
Abstract
Abstract
Background:
Patients who survive the early phases of major sepsis and trauma can have greater susceptibility to nosocomial infection later. One cause may be impaired monocyte function, which can leave the patient at risk of overwhelming sepsis and multi-organ dysfunction. Efforts to target this immune defect have been fraught with challenges, with many questions unanswered. We summarized the past and current and likely future therapeutic approaches to augmentation of monocyte function in the surgical patient.
Methods:
A literature search was conducted using PubMed to determine the evidence to date for immunoadjuvant therapy specifically for monocyte impairment. The search terms were “monocyte,” “immunoparalysis,” “tolerance,” and “deactivation” cross-referenced with “trauma,” “major surgery,” and “sepsis.” We supplemented our search with “interferon-γ,” “granulocyte colony-stimulating factor” (G-CSF), and “granulocyte-macrophage colony-stimulating factor” (GM-CSF), known agents used for this purpose. We limited our findings to clinical trials in human beings. Relevant currently registered trials relating to impaired monocyte function also were included.
Results:
Interferon-γ appears to be the most commonly studied therapeutic agent to augment monocyte function, followed in decreasing order by GM-CSF and G-CSF. Studies were heterogeneous, generally under-powered, and enrolled few target patients with documented monocyte impairment. Finally, current studies are focusing on personalized therapy in order to treat those with monocyte impairment, with attention to programmed cell death protein 1 (PD-1) and programmed cell death ligand (PD-L1) as both markers and therapeutic targets.
Conclusion:
Early studies have been promising in identifying patients who are likely to benefit from monocyte augmentation; i.e., those with low HLA-DR or ex-vivo tumor necrosis factor (TNF)-α production. The surgeon remains incompletely equipped to enhance monocyte function consistently and specifically in order to reduce the mortality rate. Although there is little evidence to support the routine use of any of these immunotherapies, the issues of patient selection, timing of administration, and treatment duration have hampered any true answers to this important clinical problem. The challenge remains in identifying the right patients, at the right time, to receive the right therapy.
S
A major flaw in many of these studies, including our own, is the failure to define what is the most appropriate threshold to determine impaired monocyte function and the most meaningful duration of that impairment. Although low monocyte HLA-DR expression is cited commonly as the most useful predictive marker of surgical infection, not all reports have agreed, in part because of a lack of standardization among laboratories. Newer methods of calibration to calculate antibodies per cell have somewhat improved this measurement [2,3].
Various studies have aimed to boost immune function by increasing the proportion of normal, activated monocytes (such as with interferon-γ, granulocyte–macrophage colony-stimulating factor, or other agents), but these measures have thus far failed to produce a consistent reduction in the mortality rate [4–6]. One of the biggest challenges has been in defining and identifying an appropriate subset of patients, a problem that has in parallel stimulated the field of endotoxin tolerance research [7,8]. This principle is illustrated in Figure 1, where the previously stimulated monocytes (by LPS) have reduced responsiveness to a further LPS challenge. Again, the role of potential therapy is demonstrated in Figure 2, an in-vivo model of endotoxin tolerance. Here, one can see the augmentation of tumor necrosis factor (TNF)-α production when interferon (IFN)-γ is given. This review aims to address the evidence and lessons learned from previous trials of therapies aimed at restoring monocyte function and to discuss current and future approaches to a clinically important conundrum.
