
Abstract
Abstract
Background:
Critically ill surgical patients remain at a high risk of adverse outcomes as a result of secondary peritonitis (SP). The risk is even higher if tertiary peritonitis (TP) develops. Factors related to the development of TP, however, are scarce in the literature. The main aim of our study was to identify factors associated with the development of TP in patients with SP in the intensive care unit (ICU), and also to report differences in microbiologic patterns and antibiotic therapy in patients with the two conditions.
Patients and Methods:
A prospective, observational study was conducted at our institution from 2010 to 2014. Baseline characteristics on admission, outcomes, microbiologic results, and antibiotic therapy were recorded for analysis.
Results:
We included 343 patients with SP, of whom TP developed in 185 (53.9%). Almost two-thirds (64.4%) were male; mean age was 63.7 ± 14.3 years, and mean APACHE was 19.4 ± 7.8. In-hospital death was 42.6% (146). Multivariable analysis showed that longer ICU stay (odds ratio [OR]: 1.019; 95% confidence interval [CI]: 1.004–1.034; p = 0.010), urgent operation on hospital admission (OR: 3.247; 95% CI: 1.392–7.575; p = 0.006), total parenteral nutrition (TPN) (OR: 3.079; 95% CI: 1.535–6.177; p = 0.002) and stomach-duodenum as primary infection site (OR: 4.818; 95% CI: 1.429–16.247; p = 0.011) were factors associated with the development of TP, whereas patients with localized peritonitis were less prone to have TP develop (OR: 0.308; 95% CI: 0.152–0.624; p = 0.001). Higher incidences of Candida spp. (OR: 1.275; 95% CI: 1.096–1.789; p = 0.016), Enterococcus faecium (OR: 1.085; 95% CI: 1.018–1.400; p = 0.002), and Enterococcus spp. (OR: 1.370; 95% CI: 1.139–1.989; p = 0.047) were found in TP, and higher rates of cephalosporin use in SP (OR: 3.51; 95% CI: 1.139–10.817; p = 0.035).
Conclusions:
Complicated peritonitis remains a cause of a high numbers of deaths in the ICU. The need for TPN, urgent operation on hospital admission, and particularly surgical procedures in the proximal gastrointestinal tract were factors associated with development of TP and may potentially help to identify patients with SP at risk for development of TP. Physicians should be aware concerning multi-drug–resistant germs when treating these patients.
P
Despite advances in the management of the peritoneal cavity, ICU surgical patients with peritonitis remain at a high risk of adverse outcome [4]. Secondary peritonitis is the most frequent form, associated with high morbidity and a death rate ranging from 17% to 63% [5]. Prompt surgical source control (e.g., re-laparotomy) is the treatment of choice and is mandatory alongside adequate antibiotic treatment. Tertiary peritonitis usually occurs at least 48–72 hours after adequate surgical treatment and source control of a previous SP; its death rate ranges from 30% to 60% [6].
The composition of the intra-abdominal flora found in ICU patients with peritonitis may be influenced by several factors, such as the location of the perforation, antibiotic pressure, and the ICU/hospital local flora [7]. The contaminating micro-organisms in SP and TP are diverse: TP is associated mostly with opportunistic and nosocomial pathogens, including multi-drug resistant (MDR) germs such as Enterococcus, Enterobacter, and Candida [8].
In previous series, TP was found to develop in 20% of patients with SP, and patients presented higher death rates and longer stay [8]. The costs associated with TP are higher because of the need for ICU admission [9]. Although many studies have looked for diagnostic markers able to predict the outcome of peritonitis in the ICU, there is little information at present on the identification of patients in whom TP is likely to develop [8].
The main aim of our research was to identify factors related to the development of TP in patients with SP admitted to our ICU. The secondary objective was to identify differences in microbiologic pattern and antibiotic therapy in these patients.
Patients and Methods
This prospective observational study was performed at our institution from January 2010 to December 2014. We included all consecutive patients who had undergone any type of abdominal surgical procedure with signs of peritonitis and who were admitted to the ICU for more than 24 hours for post-operative care. All included patients had organ failure after presenting with signs and symptoms of a systemic inflammatory response [1]. Figure 1 shows how SP or TP diagnosis was performed, in accordance with the definitions described above. To focus specifically on the critical care spectrum, we excluded patients who required only a short ICU admission (<24 h) and who recovered rapidly. All patients had undergone a surgical procedure before ICU admission and were transferred to the surgical theater for re-operation when required.
