
Abstract
Abstract
Background:
Discoveries regarding the basic mechanisms underlying malignant disease, rheumatologic disorders, and autoimmune diseases have led to the development of many new therapeutic modalities that target components of the immune system. Most of these are antibodies or fusion proteins that interfere with components of the immune response that are playing both pathological and protective roles, resulting in variable degrees of immune suppression and a higher risk of infectious complications.
Methods:
Review of the English-language literature.
Results:
As these modalities are often used in combination with more traditional methods of immune suppression (e.g., corticosteroids), an increasing spectrum of infection is being encountered by clinicians. Febrile neutropenia requires rapid assessment and initiation of empiric broad-spectrum antimicrobial therapy. Persistence despite this therapy should prompt further investigation for drug-resistant bacteria and invasive fungal disease. Important pathogens to consider in patients with neutropenia, chronic steroid exposure, or underlying gastrointestinal malignant diseases include fungi (Candida, Aspergillus) and atypical bacteria (Nocardia, Clostridium septicum).
Conclusions:
This review focuses on observations regarding the greater risk of infections associated with many of these new biological modalities, as well as some specific infectious complications that may be encountered more commonly by the surgical consultant.
Infections and Neutropenia
E
Definitions
Fever here is defined as a single oral temperature >101°F (38.3°C) or an oral temperature >100.4°F (38°C) sustained for at least one h. Neutropenia is defined as an absolute neutrophil count <1,000/mcL of blood, with absolute neutropenia being <500 neutrophils/mcL. Febrile neutropenia (FN) is fever during the course of neutropenia.
Febrile neutropenia
Neutropenia is most commonly the result of the administration of cytotoxic chemotherapeutic agents during treatment for malignant disease but may occur as part of an underlying disease (e.g., acute myelogenous leukemia), other cytotoxic therapies (e.g., anti-metabolite drugs such as methotrexate or azathioprine), or as a consequence of radiation therapy. Generally, the agents used as chemotherapy for solid cancers are associated with short durations of neutropenia (<7–10 days) and less severe neutrophil nadirs, such that relative neutropenia may be the severest extent of immune suppression, followed by full neutrophil recovery. In contrast, chemotherapies used to treat hematologic cancers commonly are associated with absolute neutropenia and possibly with severe, prolonged neutropenia (>10 d of <100 neutrophils/mcL).
Febrile neutropenia may complicate the therapy of solid tumors in 10%–50% of cases, whereas this condition occurs in >80% of patients undergoing therapy for hematologic cancers [2]. The etiology of FN differs, largely because of the heterogeneity of the patient populations included in epidemiologic studies of this condition. Infections account for 20%–30% of FN cases, with the majority identifiable as bacterial or fungal [2]. Bacterial infections are more common, and the duration and depth (nadir) of neutropenia are important risk factors associated with an increasing risk for invasive fungal infections (IFIs), especially those caused by molds [1,2].
The enteric gram-negative flora (e.g., Escherichia coli, Klebsiella spp.), mucosal gram-positive flora (e.g., viridans streptococci), and Pseudomonas aeruginosa are the bacteria most commonly isolated from patients with FN, although staphylococci are playing a greater role in recent studies, especially in patients with indwelling catheters or other biomedical devices [3]. Enterococci, especially vancomycin-resistant enterococci (VRE), also are important pathogens in FN and should be suspected in patients failing to respond to antimicrobial agents that lack activity against VRE or those having extensive antimicrobial exposure prior to developing FN.
Colonization with multi-drug resistant (MDR) pathogens, such as methicillin-resistant Staphylococcus aureus (MRSA), VRE, extended-spectrum beta-lactamase (ESBL)-producing organisms, Acinetobacter spp., or carbapenem-resistant Enterobacteriaceae, should be accounted for when selecting empiric antimicrobial therapy for FN patients. An important bacterium to keep in mind is Clostridium difficile, as these patients commonly have had extensive exposure to antimicrobial agents, a major risk factor for infection with this organism, and diarrhea is a common side effect of chemotherapeutic agents, leading to a potential for underdiagnosis or a delay in diagnosis of infection with this deadly pathogen.