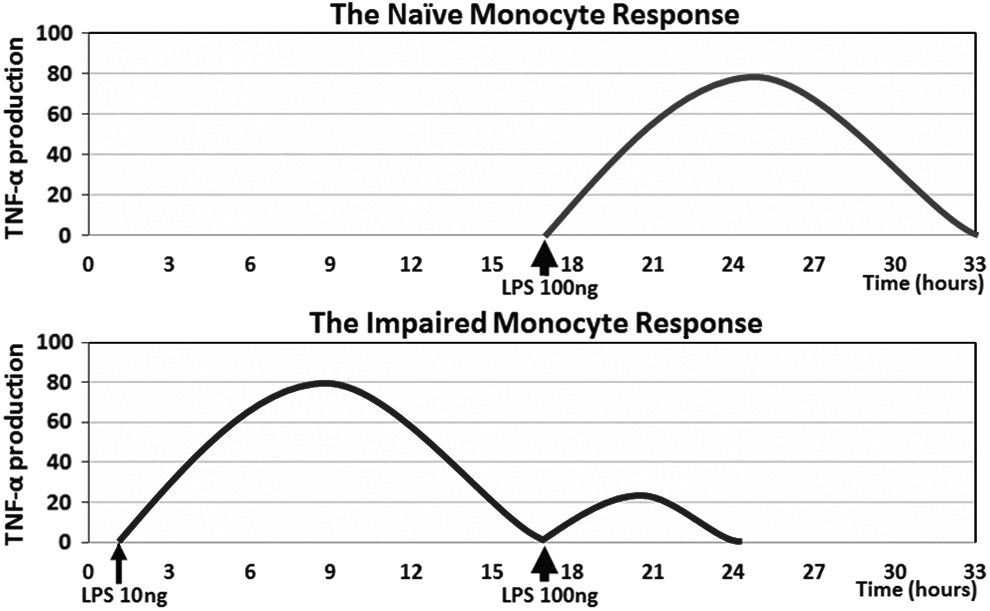
Principle of in vitro studies of impaired monocytes using relative units of TNF-alpha production.

Human in vivo monocyte impairment in response to subcutaneous lipopolysaccharide (LPS). Compared with the first LPS dose (day 1), there is decreased monocyte responsiveness of tumor necrosis factor-α production, as well as of interleukin (IL)-6 and IL-10 in response to a second dose (day 7). Note partial reversal with interferon-γ and granulocyte–macrophage colony-stimulating factor when given between doses. Adapted from Leentjens et al. [16]. (With permission from the American Thoracic Society. ©2015 American Thoracic Society.)
Materials and Methods
A literature search was carried out using the PubMed, MEDLINE, and Cochrane databases using the terms “monocyte,” “impairment,” “endotoxin tolerance,” “deactivation,” “HLA-DR,” and “immunoparalysis.” They were cross-referenced against “trauma,” “sepsis,” “infection,” and “surgery.” Combinations of the above were used. The search was supplemented using the terms “interferon-γ,” “granulocyte–macrophage colony-stimulating factor,” (GM-CSF) and “granulocyte colony-stimulating factor” (G-CSF), agents potentially targeting monocyte impairment. Relevant results of selected papers are discussed in chronological order below, grouped by the immune adjuvant used.
Interferon-γ
Polk et al., Am J Surg 1992 (Trauma) [6]
Interferon-γ has been used safely in human beings for other clinical indications such as malignant disease. A narrowly focused pilot clinical trial in 15 patients who were treated with IFN-γ after major trauma demonstrated increased monocyte HLA-DR expression. This was followed by a larger randomized controlled trial at four medical centers that enrolled 201 patients with an injury severity score exceeding 20 and bacterial contamination. Recombinant IFN-γ (100 mcg) was given subcutaneously for 10 consecutive days. Expression of HLA-DR was augmented for the duration of IFN-γ treatment; however, the concentration quickly returned to that of the placebo group after treatment cessation on day 10 (Fig. 3). Patients were followed for 90 d, and it was noted that a quarter of the infections occurred after day 11. Fewer patients required an operation for infection, and the mortality rate appeared to be lower in the treatment group, although this difference was not statistically significant. Fever was experienced by 93% of the treated patients as a side effect of therapy. The authors later concluded that future trials might consider administering doses on alternate days over a longer period, with the aim of reducing febrile side effects yet extending therapy [1]. Interestingly, this idea was a keystone of concurrent parallel work by Dries et al. [4].
