
Abstract
Abstract
Background:
Median sternotomy, the most common means of accessing the heart for cardiac procedures, is associated with higher risk of surgical site infections (SSIs). A limited number of studies reporting the impact of medication use prior to cardiac surgery on the subsequent risk of SSIs usually focused on antibacterial prophylaxis. The objective of the current study was to evaluate the effect of medications prescribed commonly to cardiac patients on the risk of incident SSIs.
Methods:
The study analyzed data on consecutive cardiac surgery patients undergoing median sternotomy at a McGill University teaching hospital between April 1, 2011 and October 31, 2013. Exposure of interest was use of medications for heart disease and cardiovascular conditions in the seven days prior to surgery and those for comorbid conditions. The main outcome was SSIs occurring within 90 d after surgery. Univariate and multivariate logistic regression (adjusted odds ratio [AOR]) was used to evaluate the effect.
Results:
The cohort included 1,077 cardiac surgery patients, 79 of whom experienced SSIs within 90 d of surgery. The rates for sternal site infections and harvest site infections were 5.8 (95% confidence interval [CI]: 4.4–7.3) and 2.5 (95% CI: 1.4–3.7) per 100 procedures, respectively. The risk of SSI was increased with the pre-operative use of immunosuppressors/steroids (AOR 3.47, 95% CI: 1.27–9.52) and α-blockers (AOR 3.74, 95% CI: 1.21–1.47).
Conclusions:
Our findings support the effect of immunosuppressors/steroids on the risk of SSIs and add evidence to the previously reported association between the use of anti-hypertensive medications and subsequent development of infection/sepsis.
S
Surgical site infections after cardiac surgery are associated with substantial increases in hospitalization costs, length of in-hospital stays, and mortality [5–7]. Median sternotomy is the preferred and most common means of accessing the heart for such cardiac procedures as coronary artery bypass grafting (CABG) and valve surgeries. Nonetheless, it is associated with higher risk of SSIs, mechanical instability, and dehiscence [8].
A variety of factors of SSIs after cardiovascular surgery have been investigated at length [9–11]. However, there are a limited number of studies reporting the impact of medication use prior to cardiac surgery on the subsequent risk of SSIs, and studies scrutinizing drug use usually focus on antibacterial prophylaxis [12–14].
The objective of the current study was to evaluate the effect of medications prescribed commonly to cardiac patients and used up to seven days prior to surgery on the risk of incident SSIs in patients undergoing median sternotomy for cardiac procedures.
Patients and Methods
Study cohort
The Sir Mortimer B. Davis Jewish General Hospital (JGH) in Montreal, Canada, is a teaching hospital associated with McGill University. Each year, the hospital's cardiac surgery department performs interventions on approximately 500 individuals. Since 2009, the JGH has reported information to the Quebec Registry in Adult Cardiac Surgery (QRACS), a province-wide database established for evaluating the quality of patient care and specific outcomes after cardiac interventions. One important component of the QRACS is a post-discharge surveillance with follow-up period of up to one year. Designated health care professionals in the JGH's cardiac surgery department enter the data into the QRACS and conduct active post-discharge surveillance. There is an ongoing data quality review, including data verification, end study audit, and critical variables review.
A retrospective cohort study was conducted using the QRACS data collected on a consecutive cohort of adult cardiac surgery patients admitted to the JGH between April 1, 2011 and October 31, 2013. For this study, the patients were followed up to 90 d after the date of surgery for incident SSIs. Only those who underwent median sternotomy were included in the analysis.
Information on known potential patient- and procedure-related risk factors for SSIs [9–14] were extracted for the analysis, including sociodemographic and behavioral characteristics (gender, age, body mass index, smoking status), pre-surgery assessment of cardiac functions (left ventricular ejection fraction [LVEF]), development of cardiogenic shock), American Society of Anesthesiologists (ASA) scores, presence of severe comorbid conditions (diabetes, hypertension, chronic obstructive pulmonary disease [COPD], peripheral vascular disease [PVD], chronic infection), priority of surgery (elective versus emergency), surgery type (isolated CABG, isolated valve, CABG and valve), use of internal mammary artery, location from which the patient arrived prior to surgery, wait time for surgery, infection control procedures, time of antibiotic initiation, time and duration of surgery, minimum body temperature during the operation, and duration of mechanical ventilation.
