
Abstract
Abstract
Background:
To study the effectiveness of gentamicin-collagen sponges (GCS) for the prevention of surgical site infections (SSIs).
Methods:
A systematic search of the PubMed and Scopus databases was performed (up to April 2015) to identify randomized controlled trials evaluating the efficacy of GCS for the prevention of SSIs. A random effects model was applied.
Results:
Twenty-one RCTs (8,472 patients) were included. Gentamicin-collagen sponges were associated with a lower risk of SSIs (risk ratio [RR] 0.65; 95% confidence interval [CI] 0.49–0.84). Based on Jadad scores, a lower risk for the development of SSI was presented in lower-quality studies (Jadad <3; RR 0.44; 95% CI 0.27–0.71), but no difference was observed in high-quality studies (Jadad ≥3; RR 0.77; 95% CI 0.58–1.02). No difference was observed in all-cause deaths in the GCS group compared with the control group (RR 0.77; 95% CI 0.56–1.06).
Conclusions:
When analyzing lower-quality studies or only clean procedures, GCS significantly reduced the risk of SSI. Further high-quality randomized studies are needed to confirm the benefit of GCS for lowering mortality rates.
S
The main causative pathogens for SSIs are the native flora of the skin, mucous membranes, and hollow viscera. The predominant pathogens are gram positive (Staphylococcus spp., Enterococcus), gram negative (Escherichia coli), and anaerobic (Bacillus fragilis) organisms [2].
Various risk factors or predictors have been associated with a higher risk of SSIs. These include diabetes mellitus, smoking, the use of steroids or other immunosuppressive drugs, obesity, re-operation, long operating time, and contaminated or dirty procedures [2,3].
Several efforts have been made to reduce the incidence of SSIs. Antimicrobial prophylaxis, adequate antiseptic preparation of the skin, and laparoscopic surgery seem to reduce the likelihood of SSI [2,4]. Gentamicin-collagen sponges (GCS) have been developed in order to prevent post-operative site infections. They provide high concentrations of the antibiotic locally at the surgical site, with low serum concentrations and thus less toxicity. Additionally, the collagen has a positive effect on hemostasis and incision healing [5].
Although the use of GCS has increased in recent years, their effectiveness appears to be controversial [6–8]. Furthermore, the role of GCS against specific pathogens and for specific procedures is under debate [7,9–12]. We performed a systematic review and meta-analysis of randomized controlled trials (RCTs) to determine the effectiveness of GCS in the prevention of SSI.
Materials and Methods
Search strategy
A systematic search of the literature was performed in the Pubmed and Scopus databases up to April 2015. The following search terms were used: (gentamicin OR aminoglycoside) AND (sponge OR collagen). There was no limit on the year of publication.
Study selection
Two independent investigators (A.A.K. and K.A.P.) performed the search of the literature according to the PRISMA statement [13]. A study was eligible for inclusion only if: (1) it was an RCT; (2) it studied the efficiency of antibiotic sponges for the prevention of SSIs; and (3) a full text was available. A study was excluded if: (1) it was an abstract from a presentation at a conference; (2) it was written in a language other than English; (3) it was an animal or in-vitro study; (4) it had zero results regarding the development of SSI; and (5) it was one of multiple publications of the same data (in which case, only the study with the greatest number of patients was included).
Data extraction
Data were recorded regarding the study design, the region where the study was performed, the study period, the age of the patients, the commercial name of the antibiotic sponge, the provision of corporate funding, the definition of “infection,” the primary scope of the study, the rate of infection, and the follow-up period. The modified Jadad criteria were used to assess the quality of the studies [14]. A study with a Jadad score of ≥3 was considered to be of high quality.
Outcomes and definitions
The primary outcome analyzed was the development of SSI after the implantation of the antibiotic sponge. The secondary outcome was all-cause deaths. The definition of SSI (either superficial or deep) provided by each study was considered to be eligible. A further analysis was performed based on the definition of the U.S. Centers for Disease Control and Prevention (CDC)/National Healthcare Safety Network criteria [15].
Statistical analysis
The Mantel–Haenszel random effect model was used to estimate the pooled risk ratio (RR) and the 95% confidence interval (CI) for all outcomes. A χ2 test (p < 0.10 indicated significant heterogeneity) and I2 were used for the assessment of statistical heterogeneity. Publication bias was assessed using a funnel plot of standard errors. The statistical analysis was performed using Review Manager version 5.2.