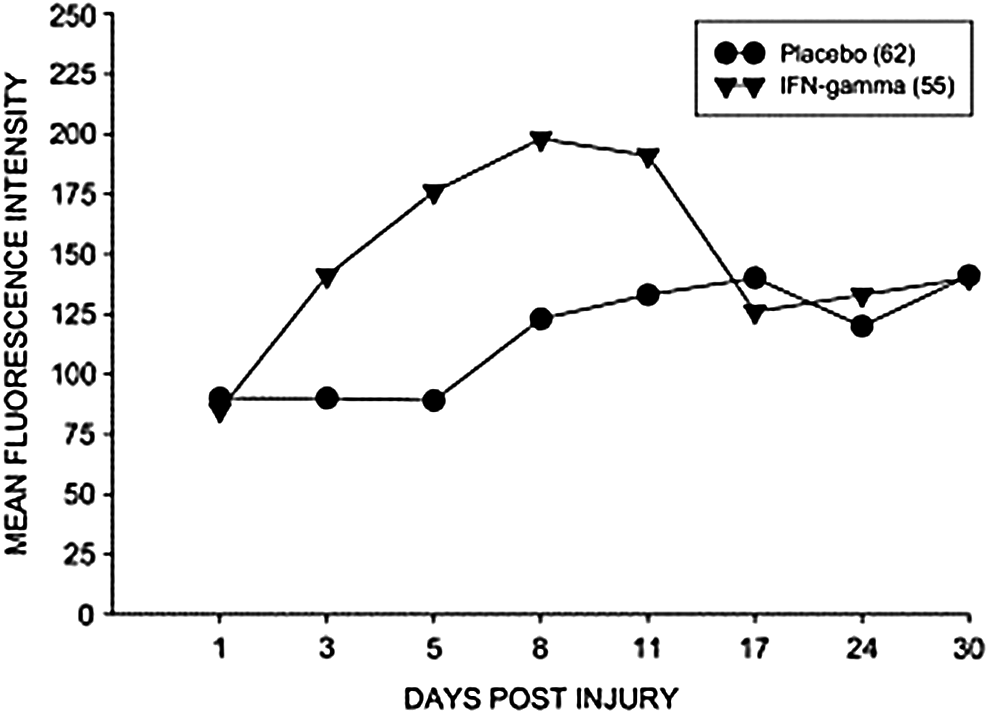
For the duration of treatment, the interferon-Ύ-treated group (inverted triangles) benefits from increased monocyte HLA-DR expression (mean fluorescence intensity) compared with the placebo group (black circles). However, note rapid return of monocyte HLA-DR to an amount similar to that in the placebo group after the final dose of the regimen (given on day 10 post-injury). (Reprinted with permission from Polk et al. [6].)
Dries et al., Arch Surg 1994 (Trauma) [4]
A second randomized trial was undertaken in parallel, with 416 patients across nine medical centers randomized to IFN-γ or placebo. Again, severe trauma was the indication, but the major difference in design was that doses were given on alternate days for 20 d rather than 10. The differences between this and the previous trial are discussed at length elsewhere [9]. The major findings were that all-cause mortality was similar, but infection-related mortality were lower in the treatment group (3% with IFN-γ vs. 9% with placebo). The authors noted an unusually high mortality rate in the placebo group in a single hospital that contributed to a large imbalance. Interestingly, this treatment group did have a longer intensive care unit (ICU) stay than the placebo group, perhaps attributable to investigation of the febrile reaction to therapy. Solving intellectually or technically the excess death rates in the placebo arm in the leading enrolling institutions has not been accomplished.
Docke et al., Nature Medicine 1997 (Sepsis) [5]
In 1997, Docke et al. used IFN-γ in nine patients with sepsis and impaired monocyte function. “Monocyte deactivation” was defined as <30% HLA-DR-positive monocytes for two consecutive days in the context of Bone's criteria for sepsis [10]. Therapy was continued until HLA-DR expression was restored for two consecutive days or eight days total. Therapy also boosted ex-vivo TNF-α production compared with 26 historical control groups. This novel approach appeared to help clear infection in eight of the nine patients; however, although the mortality rate for the treatment group was reduced from 58% in similar patients to 33%, this was too small a study to draw any conclusion about deaths. This approach of treating only patients with evidence of monocyte impairment was promising for larger studies. These authors appear not to have performed or contributed to other trials to enhance the power of their nine-patient trial.