Typhlitis
Among the many conditions to be considered in the differential diagnosis of diarrhea in the neutropenic host is the syndrome known as typhlitis. This disease, often referred to as neutropenic enterocolitis, is characterized by clinical and radiographic signs and symptoms occurring collectively in a neutropenic patient. The clinical features are fever and abdominal pain (typically in the right lower quadrant) and may include additional symptoms suggesting gastrointestinal distress such as nausea, vomiting, and diarrhea. Radiographically, imaging of the abdomen demonstrates thickening of the ileocecal intestinal wall and distention of the same and may show additional findings such as obstruction, perforation, or abscess formation. Computed tomographic or ultrasound imaging may also reveal an inflammatory mass involving the cecum.
The extent of bowel wall thickening (BWT) is prognostic, with BWT >10 mm associated with worse clinical outcomes [4]. Typhlitis commonly is accompanied by bacteremia with enteric pathogens, perhaps secondary to translocation of gut microbes across the inflamed wall. The pathogenesis of typhlitis probably is multifactorial, with increased inflammation in the cecum triggered by mucosal damage from chemotherapeutic agents, pro-inflammatory signaling via innate pattern recognition receptors (e.g., Toll-like receptors), and poor clearance of translocating microbes because of the neutropenic state [4].
Empiric antimicrobial therapy in patients with typhlitis should include agents with activity against enteric pathogens (e.g., E. coli, Klebsiella spp., enterococci) and gut anaerobes (e.g., Bacteroides fragilis). Surgical intervention sometimes is required to address specific complications such as perforation, abscess, or necrotic bowel. Necrotic mucosa may be present in typhlitis even when the serosa appears normal [4].
Fungal Infections in Febrile Neutropenia
As mentioned previously, the duration and depth of neutropenia are both risk factors and predictors for IFIs in neutropenic patients. Such infections usually are considered when fever persists in a neutropenic host despite treatment with broad-spectrum antibiotics. The incidence of IFI in neutropenic patients differs widely in published studies, ranging from 1%–35% [5–8]. This variability is a reflection of the many underlying factors that influence individual risk for IFIs, such as the type of malignant disease, the type of chemotherapy, colonization status, exposure history, use of antibacterial or antifungal agents, monocytopenia, use of parenteral nutrition, and recent abdominal surgery [9,10].
Infections caused by Candida and Aspergillus spp. are the most common among neutropenic patients [11]. Less common causative fungi are Cryptococcus neoformans, other endemic fungi (Histoplasma capsulatum, Blastomyces dermatididis, Coccidioides immitis), agents of mucormycosis (e.g., Rhizopus spp.), Trichosporon spp., and Fusarium spp. Candida albicans remains the most commonly isolated pathogenic yeast in most studies of IFIs in neutropenic patients, accounting for 20%–50% of Candida species in blood cultures [11,12]. However, non-albicans Candida species such as C. glabrata, C. parapsilosis, C. tropicalis, C. krusei, and C. lusitaniae have become more frequent causes of IFI over the past decade, with several important species accounting for growing “slices of the IFI pie” [13]. Candida glabrata often is the second or third most commonly isolated pathogenic Candida spp. and may be relatively or completely resistant to fluconazole.
Relative fluconazole resistance in C. glabrata, termed dose-dependent susceptibility, is mediated by efflux pumps that remove fluconazole from the cytosol of these yeasts, thus increasing the minimum inhibitory concentration of fluconazole required to inhibit yeast growth [14]. A smaller percentage (∼1–5%) of C. glabrata isolates is completely resistant to fluconazole, usually because of alteration of the lanosterol-14α-demethylase target of the drug [14]. Another important Candida species that is completely resistant to fluconazole and is more commonly isolated from patients with hematologic malignancies is C. krusei [13].
Diagnosis of IFIs
Invasive fungal infections are notoriously difficult to diagnose for a number of reasons, including failure to consider the possibility, difficulties in obtaining diagnostic specimens, interference from colonizing flora, and the poor sensitivity of many diagnostic tests employed in this venture. For example, routine blood cultures have a sensitivity of 21%–71% for candidemia, and these cultures are virtually useless for the diagnosis of invasive aspergillosis [15]. Two newer assays have become available for the diagnosis of IFIs and are being used routinely in clinical practice: (1) The Aspergillus galactomannan (GM) antigen assay; and 2) the (1,3)-β-D-glucan assay (BDG).