Exposure
The exposure of interest was the reported use of selected medications seven days prior to the surgery. Medications of interest were those prescribed commonly to cardiac patients (medications for heart disease and cardiovascular conditions and those for comorbid conditions), namely: β-blockers, α-blockers, statins, angiotensin-converting enzyme (ACE) inhibitors, calcium channel blockers, nitroglycerin, vasopressors, diuretics, proton pump inhibitors (PPIs), bronchodilators, immunosuppressors/steroids, insulin, oral hypoglycemic agents, acetylsalicylic acid, clopidogrel, and other anti-platelet agents.
Patients were classified either as users of a particular medication if recorded in the registry or as non-users. Information on the dosages, duration of use, and indications was not available in the dataset.
Outcome
The main outcome of this study was SSIs occurring within 90 d after surgery. Surgical site infections were defined according to U.S. Centers for Disease Control and Prevention criteria [15], and were classified as superficial (skin or subcutaneous tissue) or complex (deep soft tissues and organ/space). Furthermore, infections were classified based on the time of detection (in-hospital versus post-discharge) and the site of incision (sternal and harvest site infections).
Statistical analysis
Continuous, categorical, and binary variables were summarized with medians (interquartile range [IQR]) and proportions. The SSI rates were calculated per 100 procedures. Unconditional univariate logistic regression was used to calculate odds ratios (OR) with 95% confidence intervals for each reported risk factor and for each medication of interest. Adjusted odds ratios (AOR) were calculated with a multivariate logistic regression model constructed from age and gender, the variables found significant in univariate analysis, and all medications of interest regardless of their significance in the univariate analysis.
For each risk factor separate categories were assigned for missing values. The data were analyzed using SAS 9.3 statistical software (SAS Institute, Cary, NC).
The JGH ethics review board granted ethics approval. Use of the QRACS data was approved by the Association des chirurgiens cardiovasculaires et thoraciques du Québec.
Results
From April 1, 2011 to October 31, 2013, 1,077 patients who underwent sternotomy were included in the study (Fig. 1) with a total of 835 harvest site incisions. Most patients were male (71.8%). The median age was 68.2 years. A majority (74.7%) were non-smokers and nearly one-third of all patients (30.6%) were obese. The most frequently reported comorbid conditions were hypertension (62.1%) and diabetes mellitus (31.4%). A chronic infection was present in 4.5% of patients, and the most prevalent were respiratory tract infections. The majority (99%) had ASA scores of III or IV (Table 1). Almost all patients (99.9%) received prophylactic antibiotics prior to surgery, mostly cefazolin (85.9%). Two-thirds (64.8%) of surgeries were performed in the morning.
