the studies incorporate ample “wiggle room” for subjective clinical judgment. Inter-rater variability in defining SSI may manifest as a difference in the way practitioners in different regions or surgical specialties define SSI. This lack of provider consensus has been highlighted as an explanation for SSI rate variation after colorectal surgery [72]. This variation will become increasingly problematic if SSI rates continue to be used as performance benchmarks, as noted by others [74].
Relations between post-discharge SSI and death
Although it is unclear whether identifying SSI after discharge reduces the morbidity or mortality rate, several studies underscore the potential impact of early SSI detection and antibiotic treatment. A retrospective cohort study of patients with Staphylococcus aureus bacteremia found that a delay in treatment by 45 h or more was associated with a higher overall rate of infection-related deaths and 3.8 times greater odds of death after adjusting for potential confounders [75]. This substantially increased risk of infection-related death also was accompanied by a longer hospital stay after bacteremia [75]. In a study of delayed antibiotic treatment of Pseudomonas aeruginosa by the same authors, a 50-hour delay in treatment was associated with a >2-fold increase in the 30-day mortality rate [76]. A study of orthopedic procedures found that delaying debridement of infected joints beyond 48 h yields lower success rates [77]. Finally, an analysis of 284,098 ambulatory surgical procedures concluded that earlier access to a clinician (e.g., using a telephone check-in prior to a two-week post-operative appointment) may help identify and treat SSIs early and reduce morbidity [78]. Thus, detection of post-discharge SSI represents a possible method to reduce the burden of infectious disease if it can prevent treatment delay.
Post-discharge SSI also may be a substantial source of morbidity in countries excluded from analysis. For example, in a study of 167 patients undergoing surgery in Phnom Penh, Cambodia, 24 developed SSI during their hospitalization, whereas 34 SSIs were identified after discharge using aggressive surveillance [79]. A Brazilian study of 222 surgical patients found that 62.2% of SSIs occurred after discharge [80]. Post-discharge SSI also represents a substantial proportion of SSI in hospitals in low-income countries such as Kenya, Sudan, and Tanzania [81–83].
Rate of SSI
The importance of SSI monitoring is made more apparent by national surveillance systems, which show that SSI is a common sequela of surgery. A 2011 National Healthcare Safety Network (NHSN) study found that 1.9% of operations resulted in an SSI [84]. A 2010 study of 284,000 selected low-risk out-patient procedures by the Agency for Healthcare Research and Quality found that the rate of clinically significant SSI after 30 d was 0.48% despite excluding in-patient and high-risk outpatient operations [78]. The overall rate of SSI in NHS hospitals in England from 2013–2014 was 1.4% [85].
Our study reported a higher overall rate of SSI (9.9%). This may be attributable to several factors. First, studies of operations and patient populations with historically high rates of SSI, such as colorectal surgery, were disproportionately represented in the chosen studies and may have introduced a selection bias. In general, SSIs are a substantial source of morbidity among high-risk patient populations, a phenomenon that is best characterized in placebo arms of randomized controlled trials of SSI prevention. The landmark trial comparing the effectiveness of ertapenem and cefotetan prophylaxis in elective colorectal surgery demonstrated an SSI rate of 26.2% in the cefotetan (usual care) group [86]. A 2011 study of the effect of an SSI prevention bundle in 211 subjects undergoing colorectal operations yielded a 36% incidence of SSI, with nearly half of the infections identified after the patient had left the hospital [87]. A 2013 randomized controlled trial of wound protector use in emergency and elective laparotomy in 760 patients at 21 U.K. hospitals showed an SSI rate of 25.4% in the control group [88]. Another study of wound protectors found that 20% of control patients developed SSI after open elective abdominal surgery [89]. These examples highlight the potential impact of high-risk operations on the calculation of the overall SSI rate.
The high rate of SSI reported in our study also may be the consequence of thorough case-finding, with surveillance via post-discharge telephone monitoring and adherence to recommended in-patient and out-patient follow-up protocols. Variation in case finding has been demonstrated even in large-scale national reporting systems. A comparative study of colon SSI rates reported by 16 hospitals using both the ACS NSQIP and the CDC's NHSN found that the rate reported by NHSN (5.7%) was significantly lower than that reported by NSQIP (13.5%) [90]. This variation was explained partially by the out-patient SSIs being missed under NHSN reporting practices [90].
Even standardized national surveillance systems are likely to underestimate the true rate of SSI, because hospitals lack a mechanism to capture all SSIs after patients are discharged, and retrospective chart review is prone to type II error. Beyond aggressive telephone follow-up, investigators have experimented with mobile platforms for post-discharge SSI diagnosis with limited but promising results [91,92].
In our study, authors tended to report high rates of follow-up in prospective cohort studies (see Fig. 1), theoretically increasing the success rate of case finding and reducing type II error. However, post-discharge case finding alone is not sufficient to explain the difference between the SSI rate in our study and those reported by national surveillance systems. Excluding all post-discharge infections, data obtained from our systematic search still showed an SSI rate of 3.9%, higher than that reported by national surveillance systems. Thus, our study is likely to have higher overall rates because of a combination of factors, including pre-discharge case finding, post-discharge case finding, high-risk patient populations, or the inclusion of international patient populations, whose baseline SSI rates may be higher.
This study lacked a mechanism to evaluate the severity of SSIs that were diagnosed. Thus, it is possible that the included studies reported more SSIs simply because more non-emergency cases were captured during the active surveillance period. Also, it is possible that the proportion of SSIs diagnosed after discharge increases with active surveillance but that aggressive search yields few clinically severe infections that would not otherwise have presented.
Conclusion
This is the first systematic review of the proportion of SSIs that occur after hospital discharge. Of 141,347 SSIs identified through our systematic search, a majority (60.1%) occurred after discharge, with proportions differing considerably between studies and by surgery type. This result suggests that post-discharge SSI is a substantial disease burden that demands greater attention and better management by surgeons and hospital staff. Post-discharge SSI is an international problem worthy of further examination using data quality screens and restriction by individual surgery type, as the factors moderating post-discharge SSI may be different according to the hospital location and the circumstances of the operation. This review will help in developing operation-specific guidelines to determine ideal follow-up intervals and novel monitoring strategies.
Footnotes
Author Disclosure Statement
None of the authors has any conflicts of interest to disclose.