The Aspergillus GM antigen assay detects galactomannan in biologic specimens via an immunoenzymatic sandwich microplate assay. Galactomannan is released by growing Aspergillus hyphae but is also a component of many biological products, so there is some capacity for contamination or false-positive test results. The test result is expressed as a unit-less index, with a positive value ≥0.5. The specificity of this assay for IFIs caused by Aspergillus species is high (90%–97%) because of the use of a monoclonal antibody directed against Aspergillus galactomannan and by testing specimens taken from sites not normally colonized with these organisms (e.g., serum, cerebrospinal fluid [CSF]); specificity is decreased when testing specimens from sites that may be colonized (e.g., bronchoalveolar lavage fluid) [16]. The sensitivity of this assay differs according to the specimen type as well, with a range of 54%–75% for invasive aspergillosis when serum testing is performed and 72%–92% when BAL fluid is tested [16]. Therapy with anti-mold agents decreases the sensitivity of the GM assay. False-positive results may be observed in patients receiving some antibacterial agents (piperacillin-tazobactam) or with infections caused by mold species that express similar or identical galactomannan molecules (e.g., Penicillium and Paecilomyces spp.) [17].
The BDG assay utilizes the ultrasensitive coagulation cascade present in horseshoe crabs to detect (1,3)-β-D-glucan in biologic specimens. Many fungi produce this glucan during growth, including Histoplasma capsulatum, Pneumocystis jirovecii, Candida, and Aspergillus spp. However, several medically important fungi do not shed this glucan and so cannot be detected using this assay, including Cryptococcus spp., Blastomyces dermatitidis, and the agents of mucormycosis. The BDG assay has been used most commonly to test serum specimens via enzyme immunoassay and provides an absolute concentration of the organism. Results are reported as negative (<60 pg/mL), indeterminate (60–79 pg/mL), or positive (≥80 pg/mL). False-positive BDG tests have been reported with concurrent use of some antibacterial agents such as amoxicillin-clavulanic acid, by the presence of mucositis, hemodialysis using cellulose acetate membranes, use of some fractionated blood products (e.g., immune globulin), and cellulose-containing surgical dressings. The sensitivity of the BDG assay for IFI is better than that of blood culture for candidemia (55%–73%) and is high (>90%) for P. jirovecii pneumonia (PJP), but the specificity is decreased because of the large array of fungi that produce this antigen [18,19].
Other antigen assays that may be useful when investigating IFIs include the cryptococcal antigen assay for use with serum or CSF and the Histoplasma and Blastomyces assays for serum and urine. These latter antigens are excreted in the urine, and the sensitivity of antigen testing increases with fungal burden, such that patients with disseminated fungal infections are readily identified, whereas those with disease limited to the port of entry (e.g., pulmonary disease) may be missed. The Histoplasma and Blastomyces antigens are cross-reactive in immunoassays, thus decreasing the specificity of these tests when attempting to diagnose specific endemic mycoses [20].
Invasive Aspergillosis in Febrile Neutropenia
Whereas Candida spp. are the most common fungi causing IFIs in patients with febrile neutropenia, Aspergillus infections are associated with a higher mortality rate, particularly when there is a delay in diagnosis [11]. Aspergillus infections frequently manifest in structures of the upper and lower respiratory tract, and the most common clinical syndromes are fungal sinusitis and invasive pulmonary aspergillosis (IPA). The signs and symptoms of Aspergillus infection are nonspecific and mirror bacterial, viral, and fungal infections at these sites (e.g., cough, fever, dyspnea). Some clinical features suggest the possibility of an IFI, such as fever persisting despite broad-spectrum antibacterial therapy, hemoptysis, angioinvasion leading to tissue necrosis, or neuroinvasion with focal abnormalities on the neurologic examination.
Imaging of the sinuses and thorax via computed tomography (CT) may yield valuable information regarding the possibility of an IFI in patients with persistent febrile neutropenia. Fungal sinusitis, including disease caused by Aspergillus spp., may demonstrate local invasion of the bony structures surrounding the paranasal sinuses, prompting further investigation via nasopharyngoscopy. The IFIs causing pneumonia may be indistinguishable from lobar bacterial pneumonia. However, some abnormalities on chest CT favor a diagnosis of IFI: (1) Macronodules (solid densities >1 cm, Fig. 1) with or without cavitation; (2) the halo sign (macronodule surrounded by a ground-glass infiltrate); (3) a reverse halo sign (a nodule with ground-glass interior surrounded by a solid rim); or (4) an air-crescent sign (a late finding, often after recovery of the neutrophil concentration, with separation of a portion of the interior of a macronodule, leaving a rim of air around the separated necrotic tissue) [21]. The Aspergillus GM antigen assay may be useful as an adjunct diagnostic aid, as discussed above. Growth of Aspergillus from a respiratory specimen (sputum, BAL fluid) should increase suspicion for IPA but does not provide definitive proof of this infection. Lung biopsy (via a transbronchial route, CT-guided, video-assisted thoracoscopy, or open) can provide direct evidence of IPA by providing tissue for histopathologic examination or culture.