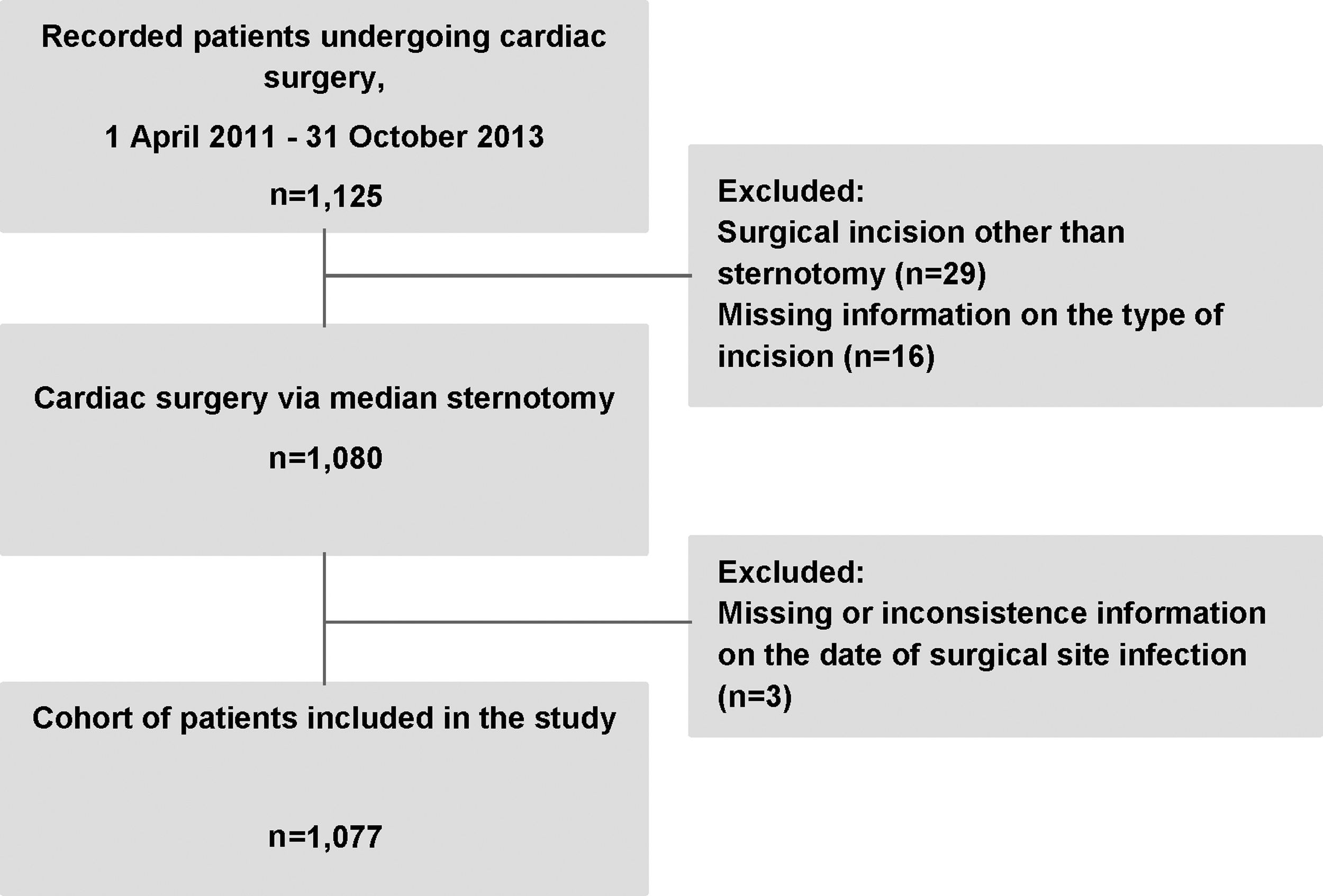
Flow of participants in the cohort study of per-operative medication use and subsequent risk of surgical site infections in patients undergoing cardiac surgery.
Forty-one values are missing.
Fifty-nine values are missing.
IQR = interquartile range; COPD = chronic obstructive pulmonary disease;
ASA class = American Society of Anesthesiologists physical classification system; LVEF = left ventricular ejection fraction; IQR = interquartile range.
Surgical site infections after cardiac surgery
A total of 79 patients experienced SSIs: 63 sternal site infections and 18 harvest site infections with rates of 5.8 (95% CI: 4.4–7.3) and 2.5 (95% CI: 1.4–3.7) per 100 procedures, respectively. Of sternal site infections, 31 were defined as complex (29 deep infections and two mediastinitis). All harvest site infections were leg harvest surgical site infections. Median time to the first SSI was 23 days (IQR: 14–32 days). More than 80% of SSIs, both superficial and complex, occurred after discharge from the hospital (Table 2). Pathogenic isolates were identified for 64 (79%) of all SSIs, and staphylococci were found in 90% of isolates (Table 3).
Among 787 patients with coronary surgery, 713 had saphenous veins harvesting.
CI = confidence interval.
Not mutually exclusive.
Prior medication use and risk factors for SSI
The most commonly prescribed medications were statins (77.6% of patients), PPIs (77.6%), β-blockers (62.6%), acetylsalicylic acid (57.4%), and ACE inhibitors (50.3%) (Table 4).
Unexposed as a reference group.
Adjusted for age, gender, American Society of Anesthesiologists (ASA) class, pre-operative hair removal, and all listed medications.
OR = odds ratio; CI = confidence interval.
In the univariate analysis of patient- and procedure-related risk factors, two variables were found to be associated with the risk of infection: ASA class of IV/V versus ASA class of II/III (crude OR 1.91, 95% CI: 1.19–3.06), and lack of pre-operative skin preparation, specifically hair removal (crude OR 2.34 95% CI: 1.17–4.70). The univariate analysis of medications used prior to the surgery identified that pre-operative use of α-blockers, insulin, immunosuppressors/steroids, and diuretics were associated with higher risk of SSI development (Table 4). After adjustment in the multivariate logistic regression model, only two medications retained their effect: the pre-operative use of immunosuppressors/steroids was associated with 3.5 times higher risk of SSIs (AOR 3.47, 95% CI: 1.27–9.52), and pre-operative use of α-blockers seemed to increase risk of SSIs more than 3.5 times (AOR 3.74, 95% CI: 1.21–11.47).