Results
Characteristics of the studies included
The selection process is outlined in Fig. 1. Our literature search identified 1,969 publications, of which 1,908 were excluded after abstract review for failure to comply with the inclusion criteria. Sixty-one studies were assessed in full text, of which 21 (8,472 participants) fulfilling our inclusion criteria were included in our analysis [6–12,16–29]. The main characteristics of these studies are presented in Table 1. Sixteen studies were performed in Europe, two in the United States, two in Turkey, and one in Mexico. Nine studies were multicenter [7,9,11,12,16,18,19,28,29], the other 12 being single center [6,8,10,17,20–27]. Fifteen studies were non-funded, whereas six studies were funded directly by the company making the sponges. Eighteen studies compared GCS recipients with patients who did not receive any sponge [6–12,16–20,22,23,25,26,28,29]. Two studies compared GCS patients with a control group receiving a non-antibiotic sponge [21,27]. One study had three arms comparing GCS, no-sponge, and non-antibiotic-sponge patients [24]. Eight studies analyzed the role of GCS after colorectal surgery, and four studies analyzed the role of GCS in the development of sternal infections after cardiac surgery [9,10,12,27]. Two studies analyzed the role of GCS after pilonidal sinus excision [16,28]. The remaining studies analyzed GCS results in other types of surgery, including orthopedic (hip arthroplasty) [11], hidradenitis suppurativa [17], abdominal [20], and groin hernia [22] surgery; splenectomy [6]; anorectal abscess suture [8]; and mastectomy [29]. Eleven studies had a Jadad score of ≥3 [7,9-12,16,18,21,24,25,27], whereas 10 had a lower score (6,8,17,19,20,22,23,26,28,29). Thirteen studies [6-12,19,21,24–27] provided a definition of SSI, whereas eight studies [16-18,20,22,23 28,29]) did not. Nine studies provided a definition of SSI based on the CDC criteria [7,9–12,21,24,25,27]. The populations of the studies are characterized by significant heterogeneity regarding the type of operation and the risk factors for the development of SSI.

Flow diagram of selection process for studies analyzed.
CDC = U.S. Centers for Disease Control and Prevention; DB = double blind; GCS = gentamicin collagen sponge; NR = not reported; MC = multi-center; SC = single center; RCT = randomized controlled trial; SWI = sternal wound infection.
Prevention of infections
Patients with GCS had a lower risk of SSI in several analyses, as presented in Table 2 [6-12,16-29]. The overall risk for SSIs was significantly lower in the GCS group than in the control group (21 studies; 8,472 participants; RR 0.65; 95% CI 0.49–0.84; Fig. 2). There was significant heterogeneity (I2 = 63%). The publication bias is depicted as a funnel plot in Appendix A. The GCS group had a lower risk of SSI in low-quality studies, but no difference was observed in the high-quality studies (Fig. 3). A lower risk of SSI was observed in double-blind studies, single-center studies, studies performed in Europe or in other countries, and non-funded studies. Fewer infections were observed in clean procedures, but no difference was observed in clean-contaminated or contaminated-dirty procedures. The risk of infection was lower in studies with a definition of “infection” based on clinical signs or cultures (RR 0.72; 95% CI 0.52–1.00) and in studies with no definition (RR 0.53; 95% CI 0.35–0.80). On the contrary, no difference was observed in studies with a definition based on the CDC criteria [15].

Forest plot depicting risk ratios for gentamicin-collagen sponge-associated infections when patients with GCS were compared with control group. Vertical line indicates the “no difference” point for two groups; squares indicate risk ratios; diamonds show pooled risk ratios for all studies; horizontal lines indicate 95% confidence intervals; “events” are the number of infections; “total” refers to number of procedures.