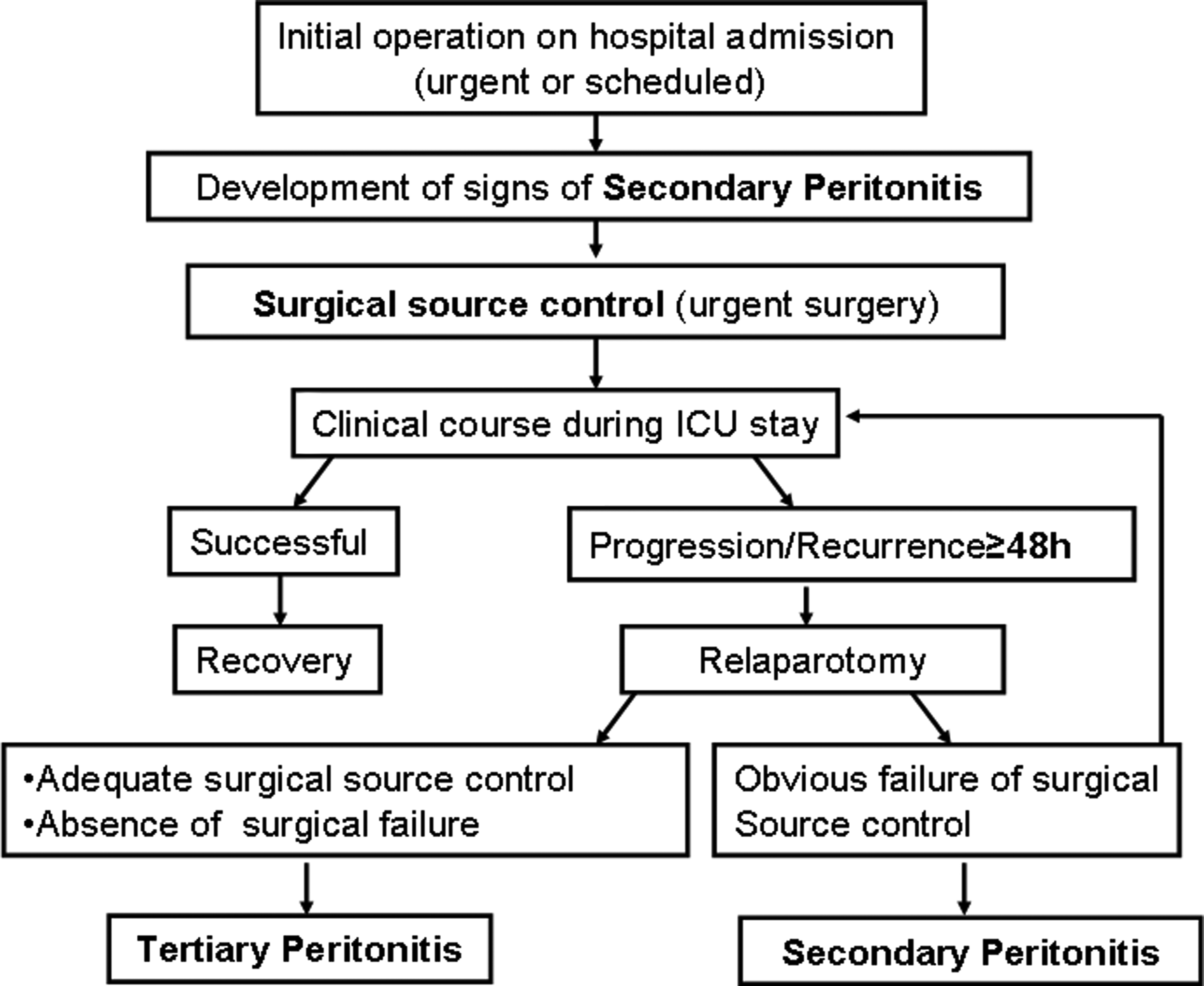
Diagnostic criteria for secondary and tertiary peritonitis during follow-up.
The study was approved by our hospital's Institutional Ethics Committee. The need for informed consent was waived because of the study's observational nature.
Diagnosis and decisions in all patients regarding ICU admission, medical treatments, source control measures of infection, and surgery needs (e.g., drainage of abscesses/collections of infected fluid, debridement of necrotic infected tissue) were evaluated daily by the attending ICU physicians and by the surgical team, in accordance with current recommendations [4]. Antibiotic use and microbiologic data were reviewed daily by the investigators. A program for optimizing the use of antibiotic therapy was applied in our hospital at the time the study was performed, which additionally ensured close interaction between the microbiology and infectious diseases teams and the ICU team to perform appropriate antibiotic de-escalation when possible. Thus, antibiotic therapy was administered in accordance with the patient's clinical status and local guidelines based on local flora, and applying a multi-disciplinary approach [9,10].