Discussion
Surgical site infections are common complications in patients undergoing median sternotomy for cardiac procedures [8]. We found the incidence of sternal site and harvest site infections was 5.8 (95% CI: 4.4–7.3) and 2.5 (95% CI: 1.4–3.7) per 100 procedures, respectively. The rate of harvest site infections in this population was in the lower limits of those reported previously [16–20]. This can in part be explained by the JGH's routine use of endoscopic saphenous vein graft preparation in myocardial revascularization procedures, a technique proven to reduce leg surgical site infections [21]. Conversely, the rate of SSIs was among the highest of those identified by other authors [17,18,20,22]. However, comparisons are to be made with caution because the study group, definitions of infections, and methodologies vary.
A majority (80%) of the infections in this study was diagnosed after discharge from the hospital. This is consistent with previous reports [17,18,23]. These findings confirm the importance of active post-discharge surveillance in monitoring of patients to detect SSIs in a timely fashion [24,25].
To evaluate the independent effect of medications used seven days prior to surgery on subsequent incident SSIs, we also examined the effect of baseline- and procedure-related SSI risk factors identified from the literature. Profiling characteristics such as age, gender, smoking, pre-existing diabetes mellitus, congestive heart failure, and obesity [9–11] were not predictors of SSI in this study population. Similarly, a history of infections was not associated with increased risk of SSI [26,27]. This may be explained partially by insufficient power in the analysis to detect the association because of small sample size and the presence of missing values on some risk factors, although for each characteristic the missing data did not exceed 4%.
The main objective of this study was to assess the independent effect of prior use of medications prescribed commonly to cardiac patients on the risk of SSI after surgery. We found α-blockers and immunosuppressors/steroids were independent predictors of SSIs. The association of immunosuppressors/steroids with higher rates of SSIs and other infections has been reported previously for patients after cardiac and other surgeries [28–30]. Immunosuppression has been hypothesized to mask inflammatory responses to infection, thus rendering early detection of infection more difficult and increasing the likelihood of severity and/or exacerbation [29]. However, in our study, the group “immunosuppressors/steroids” encompasses several classes of medications with a potentially distinct effect on infection development. For more precise risk estimates, one would need information of the length of exposure and indications for these drugs that were not available in our dataset.
Use of α-blockers as a risk factor for SSIs constitutes seemingly unique findings. However, there is evidence that some groups of anti-hypertensive medications, namely ACE inhibitors [31] and β-blockers [32], may be associated with increased risk of sepsis and sepsis-related outcomes. This association may be explained by the mechanism of action of β-blockers that involves prevention of tachycardia that, in turn, may impede recognition of an infection complication. Moreover, the vasodilatation induced by ACE inhibitors may worsen hemodynamic response to infection [31,32]. The finding of α-blockers effect on developing SSIs may be explained by the mechanism of vasodilation or by direct modulation of the immune system function [33]. This finding supports the potential association between anti-hypertensive medication use and infection/sepsis. However, our results should be replicated in other settings and with higher number of patients exposed to α-blockers.
We did not find any effect of statin use on incident SSI, although earlier studies demonstrated that statins were associated with reduced risk of sepsis in patients with cardiovascular disease [34], and may be protective against postoperative infections following cardiac surgery [35]. A recent meta-analysis, however, did not provide statistically significant evidences of association between pre-operative statin use and post-operative infectious complications [36]. Nonetheless, a Cochrane Systematic Review found that statins may benefit patients undergoing cardiac surgery by means of reduction of risk of post-operative atrial fibrillation and shortening post-operative intensive care unit stay [37].
The study limitations include missing information on many variables of interest. Furthermore, the relatively small sample size limits the power of estimations and it is possible that some associations are attributable to random error. Although the results yielded by the study are applicable to the JGH, they lack generalizability because of the specificity of the study population and its conditions.
Additional research with larger populations would prove valuable in ascertaining a better understanding of the risks or benefits of pre-operative medication use and SSI outcomes in order to improve surgical patient care and maximize service delivery.
Footnotes
Author Disclosure Statement
No competing financial interests exist.