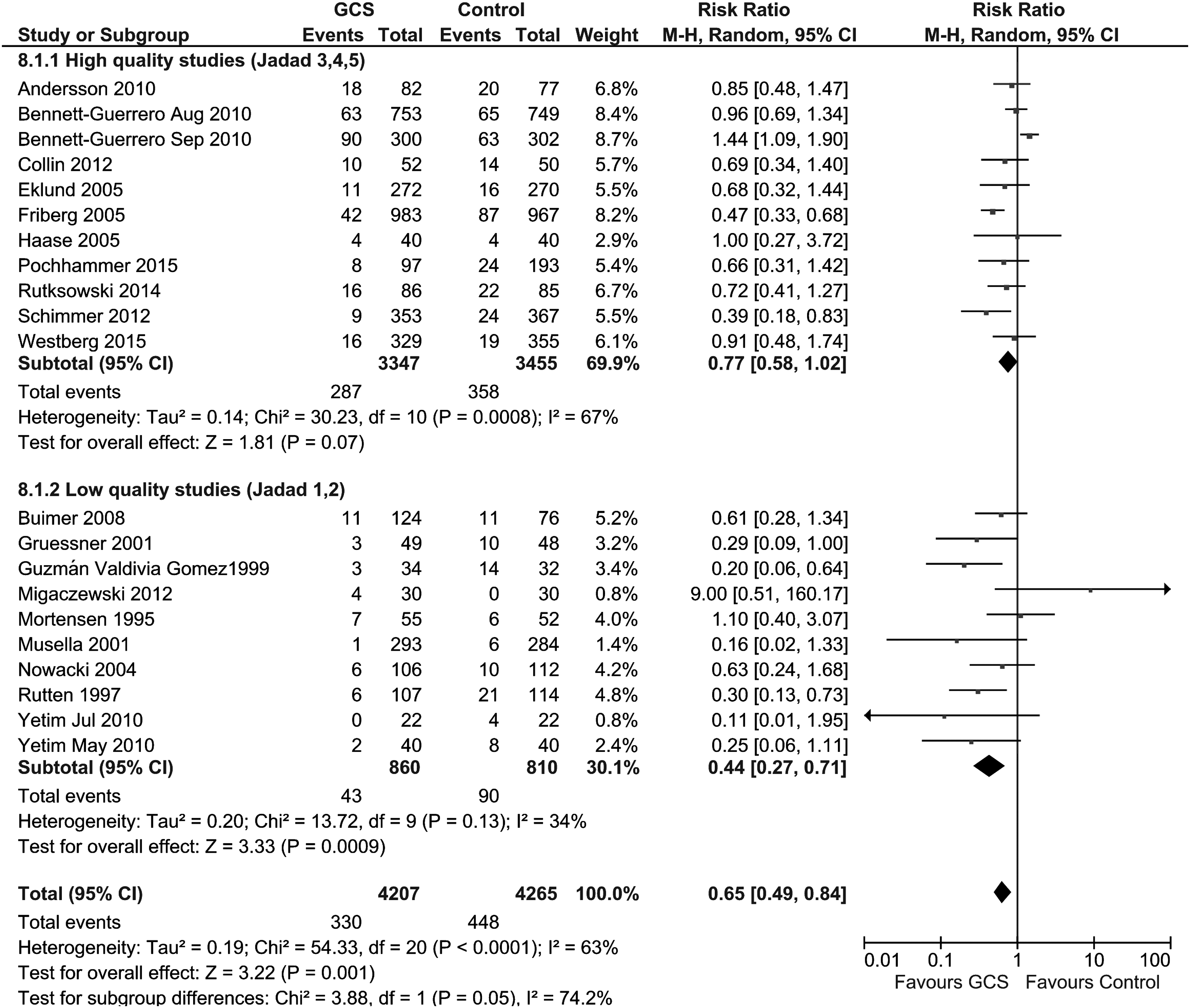
Forest plot depicting risk ratios for gentamicin-collagen sponge-associated infections when patients with GCS were compared with control group in high- and low-quality studies as defined by the Jadad score. Vertical line indicates the “no difference” between two groups; squares indicate risk ratios; diamonds show pooled risk ratios for all studies; horizontal lines define 95% confidence intervals; “events” represent number of infections; “total” refers to number of procedures.
CDC = U.S. Centers for Disease Control and Prevention, CoNS = coagulase-negative staphylococci; GCS = gentamicin collagen sponges; MRSA: methicillin-resistant Staphylococcus aureus.
Statistically significant associations are printed in boldface type.