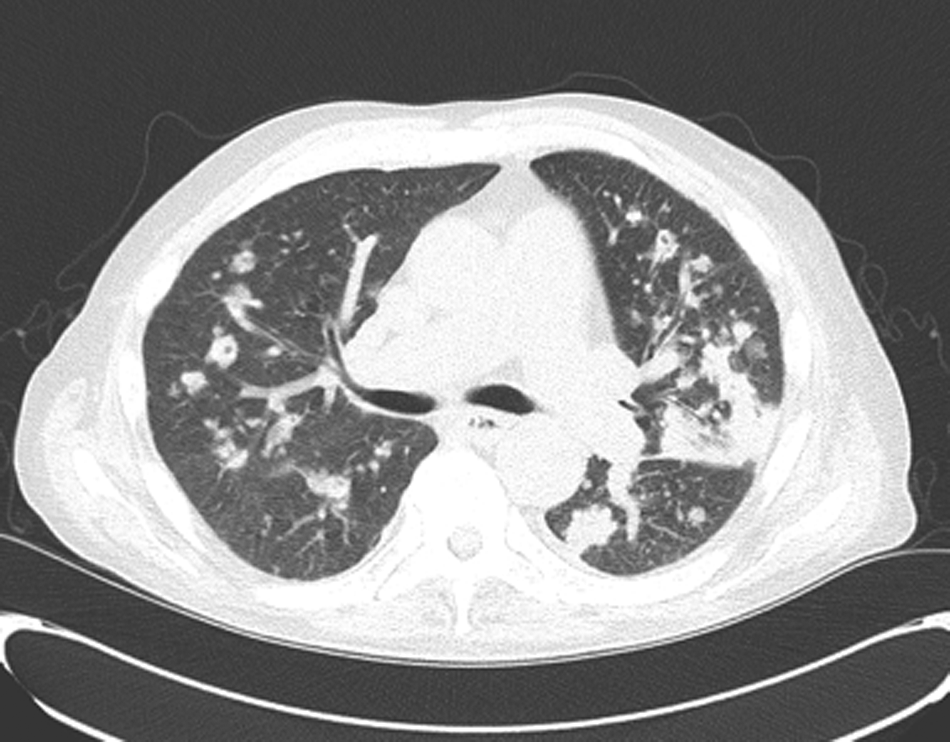
Abnormalities on chest computed tomography scan that favor diagnosis of invasive fungal infection.
The decision to initiate therapy for IPA (or Aspergillus sinusitis) should not be based on obtaining a definitive diagnosis, as this usually is not feasible in patients with febrile neutropenia. Rather, therapy should be initiated based on the degree of clinical suspicion for IFI and knowledge of the high mortality rate associated with delayed diagnosis. The current best therapy for IPA is voriconazole; alternatives such as amphotericin B, itraconazole, posaconazole, and the echinocandins may be suboptimal [22]. Although echinocandins have activity against Aspergillus spp., they are not active against many other invasive molds.
Other Infections To Consider in Immunocompromised Patients
The spectrum of potential pathogens causing infections in immunocompromised patients is too large to review in a single paper, but there are two additional pathogens of interest to a surgical audience that will be addressed here. The first (Nocardia) can mimic IFIs in neutropenic hosts but may present in non-neutropenic patients with other forms of immune suppression, such as chronic steroid exposure. The second (Clostridium septicum) is an emerging infection that appears disproportionately in immunocompromised patients and often requires surgical intervention for proper treatment.
Nocardia infections
Nocardia spp. are ubiquitous, gram-positive, environmental bacilli that cause infections predominantly in immunocompromised hosts. There are a large number of Nocardia spp. that have been described as causes of human infection, and identification of the species is important because of the wide variability in antimicrobial susceptibility. The route of infection for Nocardia usually is inhalational but also includes percutaneous (traumatic inoculation) and device-related routes (e.g., intravenous catheters). Clinical presentations are those of the primary site of infection, such as pneumonia or soft tissue infection but may follow a “lung–brain” pattern, as Nocardia have a propensity for dissemination to the central nervous system and formation of brain abscesses.