Wasserman et al., Crit Care Med 1998 (Burns) [11]
This Phase III randomized double-blind trial compared subcutaneous IFN-γ in 109 burn patients with placebo in 107 patients. All patients had severe burns, scoring at least 7 on the Abbreviated Burn Index. Therapy was started in the first four days after thermal injury and continued daily until 90 d, hospital discharge, or wound closure. The IFN-γ-treated patients had equivalent rates of major infection and death. We believe that the putative benefits of therapy could have been masked by including patients with no evidence of monocyte impairment and of older, severely burned patients, who are likely to die regardless of the intervention.
Nakos et al., Crit Care Med 2002 (Trauma) [12]
In 2002, Nakos et al. studied mechanically ventilated trauma patients having an alveolar macrophage HLA-DR of <30%, as found by bronchoscopy (in 21 of 52 patients). Patients were randomized to inhaled recombinant IFN-γ (11 patients) or placebo (10 patients). The Injury Severity Score was 40 and 43, respectively. The treatment group received inhaled IFN-γ three times a day. These investigators found increased HLA-DR expression, from 16.4% to 44%, in the follow-up bronchoscopy on day 3 after injury. This compared with a persistence of low HLA-DR in the placebo group. In addition, there was a decrease in bronchoalveolar fluid interleukin (IL)-10 concentration and decreased rates of ventilator-associated pneumonia than in the placebo group. It is not clear whether the inhaled delivery allowed IFN-γ to have significant systemic effects. The mortality rate remained unchanged. This important trial needs to be repeated; the alveolar macrophage action plus inhaled IFN-γ are both unique.
Schinkel et al., Shock, 2001 and Licht et al., J Interfeon Cytokine Res 2003 (Major Elective Surgery) [13,14]
The Faist group (both papers) screened 209 patients undergoing major surgery for pre-operative immunosuppression, defined by a negative delayed-type hypersensitivity skin test [13]. Of those, 46 anergic patients (22%) were randomized to pre-operative parenteral IFN-γ (on days −7, −5, and −3). Visceral, gynecologic, vascular, and thoracic operations were included and were said to be physiologically equivalent in each group. There was a significant increase in HLA-DR, IL-1, and IL-8. Also, LPS-induced TNF-α was augmented. A subsequent 2003 report from the same group said that treated patients demonstrated increased IL-2R and decreased IL-4 concentrations, without effect on IL-10 or lymphocyte proliferation, suggesting a shift to a Th1 phenotype. The investigators cited a generally low number of infectious complications and were unable to demonstrate any real differences in morbidity and mortality rates. There are many examples of bias in these trials of dually reported patients that could warrant repeating the test in more depth and breadth, particularly to the extent that skin testing does or does not reflect monocyte function.
Granulocyte-Macrophage Colony-Stimulating Factor (GM-CSF)
Meisel et al., Am J Respir Crit Care Med, 2009 (Sepsis) [15]
This randomized double-blinded trial using GM-CSF was undertaken in very sick patients, with the protocol requiring severe sepsis or septic shock for inclusion. More specifically, patients were required to have depressed monocyte HLA-DR expression for two consecutive days. This yielded 38 patients from a total of 135 who were screened for impaired monocyte function. Pneumonia was the leading cause of sepsis, affecting 60% of the 38 patients, and peritonitis was responsible for 30%. After eight days of treatment, all 19 patients in the treatment arm demonstrated increased monocyte HLA-DR expression, as well as restored ex-vivo TNF-α secretion. Furthermore, T-cell and monocyte counts increased, accompanied by a decrease in IL-10. Such patients had shorter times of ventilation and shorter ICU stays. The mortality rate was 16% in the GM-CSF group vs. 21% in the placebo group, but this difference was not statistically significant. This study badly needs expansion or repeating!
Leentjens et al., Am J Respir Crit Care Med 2012 (Experimental Endotoxemia) [16]
Leentjens et al. induced impaired monocyte function in healthy volunteers given low-dose intravenous LPS. Eighteen males were then randomized to receive IFN-γ, GM-CSF, or placebo for three alternate days, followed by a second LPS dose on day 7. The placebo group had an initial increase in the concentrations of TNF-α, IL-6, IL-10, and IL-1RA after the first dose, but after the second dose, there was a reduction in TNF-α production, in keeping with in-vitro monocyte models (see Fig. 1). After the second LPS dose, there was a trend to lower IL-10, but this did not reach statistical significance. Expression of HLA-DR decreased after the first dose of LPS but appeared to recover prior to a subsequent similar depression in response to the second LPS dose. Compared with the placebo-treated subjects, IFN-γ increased TNF-α and HLA-DR, with decreased IL-10, and was more effective than GM-CSF in achieving monocyte activation. This effect appears to slow in healthy human beings; many of the aspects of the impaired monocytes we have noted [1].
