
Abstract
Abstract
Background:
Patients with infective endocarditis (IE) are at high risk for post-operative morbidity and death, which might be associated with drug abuse. The purpose of this study is to evaluate the impact of drug dependence on outcomes in patients who have IE and undergo valvular surgery (VS).
Patients and Methods:
The Nationwide/National Inpatient Sample 2001–2012 was queried to select patients with IE who had elective VS using International Classification of Diseases, Ninth Revision, Clinical Modification diagnosis and procedure codes. Among them, patients with drug dependence (PDD) were identified, and their health status and post-operative outcomes were compared with those in patients without drug dependence (control group). Chi-square and Wilcoxon rank sum tests as well as multi-variable regression analysis were used for statistics.
Results:
A total of 809 (12.9%) PDD of the 6,264 patients who underwent VS were evaluated. They were younger compared with those in the control group (39.0 ± 10.8 y vs. 54.4 ± 14.8 y; p < 0.0001), had less age-related co-morbidities such as hypertension, diabetes mellitus, congestive heart failure, renal failure, obesity, but greater rates of alcohol abuse, liver disease, and psychoses. Despite the younger age and fewer co-morbidities, PDD compared with control patients were more likely to have post-operative complications develop overall (odds ratio [OR] = 1.6; 95% confidence interval [CI] 1.34-2.01), including infectious complications (OR = 1.5; 95% CI 1.27–1.78), specifically pneumonia (OR = 1.4; 95% CI 1.14–1.74) and sepsis (OR = 1.4; 95% CI 1.16–1.63), renal complications (OR = 1.5; 95% CI 1.23–1.77), and pulmonary embolism (OR = 1.9; 95% CI 1.44–2.52). Further, PDD had 11% longer hospital length of stay than those in the control groups (p < 0.0001). We did not find significant difference in hospital deaths, however, between these groups.
Conclusion:
Drug dependence is associated with worse post-operative outcomes in patients with infective endocarditis who underwent valvular surgery and lengthens their hospital stay.
E
Infective endocarditis in IVDUs differs substantially from that typically observed in the general population in terms of microbiology and the involvement of multiple heart valves [7]. Patients with IE are at high risk for post-operative morbidity and death, which might be associated with drug abuse. The purpose of this study is to evaluate the impact of drug dependence on outcomes in patients who have IE and undergo valvular surgery (VS). We hypothesize that patients with a history of drug dependence will have more post-operative complications than those patients without a history of drug use who undergo VS.
Patients and Methods
The data for analysis were taken from the NIS (National/Nationwide Inpatient Sample) database from 2001 to 2012. Developed by the Agency for Healthcare Research and Quality (AHRQ) as a part of the Healthcare Cost and Utilization Project (HCUP), NIS is the largest publicly available all-payer hospital discharge database in the United States. It includes clinical and resource utilization information for about 20% of all hospital stays in community hospitals. More detailed information about this database may be found in the literature [8].
The study population included patients aged 18 years and above who were hospitalized with endocarditis as a principal diagnosis (ICD-9-CM [International Classification of Diseases, Ninth Revision, Clinical Modification] diagnosis codes 036.42, 074.22, 093.2x, 098.84, 112.81, 115.x4, 399.1, 421.x, and 424.9x) and underwent replacement of heart value (ICD-9-CM procedure code 35.2x) or valvuloplasty without replacement (ICD-9-CM procedure code 35.1x). To identify those with drug abuse, we used AHRQ co-morbidity measure CM_DRUG that is available in the NIS database.
Employing the appropriate ICD-9-CM diagnosis codes for secondary diagnoses, we detected the following post-operative complications: Cardiac complications including myocardial infarction (997.1, 410.00-410.02, 410.10-410.12, 410.20-410.22, 410.30-410.32, 410.40-410.42, 410.50-410.52, 410.60-410.62, 410.70-410.72, 410.80-410.82, 410.90-410.92, and 427.5); respiratory complications and pneumonia (997.3x, 480.x, 481, 482.0-482.2, 482.3x, 482.4x, 482.8x, 482.9, 483.x, 484.x, 485, 486, 507.0, 512.1, 518.4, 518.5, 518.81, and 518.82); renal complications and acute renal failure ( 997.5, 584.x, and 593.81); post-operative stroke and cerebral hemorrhage (997.02, 430, 431, and 432.x); sepsis and other blood stream infections (038.0, 038.1x, 038.2, 038.3, 038.4x, 038.8, 038.9, 995.91, 995.92, 998.0, 785.52, 996.61, 996.62, and 999.3x); surgical site infection (SSI; 998.5x, 998.30- 998.32, and 998.83); urinary tract infection (UTI; 599.0); and pulmonary embolism (415.1x).