Each operation included pre-operative hygiene and pre-operative antibiotic prophylaxis when anesthesia was induced, covering anaerobic (e.g., metronidazole) and gram-negative bacteria (GNB) (e.g., amoxicillin/clavulanic acid, ceftriaxone, cefuroxime) in accordance with the institutional protocol. Information on previous microbiologic results and medical history (e.g., colonizing micro-organisms) was also considered to modify antibiotic prophylaxis and provide adequate coverage. Routine screening on ICU admission of skin and respiratory tract colonizing bacteria was also performed to determine the resistance pattern and to guide antibiotic therapy.
Data on ICU admission and during ICU stay were extracted from the medical record of each patient and recorded prospectively in a database. Variables were selected and agreed on by the authors based on those from previous studies [2–8]. The following information was recorded within 24 hours of ICU admission: Demographic data, medical history and co-morbidities, inflammatory response and arterial lactate (on ICU admission), surgical indication and type of surgical procedure on hospital admission (scheduled or urgent), surgical technique, intra-operative variables such as number of drainages, microbiologic findings, and treatment characteristics. Immunosuppression was defined as the presence of a factor that reduces or modifies the efficacy of the immune system (e.g., medications, spleen removal). Inflammatory response was characterized according to the Surviving Sepsis Campaign definitions [9,10].
During ICU stay, we recorded the development of TP, the presence of outcomes (e.g., need of vasopressor drugs, mechanical ventilation, and renal replacement therapy [RRT]) and new microbiologic findings. The criteria used for starting RRT were based on current clinical practice and consensus guidelines [11]. Early enteral nutrition (EN) (defined as <24 hours after ICU admission once the patient was stabilized) was attempted if indicated. If EN was not tolerated and an increased gastric residual volume (with a threshold of at least 500 mL) was present, or if the patient could not be fed by means of EN, total parenteral nutrition (TPN) was indicated [12]. Based on individual nutritional evaluation in agreement with the ICU nutritionist, immune-enhancing formulas were recommended; daily attempts at EN were made during ICU stay, and TPN was not usually initiated promptly (at the earliest, on day 3 after operation).
To determine illness severity, Sequential Organ Failure Assessment, Acute Physiology and Chronic Health Evaluation and Simplified Acute Physiology Score scoring systems were applied to all patients within 24 hours of ICU admission. Finally, after ICU discharge, patients were followed to assess in-hospital death.
Microbiologic sampling and antibiotic delivery were performed within 1 hour in accordance with local and international recommendations [13,14]. Blood cultures were performed by means of a conventional venipuncture method and from a vascular access device when indicated. Intra-abdominal samples (e.g., tissue samples and/or purulent material from abscesses) were also collected during operation and sent for microbiologic analysis.
Statistical analysis
Statistical analysis was performed using PASW statistics 13.0 (SPSS Inc., Chicago, IL). Continuous data are expressed as means ± standard deviation. Categorical data are expressed as percentages. Comparisons between groups with abnormal distribution of the variables were performed with the two-sample t-test or the Mann-Whitney U test (after applying the one-sample Kolmogorov-Smirnov test). The chi-square test was used to evaluate categorical variables. To confirm univariable results, a multivariable analysis using a logistic regression model was performed. Stepwise variable selection was performed, and a variable remained in the model if the p-value was <0.1.
We performed a total of three multivariable analyses: The first to assess the presence of variables associated with development of TP (main aim of our research) and two additional multivariable analyses to confirm differences between microbiologic pattern and antibiotic therapy between SP and TP (secondary objectives). Model fit was assessed by checking residual normality, the existence and influence of outliers, and goodness-of-fit. Odds ratios (ORs) and 95% confidence intervals (CIs) are quoted, as appropriate. A p value of 0.05 was considered statistically significant in all cases.
Results
We included 343 patients with SP, in whom TP developed in 185 (53.9%). Patient characteristics, type of infection, inflammatory response, type of initial surgery, anatomic location of primary infection sites, and outcomes are shown in Table 1. Variables associated with the procedures, such as time delay to operation, performance of second- and third-look surgical procedure, and type of surgical technique did not influence outcomes. The mean duration of hospitalization before the second operation after initial operation was 5.5 ± 3.2 days. All patients were receiving vasoactive drugs or inotropic support and were monitored by means of a central venous catheter, an arterial catheter, and a urinary catheter.