Spies et al., PLoS One 2015 (Major Elective Surgery) [17]
This recent randomized trial examined the role of continuous intravenous infusion of GM-CSF in preventing infection after elective esophageal and pancreatic resections. Crucially, only patients with empirically proved low monocyte DR expression on post-operative day 1 were eligible. Although we have discussed using a single observation to trigger immunoadjuvant therapy, more than one subnormal value could define the deficiency more clearly. Sixty-one patients were included in this trial, equally distributed into a GM-CSF group, influenza vaccination, and placebo. As expected, the GM-CSF-treated group developed significantly higher monocyte HLA-DR expression than the placebo-treated group. However, daily HLA-DR measurements were used to assess the response, and as soon as the treated patients reached the threshold of 10,000 monoclonal antibodies per cell, therapy was stopped. Therefore, the duration of this immunoadjuvant use was short: (i.e., between one and three days of continuous intravenous infusion). The result was a rapid return of monocyte HLA-DR to the depressed amounts of the other two groups by post-operative day 5. Note the similarity of this “post-treatment dip” to our group's prior interferon-γ study, as demonstrated in Figure 3. Spies et al. reported fewer “infection days” in the GM-CSF-treated patients, but the post-operative infection rate was similar in the two groups. We believe the learning point may be that single monocyte HLA-DR measurement of response may not be an optimum marker of treatment effect. In addition, the immunologic benefits of GM-CSF appear transient (at least in circulating monocytes), and therefore, therapy probably should continue for at least 7–14 days when the peak post-operative infection rate might occur.
The decision to include an arm of influenza vaccine and its apparent association with increased delirium detracts from the clarity of this work.
G-Csf
Schneider et al., Ann Surg 2004 (Major Elective Surgery) [18]
Prophylaxis with G-CSF was given pre-operatively to patients undergoing major extirpative surgery. Sixty patients were divided equally into three arms: Two different G-CSF regimens and placebo. In the first regimen, subcutaneous G-CSF was given on peri-operative days −2, 1, and 3, whereas the second regimen had a dose on day −2, with smaller subsequent doses on the following five days. Operations included a mixed bag of colectomy, gastrectomy, Whipple pancreatoduodenectomy, esophagectomy, and liver and lung resection. Patients who received G-CSF had greater TNF-α production and HLA-DR expression and decreased lymphocyte anergy. This led to both a decreased rate and lesser severity of infection in the treatment group. Interestingly, the authors said that, in their opinion, monocyte deactivation was irreversible, and that this therapy exerted its effects by increasing the number of functioning leukocytes. Although this study included an odd collection of variably big and really big operations, the differences described are worthy of future work.
Bo et al., J. Crit Care 2011 (Sepsis) [19]
In 2001, Bo et al. undertook a meta-analysis of 12 randomized trials using either G-CSF or GM-CSF in sepsis. This series included 2,380 patients. Most of the studies included did not target therapy specifically to patients with impaired monocyte function. Although there was a trend to lower death rates in the treatment groups, there were no statistically significant differences in 28-day mortality rate for either immunoadjuvant. That being said, in three trials of G-CSF and one trial of GM-CSF, both agents appeared to reverse infection to a degree of statistical significance. This paper contains many loose ends but needs more in-depth review because of its innate potential value.
Alternative Approaches
Although the subject is beyond the scope of this review, there have been various alternative approaches for immunomodulation, including extra-corporeal blood and plasma filtration. Early work showed that endotoxin filtration combined with immune stimulation improves survival in a murine model of sepsis [20]. Endotoxin filtration, such as with polymyxin B cartridges, for severe sepsis has been accepted therapy in Japan, with approval also for many years in Europe, as discussed by Esteban et al. [21]. Furthermore, cytokine filters (such as CYTOSORB®) have the potential for filtering out “harmful” pro-inflammatory cytokines. This principle is probably oversimplified, and elucidating optimum timing, if such there is, will be difficult. Nevertheless, there is no acceptable evidence at present for filtration use in the U.S.A.