Computed tomographic imaging of the chest may demonstrate macronodules, ground-glass infiltrates, or both; and the nodular infiltrates may form cavities. Biologic specimens may show beaded, branching, gram-positive bacilli (Fig. 2) suggestive of actinomycotic infection. Unlike Actinomyces, Nocardia usually is weakly acid-fast. As noted earlier, antimicrobial therapy for Nocardia infections is species-specific, so every attempt should be made to isolate these bacteria and submit specimens for culture.

Beaded, branching, gram-positive bacilli characteristic of Nocardia.
Several empiric antimicrobial regimens will cover most, if not all, of the commonly invasive Nocardia species: (1) trimethoprim-sulfamethoxazole; (2) imipenem plus amikacin; and (3) linezolid. When Nocardia infections are suspected or confirmed, imaging of the brain should be done to exclude central nervous system involvement, usually in the form of a brain abscess. The presence of brain involvement should prompt evaluation for drainage of abscesses and use of antimicrobial agents that penetrate into the central nervous system (e.g., trimethoprim-sulfamethoxazole). The duration of therapy for most Nocardia infections is long, typically 6–12 months, and should be accomplished in conjunction with infectious disease consultation.
Clostridium septicum infections
Clostridium septicum is a spore-forming, gram-positive bacilli that is part of the endogenous human bacterial flora. All pathogenic clostridia, including C. septicum, produce protein exotoxins that facilitate infection. Clostridium septicum infections have been described most often in patients with neutropenia, gastrointestinal malignant diseases, gastrointestinal operations, or a history of chemotherapy or radiation. The most common clinical syndrome associated with C. septicum infection is bacteremia, and there is a notable association between bacteremia, colon cancer, and mycotic aneurysms [23].
Unlike other pathogenic clostridia, C. septicum is aerotolerant and may cause infections in normal human tissues that have not been devascularized or deprived of oxygen. As a consequence of this aerotolerance, C. septicum is able to cause spontaneous, non-traumatic gas gangrene. This disease may mimic necrotizing fasciitis and carries a high mortality rate (70%–100%), with patients often dying within 24 h of becoming ill [23].
The treatment of necrotizing infections caused by this organism is emergency surgical debridement, accompanied by adjunctive antimicrobial therapy. Non-necrotizing infections may be treated with antimicrobial therapy alone, with the preferred regimen including penicillin plus clindamycin or tetracycline to reduce toxin synthesis [23]. Alternatives include other antimicrobial agents with anaerobic activity (carbapenems, piperacillin, ticarcillin, metronidazole), but there are no controlled trials to inform us regarding the optimal drug regimen.
Antibody-Related Biological Therapies and Infections
The past decade has witnessed an explosion in the availability of antibody-based or antibody-related biologic therapies for a wide variety of diseases. Many of these agents are directed against components of the immune system and, as expected, are associated with a higher risk of infection. Some of these agents are associated with a higher risk for specific infections, whereas others have been associated with a general increase in infectious complications. Clinicians need to be aware of these associations to remain vigilant for infectious complications and initiate the appropriate diagnostic and therapeutic process as early as possible. Table 1 displays many of the more commonly encountered or well-described biologic therapies and their associated infections.
Abbreviations: CMV = cytomegalovirus; HSV = herpes simplex virus; mAb = monoclonal antibody; TNF = tumor necrosis factor; VZV = varicella zoster virus.
Summary
Infections are an unfortunate, but common, complication of compromised immunity. Knowledge of the relevant clinical syndromes, pathogens, diagnostics, and therapeutics related to the immunocompromised state is critical to providing excellent clinical care to these patients. Febrile neutropenia is a frequently encountered condition that requires rapid assessment and initiation of empiric broad-spectrum antimicrobial therapy directed against the most common bacterial pathogens associated with this condition. Persistence of febrile neutropenia despite this therapy should prompt further investigation for drug-resistant bacteria and invasive fungal disease. Important pathogens to consider in patients with neutropenia, chronic steroid exposure, or underlying gastrointestinal malignant diseases include fungi (Candida, Aspergillus) and atypical bacteria (Nocardia, Clostridium septicum). Finally, clinicians are likely to encounter patients who have received antibody-related biologic therapies and should consider the potential infectious complications that may arise in these populations.
Footnotes
Author Disclosure Statement
Dr. Tessier has no conflicts of interest to disclose.