Gentamicin-collagen sponges were associated with a lower risk of SSIs in studies covering patients with low and medium infection rates, but no difference was found in studies of patients with a high infection rate. There was no difference in SSI rates between the GCS and the control group when superficial or deep infections were analyzed separately. A higher total gentamicin content (≥130 mg) was associated with a lower risk of infection (RR 0.55; 95% CI 0.32–0.93), whereas a lower content marginally reduced the risk (RR 0.73; 95% CI 0.54–1.00). Sensitivity analysis after the exclusion of studies with more than 1,000 patients showed fewer infections for the GCS group. Patients treated with GCS had no difference regarding the development of gram-positive, gram-negative, or any coagulase-negative staphylococcal or methicillin-resistant S. aureus infections. No benefit for patients treated with GCS was observed for either early (-1999) or late (2000–2015) period studies.
Gentamicin-collagen sponges in specific types of surgery
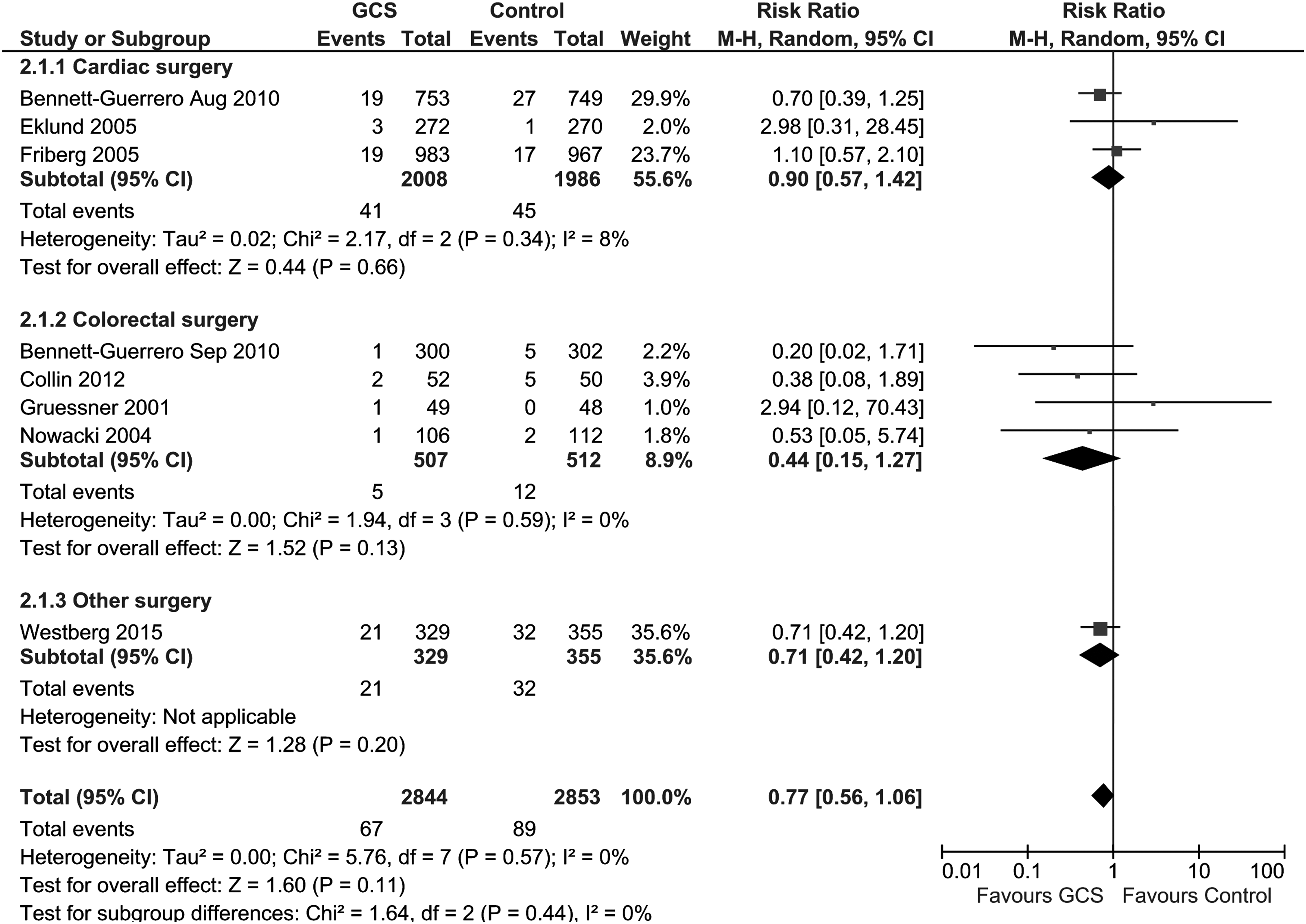
The results for the effectiveness of GCS for specific types of surgery are presented in Table 3. Among patients undergoing cardiac surgery, the risk of sternal SSIs was significantly lower in the GCS group than in the control group (four studies; 4,714 participants; RR 0.61; 95% CI 0.39–0.97) [9,10,12,27]. There was significant heterogeneity (I2 = 71%). Sub-group analyses showed a difference for deep sternal incision infections, but no benefit was observed for superficial sternal incision infections or mediastinitis (RR 0.50; 95% CI 0.19–1.33). Among patients undergoing colorectal surgery, no benefit of GCS was observed (eight studies; 1,781 participants; RR 0.69; 95% CI 0.44–1.08) [7,18,19,21,23–26]. Sub-group analyses found no benefit against either superficial or deep infections. In pilonidal sinus operations, patients did not benefit from the use of GCS [16, 28]. A pooled analysis for other surgical procedures (seven studies; 1,738 patients) showed no difference between the groups [6,8,11,17,20,22,29].
SWI: sternal wound infection.
Statistically significant associations are presented in bold text.
Mortality
Eight studies provided data regarding all-cause deaths among 5,697 patients [7,9–12,18,19,23]. Four studies provided data regarding colorectal surgery, three regarding cardiac surgery, and one regarding orthopedic surgery (Table 4). When GCS recipients were compared with the control group, no benefit and only a trend toward lower risk were observed in all-cause deaths for all studies (RR 0.77; 95% CI 0.56–1.06; Fig. 4); sub-group analyses found no difference in either colorectal or cardiac surgery.