Challenges of Therapy
Providing the patient with a reliable immunoadjuvant to treat the pathophysiology of a major insult, whether it specifically addresses monocyte impairment or other aspects of the response, remains an old conundrum yet to be resolved. Spontaneous insults such as major trauma, burns, or sepsis are a difficult issue to control for in a randomized fashion. With such heterogeneity, ensuring equal distribution between treatment and placebo groups is difficult, as discussed earlier. Furthermore, each patient will have numerous treatments, ranging from antibiotics, fluid therapy, inotropic support, and, potentially, mechanical ventilation, not to mention source control. With so many variables, proving that the addition of a single adjuvant can make a statistically significant improvement in the mortality rate becomes difficult.
Studies may show improvement in the short-term outcomes, yet when one examines the 90-day mortality rate, it remains unchanged [22]. Timing is a major issue, not just for follow-up, but also in the introduction, duration, and cessation of therapy, given the changing immune milieu from initial insult to prolonged recovery, as discussed earlier.
The immune system is redundant, which likely is a product of evolution. With so many different positive and negative effects of various inflammatory pathways, changing or altering one protein is not likely to change the ultimate outcome for a patient. Indeed, it may have unrecognized negative consequences, such as those seen in early corticosteroid and anti-TNF-α therapeutic trials. One could compare this, however, with the common use of brief peri-operative antibiotic prophylaxis for clean-contaminated elective operations. Antibiotics were in use by surgeons for more than 20 years before definitive clinical proof of their value was obtained; this is now the most common use of antibiotic agents in the world.
Although not specifically aimed at monocyte function, a meta-analysis of the effects of immune adjuvants are shown in Figure 4 [23]. Early approaches, specifically for sepsis, targeted the apparent exuberant pro-inflammatory response, the so-called “cytokine storm.” The rational for a therapeutic target was the predominance of TNF-α, IL-6, and IL-1β production from innate immune cells such as monocytes, leading to endothelial activation and acute-phase proteins contributing to vasodilation, shock, acute respiratory distress syndrome, and multi-organ dysfunction. Furthermore, blockage or binding of LPS may lower the pathogen-associated molecular pattern load to limit the foregoing cascade.

Therapeutic efficacy of mediator-targeted therapy for sepsis. (With permission from Marshall et al. [23] as modified in Fry DE [ed]: Surgical Infections, 2nd ed. St. Louis. JP Medical, 2013.)
A simple dampening of the immune system with corticosteroid therapy has remained controversial. Moreover, this approach has never improved mortality rates convincingly. The only U.S. Food and Drug Administration-approved therapy was detracogin alpha (Xigris®), a form of activated protein C. Despite its initial success in the PROWESS trial, concerns about its efficacy and bleeding side effects led to the subsequent PROWESS-SHOCK trial in 2012. Those investigators concluded that 28- and 90-day mortality rates were not significantly different in treated patients, leading to withdrawal of FDA approval [22].
Eritoran is a synthetic lipid A antagonist to MD-2-TLR4 that was used recently in a randomized controlled trial in 1,961 patients with severe sepsis. This followed previous strategies targeting endotoxemia (such as lipid A antibodies). In this Phase III trial, the placebo group had a mortality rate of 27%, much lower than the 40% expected by the investigators. Furthermore, patients with gram positive infection appeared to do worse than the group on placebo. In contrast to a smaller Phase II trial before it, there was no decrease in 28-day or one-year mortality rate [24].
The authors are concerned broadly about publication bias in this field; i.e., we suspect that numerous failed or ineffective applications of monocyte functional alterations have not been reported. Nine trials and one meta-analysis show many positive effects but no reproducible influence on death rates.
The Future of Monocyte Biology in the Surgical Patient
Since the continued failure of clinical trials to show a mortality benefit in major trauma and sepsis, the consensus seems to be moving toward ever more targeted therapy [25–28]; for example, treating only those patients with depressed monocyte HLA-DR with IFN-γ rather than non-specifically treating all patients. Such a tactic surely reduces the denominator, thus enhancing the demonstrable positive effects of putative treatments.