COPD = chronic obstructive pulmonary disease; HIV = human immunodeficiency virus; APACHE = Acute Physiology and Chronic Health Evaluation; SAPS = Simplified Acute Physiology Score; SOFA = Sequential Organ Failure Assessment; ARDS = Acute Respiratory Distress Syndrome; RRT = renal replacement therapy; ICU = intensive care unit. Data are mean ± standard deviation or percentage.
The sample for the microbiology cultures at operation was taken from an intra-abdominal abscess in 298 (86.9%) patients, biliary fluid in 21 (6.1%), percutaneous drainage in 11 (3.2%), and another source in the remaining 13 (3.8%). Microbiology results in isolates (shown in Table 2) revealed that GNB were found in 50.1% of the samples, of which 15.3% and 11.5% were Escherichia coli and Pseudomonas aeruginosa, respectively, 21.17% gram-positive cocci (GPC), and 15.1% fungi. More than one GNB was found in 13.9% of patients. Patients with TP presented isolated GPC (12.1% vs. 26.2%; p = 0.007) and fungi (7.6% vs. 19.2%; p = 0.001) more frequently than those with SP. Multivariable analysis that focused on differences among microbiologic patterns between SP and TP showed a higher incidence of Candida spp. (OR: 1.275 (95% CI: 1.096–1.789); p = 0.016), Enterococcus faecium (OR: 1.085 (95% CI: 1.018–1.400); p = 0.002) and Enterococcus spp. (OR: 1.370 (95% CI: 1.139–1.989); p = 0.047) in TP. In 303 (88.3%) patients, positive blood cultures were obtained, with the same micro-organisms as those found in the intra-abdominal samples.
Antimicrobial agents were evaluated every day based on a multi-disciplinary approach that included an assessment of patient clinical status, microbiology results, and antibiotic characteristics. The most frequently used antibiotic agents are shown in Table 3; in most cases (85.1%, n = 292), multiple or simultaneous sequential antibiotic agents were administered. A mean of 2.6 antibiotic/antifungal agents (ranging from two to four) were used in each patient, with a mean treatment duration of 10.6 ± 9.5 days. Multivariable analysis that focused on differences among antibiotic therapies between SP and TP showed a higher use of cephalosporins in SP (OR: 3.51 (95% CI: 1.139–10.817; p = 0.035). No association was found, however, between antibiotic therapy and the development of TP.
Three quarters of patients (75.8%, n = 260) presented resistance to one or more antibiotic agents in the culture antibiogram of intra-abdominal samples: Forty-eight (13.9%) presented extended spectrum beta-lactamase–producing Enterobacteriaceae and 30 (8.7%) carbapenem-resistant P. aeruginosa, but rates of typical MDR germs such as A. baumannii and methicillin-resistant Staphylococcus aureus (MRSA) were low (Table 2).
The multivariable analysis showed the main factors associated with the development of TP were longer ICU stay, the need for urgent operation on hospital admission, higher TPN needs, and stomach-duodenum as primary infection site, whereas patients with localized peritonitis on admission were less prone to development of TP (Table 4). No differences were observed regarding the occurrence of septic shock or death. The microbiologic species or antibiotic therapy had no influence over the development of TP, and there was no increase in MDR germs during the study period.
ICU = intensive care unit; ARDS = Acute Respiratory Distress Syndrome.
Discussion
The most important finding of the current study is the identification of factors associated with the development of TP in a cohort of patients with SP. To the best of our knowledge, there is only one prospective study in the literature that addresses specifically the development of TP after SP, although the development of TP entails a worse prognosis [8].
The need for TPN during ICU admission as a factor associated with the development of TP may be a reflection of the severity of the peritonitis and of an inadequate inflammatory response, which may lead to infectious complications because of immune dysfunction and an inability to tolerate early EN because of gastrointestinal dysfunction [15,16]. This may produce mucosal atrophy, which further increases the difficulty of feeding appropriately in terms of energy expenditure and protein needs, and strongly influences outcomes in this setting [17].
In abdominal operations, nutritional requirements do not differ from those in other ICU patients and depend on the patient's underlying process and degree of metabolic stress [18]. Although TPN individually adjusted to the patient's requirements may improve outcomes, addressing this issue remains difficult because of the absence of adequate nutritional biomarkers in clinical practice [19]. Reduced gastric emptying and absorption, motility, and underfeeding are the main problems after abdominal surgery and sepsis, and are associated with higher TPN needs [18]. Patients who are sick enough to require TPN may also be the patients in whom TP develops. This is also related to the fact that these patients were also more likely to have longer ICU stays.