Forest plot depicting risk ratios for all-cause deaths when patients with gentamicin-collagen sponges were compared with control group. Vertical line indicates the “no difference” point between the two groups; squares indicate risk ratios; diamonds show pooled risk ratios for all studies; horizontal lines define 95% confidence intervals; “events” represent number of infections; “total” refers to number of procedures
Discussion
The present meta-analysis investigated the efficacy of GCS in the prevention of SSI. Patients having GCS were compared with patients having either non-antibiotic sponges or no sponges. The GCS were associated with a lower risk of infection regardless of the control group in the meta-analysis of all studies. Patients receiving GCS had a benefit in the following sub-group analyses: Low-quality, double-blind, single-center, non-funded studies; origin of the study (Europe or other countries); clean procedures; any definition of “infection” based on clinical signs or cultures or no definition; low or medium rate of infection; cardiac surgery (sternal infections); deep infection for cardiac surgery; and higher or lower doses of gentamicin. Similar results were observed when GCS recipients were compared with control participants excluding the study with differences in the surgical technique among the groups [20]. A sensitivity analysis excluding studies with more than 1,000 patients found similar results for fewer infections than in the primary analysis.
No benefit was found in the GCS group in the following sub-group analyses: High-quality, multi-center, funded, early- or late-period studies; origin of the study (United States); clean-contaminated or contaminated-dirty procedures; CDC definition of infection; superficial infection; deep infection; and high rate of infection. No difference between the GCS and the control group was observed in the development of gram-positive, gram-negative, staphylococcal, coagulase-negative, and methicillin-resistant S. aureus infections. Only a trend to a lower risk of infection was observed in high-quality studies, and therefore, further studies are needed to confirm the benefit of GCS. No difference was observed in participants who received GCS in specific types of surgery with the following characteristics: Superficial infection or mediastinitis for cardiac surgery; colorectal surgery; deep or superficial infection for colorectal surgery; pilonidal sinus surgery; and other types of surgery.
It is clear from Table 3, and as also detailed in the text, that this technology will benefit patients who undergo cardiac surgery. It is still unconfirmed whether it will benefit patients who undergo colorectal or pilonidal sinus surgery.