This approach needs a readily measurable biomarker that would represent the underlying immune phenotype accurately, be evident early enough to direct therapy, and also respond in a way that will guide treatment. In many diseases, miRNAs have been found to be stable and reliable markers in various conditions, including cancer. Furthermore, various studies have identified miRNAs that are dysregulated in patients with sepsis [29–32]. More recent studies have implicated miRNAs in the host defense against trauma [33–35]. In general, these studies have not been correlated with the underlying monocyte phenotype. It remains unclear if these markers could fulfill some of our criteria. For example, some miRNAs, such as miRNA-133a, have been linked to higher mortality rates in sepsis [36]. We have discussed how manipulation of such miRNAs could abrogate monocyte impairment, but as it stands, there appears to be no miRNA-based immunotherapy scheduled for immediate human trials.
It has been postulated that negative co-stimulatory markers such as PD-L1 are increased in patients with sepsis. There are few trials demonstrating this phenotype in major elective surgery or trauma. However, the apparent success of anti-PD-1- and anti-PD-L1-based therapy for malignant melanoma may provide direction to use such therapy for trauma patients or for patients with sepsis exhibiting this immune phenotype.
Future Immunoadjuvants
It is not just PD-1-based therapies that are targeting T-cell defects in sepsis patients. Recent murine studies of sepsis models promise that IL-7 and IL-15 monoclonal antibodies increase the activity and function of T lymphocytes. This may, in turn, increase endogenous IFN-γ and restore the healthy monocyte–T-cell interaction. However, much more research is required before this product can reach human clinical trials. The current list of registered trials for trauma and sepsis relating to monocyte function is summarized in Table 1 (see clinicaltrials.gov).
GM-CSF – granulocyte–macrophage colony-stimulating factor; IFN = interferon; N/A = not available; PD-1 = programmed cell death protein 1; PD-L1 = programmed cell death ligand; PMN = polymorphonuclear cells.
Conclusion
The predisposition and response of the immune system as a factor in the outcome of the surgical patient remains as relevant in 2016 as it ever has been. As high-throughput systems approaches to trauma and sepsis, such as the Glue Grant (Inflammation and Host Response to Injury [PI: Tompkins RG]. National Institute of General Medical Sciences [NIGMS]), continue, we recognize greater complexity, with more and more molecules associated with poor outcomes such as nosocomial infection and, indeed, death. The field has progressed well beyond a rudimentary pro- or anti-inflammatory response to a given insult. Yet, the same challenges remain. With this increased knowledge, how can the physician hijack the immune system to improve the outcome of a patient? The question of what therapy might be optimum, and its timing and duration, remains.
In a previous review, we demonstrated how there may be different affected components in a patient who has impaired host defenses; and indeed, one biomarker or therapy may not fit all. For example, perhaps interferon-Ύ or GM-CSF is the right adjuvant for the patient with confirmed impaired monocyte function, and anti-PD-1 therapy might be appropriate for the patient with proved T-cell anergy with elevated PD-1 expression. One of the most promising agents is still interferon-Ύ, but the persuasive trial that is adequately powered and targeted to those patients with impaired monocyte function has not been done. Much of the failed translation of pre-clinical studies to human trials for certain therapies may be attributable, in part, to the limits of murine research, the complex genetic and post-translational variation in our patients, and an incomplete understanding of how our redundant immune system responds.
At present, there is insufficient evidence for the use of interferon-Ύ, G-CSF, or GM-CSF in the adjuvant setting for major trauma, surgery, or overt infection. Furthermore, new therapies, with apparent success in the oncologic setting, have yet to be tested. We can hope that the registered trials discussed here will answer some of these questions. We believe that although the mortality rate has yet to be reduced convincingly by such agents, the approach of targeting patients with proved monocyte impairment for the right duration, whatever that might be, holds potential in improving outcomes in some of our patients.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest with regard to this manuscript. This publication is made possible in part by the John Williamson and Barbara Thruston Atwood Price Family Trust.