We also found that patients who required urgent operation on hospital admission, particularly a surgical procedure in the proximal gastrointestinal tract, were more likely to have TP develop. As a general rule, patients who undergo urgent operation present higher rates of morbidity (and death) leading to prolonged ICU/hospital stay; the reason is that urgent operation does not allow pre-operative nutritional optimization, which may potentially improve results in these patients [20,21]. At the same time, the stomach-duodenum tract plays an important role in the early phase of nutrition in the digestive tract, and abdominal operation in this area may impair its physiologic functions [17]. On the other hand, the role of localized peritonitis as a protective factor against the development of TP seems related to an attenuated inflammatory response because of easier surgical source control. Higher Acute Physiology and Chronic Health Evaluation II, Simplified Acute Physiology Score II, and Mannheim Peritonitis Index scores, primary infections other than appendicitis, and C-reactive protein have also been described as risk factors for the development of TP [5,8]. Indeed, the longer ICU stays in patients with TP recorded here must be associated with more advanced organ dysfunction and illness severity and are a logical consequence of TP development [22].
Finally, regarding microbiologic findings, we showed a trend toward higher incidence of MDR with TP in our population. In agreement with previous studies, E. coli was the most frequently isolated microorganism [7,23]. The incidence of P. aeruginosa, reported to range from 3% to 5% in SP and from 11% to 21% in TP [24], was higher in our patients with TP, as were the rates of Enterococcus spp. and fungi, which are both associated with poor outcomes regardless of the type of peritonitis [25]. Enterococcus is associated with high death rates in peritonitis, even with adequate treatment, and an inadequate inflammatory response has been hypothesized [26,27]. It is also more frequently associated with severely ill, immunocompromised patients and with those treated with third-generation cephalosporins [28,29]. The initial severity of peritonitis and the presence of Candida spp. in cultures are also major risk factors for development of TP [30]. The higher prevalence of Candida spp. is linked with factors that are present in our population such as stomach-duodenum perforations, TPN, urgent operation, and long treatment periods with broad-spectrum antibiotic agents [7,26].
Regarding antibiotic use in our patients, the more frequent use of carbapenems and piperacillin/tazobactam may be explained by their application as initial empiric therapy. They both provide optimal activity and, in combination with a better de-escalation, may contribute to improving outcomes and preventing the appearance of MDR germs [25,31]. The higher microbiologic resistance rates of GNB such as E. coli to standard antibiotic therapy make the use of broad-spectrum antibiotic regimens mandatory [31]. Because of its microbiologic differences in relation to SP, TP may benefit from specific regimens [23]. Patients with higher co-morbidities, longer ICU admissions, and hospital stay more than a week are at a greater risk of colonization by MDR bacteria, and in these cases, the approach to TP is more complex [22].
Our study presents certain limitations. The most important is its single-center observational design. In addition, our results cannot be extrapolated to other less severely ill populations. Among the study's strengths are the large sample size, the prospective entry of all the data, and the use of post-operative scores that have not been used generally in other studies in spite of their importance in risk stratification. These features will allow for comparisons with other series in the future. Further, this study was conducted at a large tertiary referral university hospital with a high level of complexity, over a four-year period.
Although the prognosis of TP is theoretically worse [6], we did not observe any significant difference between patients with SP and TP, even with regard to the occurrence of septic shock or the death rate. We also found a high rate of TP development in SP. This is probably because of the severity of patients with SP included in our study, the high death and morbidity rates characteristic of ICU patients with peritonitis even with an optimal management, and the presence of a high proportion of immunosuppressed patients [8,15].
Conclusions
Complicated peritonitis remains a cause of a high number of deaths in the ICU, and its outcome may be related to illness severity. We showed that the need for TPN during ICU admission, as a surrogate marker of illness severity, and for urgent operation on hospital admission, especially in the proximal gastrointestinal tract, were factors associated with the development of TP in our population and may potentially serve to identify patients with SP in whom TP is likely to develop. On the other hand, patients with localized peritonitis on ICU admission were less prone to development of TP. Although the differences we found in the microbiologic pattern between SP and TP need to be confirmed in future studies, physicians should consider MDR germs that include GPC and fungi when managing TP empirically.
Footnotes
Acknowledgments
The authors wish to thank the ICU nurses and all members of the General Surgery Department for their contribution to the study and for their care of the patients. We also thank Michael Maudsley of the Universitat de Barcelona Language Services for helping with the English.
This study is dedicated to the memory of Antonio Díaz-Prieto, MD, PhD, of the Intensive Care Department for his contribution to the development of our database.
Author Disclosure Statement
No competing financial interests exist.