SAS software (SAS Institute, Cary, NC), version 9.4, was used for data analysis and statistics. The difference between the categorical variables were evaluated with the chi-square test and multi-variable logistic regression analysis with stepwise selection and adjustment by age, gender, race, co-morbidities (AHRQ co-morbid measures), and hospital characteristics such as hospital region (Northeast, Midwest, South, and West), location (urban/rural) and teaching status (teaching/non-teaching). All multi-variable models met the quality criteria. The data for the hospital length of stay (LOS) was not normally distributed and was skewed to the right. As a result, LOS was presented as a median with interquartile range Q1-Q3, and intergroup difference was tested with non-parametric Wilcoxon rank-sum test; p < 0.05 was considered significant. The study was approved by the Institutional Review Board of the Rutgers Robert Wood Johnson Medical School.
Results
A total of 809 (12.9%) patients with drug dependence (PDD) of the 6,264 patients who underwent VS were evaluated. As seen in Table 1, PDD were younger compared with control patients (39.0 ± 10.8 y vs. 54.4 ± 14.8 y; p < 0.0001), and these patients were primarily men and Caucasian versus Hispanic or African-American. They also had less age-related co-morbidities such as hypertension, diabetes mellitus, congestive heart failure, renal failure, obesity but greater rates of alcohol abuse, liver disease, and psychoses (Fig. 1). Despite the younger age and fewer co-morbidities, PDD compared with control patients were more likely to have post-operative complications develop overall (odds ratio [OR] = 1.6; 95% confidence interval [CI] 1.34–2.01), including infectious complications (OR = 1.5; 95% CI 1.27–1.78), specifically pneumonia (OR = 1.4; 95% CI 1.14–1.74) and sepsis (OR = 1.4; 95% CI 1.16–1.63). They also had more renal complications (OR = 1.5; 95% CI 1.23–1.77), and pulmonary embolism was more common (OR = 1.9; 95% CI 1.44–2.52) (Fig. 2). Further, PDD had 11% longer hospital length of stay than controls (p < 0.0001). We did not find significant difference in hospital deaths between these groups, however.

Co-morbidities in patients with and without drug abuse. CHF = congestive heart failure. Color image is available online at www.liebertpub.com/sur
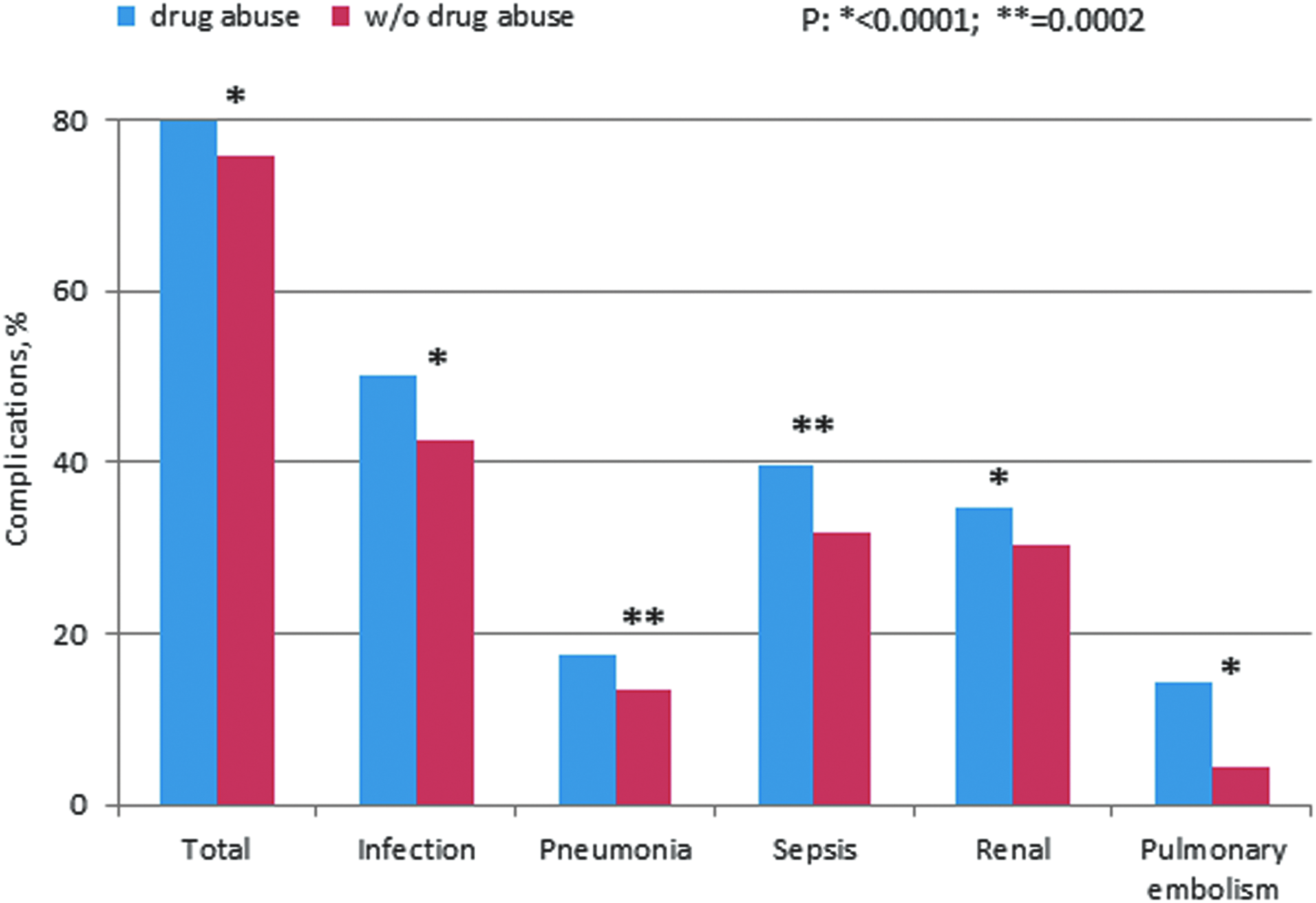
Complications in patients with and without drug abuse. Color image is available online at www.liebertpub.com/sur
IE = infectious endocarditis; VS, = valvular surgery; DD = drug abuse; SD = standard deviation.
Discussion