The main patient risk-reduction intervention, in addition to the use of GCS, is antibiotic prophylaxis. Eighteen studies reported the use of antibiotic prophylaxis [6–12,18–28]. Additionally, laparoscopic surgery may reduce the development of SSI. Laparoscopic surgery was reported in three studies [6,7,24]. However, the role of the above-mentioned factors is still controversial, that is, whether they reduce the incidence of SSI is not clear.
The present meta-analysis sought also to investigate the risk for all-cause death in patients treated with GCS. A non-significant difference for a lower risk of all-cause deaths was observed when patients receiving GCS were compared with the control group. Only eight of the 21 studies provided data regarding mortality rates, with a range of 0.7%–7.7%. Two previous meta-analyses that studied the effectiveness of GCS did not analyze or present results regarding deaths [30,31].
This meta-analysis includes 21 randomized studies (8,472 patients) and presents 44 comparisons regarding the development of SSI and three comparisons regarding all-cause death. A previous meta-analysis presented the results of seven comparisons (15 randomized studies; 6,979 patients) regarding the development of SSI [31].
We investigated the role of GCS against specific types of pathogens. Gentamicin as an anti-microbial agent provides sufficient activity against gram-positive or gram-negative pathogens [3]. There was no significant difference from the control patients in the risk of gram-positive, gram-negative, or coagulase-negative SSIs when patients were treated with GCS. Heterogeneity was not observed in the aforementioned analyses. Only two studies provided data for methicillin-resistant S. aureus infections, with no difference between groups (131 patients; I2 = 55%). The effect of GCS use on the emergence of antibiotic-resistant pathogens is a question that needs additional investigation; we did not examine this effect.
Further studies are needed to determine the optimum total dose of gentamicin in collagen sponges to prevent SSI. We found that higher doses were associated with a lower risk of infection, but only a marginal difference was observed with lower doses. In each cited study, the authors used a different type of GCS, the difference being in the amount of gentamicin. Some authors additionally used one or multiple collagen sponges in the same patient. Thus, the dose of gentamicin was variable between studies.
We also found that GCS demonstrated their effectiveness in clean procedures but not in clean-contaminated or contaminated-dirty procedures. The GCS also were effective in procedures with a low or medium infection rate but not in studies with a high infection rate. An explanation for these results is that additional infection control measures are required to prevent surgical infections in these procedures.
The present study has certain limitations. Assessment of statistical heterogeneity is essential for the interpretation of meta-analyses. Heterogeneity was observed to a low degree (I2 <25%) in 14 comparisons, to a moderate degree (I2 = 25–60%) in 15 comparisons, and to a high degree (I2 >60%) in 18 comparisons. Although statistical heterogeneity was not significant in several analyses, we used a random effects model because of the clinical diversity of the studies. There are three reasons for this decision. First, the type of operation and the surgical technique differed across studies. In the meta-analysis, the majority of participants were undergoing cardiac (4,714 patients) or colorectal (1,781 patients) procedures. Data for pilonidal surgery was available in only two studies (239 patients), and other types of surgery were evaluated in the remaining seven studies (1,738 participants). Second, the followup period differed among the studies, ranging from to seven d to 12 mos. Third, the definition of infection differed among the studies, and it is notable that eight studies (1,446 participants) did not provide a definition of SSI.
The aim of our study was to show the effectiveness of antibiotic-collagen sponges with a common, strict definition of surgical infection. We considered the CDC criteria for the development of SSI to be consistent with a lower-bias meta-analysis than any other definition of surgical infection. Fourth, one study described different surgical techniques among the groups that were compared [20]. In the GCS group, the surgical incision was closed with sutures, whereas in the control group, the site remained open. Finally, studies used a different dose of gentamicin and, probably, different systemic antibiotic prophylaxis.
Conclusions
The present study provides additional evidence for the effectiveness of GCS in preventing SSIs. Further high-quality randomized studies with comparable patient characteristics and a common definition of infection are required to confirm the effectiveness of GCS in specific types of surgery. Additionally, new studies focusing on the microbiology of infection are required to prove the effectiveness of GCS against specific pathogens and their effect on the emergence of resistance.
Footnotes
Author Disclosure Statement
No funding was provided for this study. The authors have no conflicts of interest to declare.