The diagnosis and management of IE remain challenges of clinical medicine. Patients with a history of IVDU in whom endocarditis develops should be treated uniquely. These patients are often younger and have fewer co-morbid conditions when compared with patients with IE from other etiologies. Our data show that patients with drug dependence have significantly worse post-operative outcomes when they have VS for IE. Specifically, the PDD compared with control patients were more likely to have post-operative complications develop. Further, they spent longer times in the hospital, which is associated with greater hospital costs and expenditure of resources.
Over the last few decades, there have been widespread changes in healthcare delivery, which have impacted the epidemiologic profile of the patients in whom IE develops. The increasing use of intra-cardiac devices, prosthetic valves, and hemodialysis has put more patients at risk of IE developing. Moreover, the growing elderly population with their intra-cardiac devices such as pacemakers has broadened the target population for IE with more patients being older [9–12]. Our findings are contrary to the notion that younger patients with fewer co-morbid conditions would have better outcomes. The elderly patients with more co-morbid conditions such as hypertension and diabetes mellitus had better outcomes than the younger PDD. Specifically, the older patients had fewer post-operative complications and spent less time in the hospital after surgical procedures. The PDD present particular management difficulties because of their drug seeking behavior and poor compliance treatment.
An explanation for these findings is multi-factorial. The PDD because of their history of IVDU often are found to have more complex social situations and may have more psychiatric issues as well. One finding that is critical is that these patients, who are younger, often have less social support and are less likely to have medical insurance. As a result, it is often more difficult to get these patients to rehabilitation centers. Often these patients require intravenous antibiotics for several weeks, and as a result, these patients often will require placement at facilities where their treatment can be monitored. In contrast, the older patients, although with more co-morbidities, often are employed with insurance and stable family situations. These patients can either be sent home with supportive spouses or because of their medical insurance be sent to nursing homes or rehabilitation centers. As a result, the PDD have longer length of stays.
An explanation for the increased complication rate of PDD can possibly be related to their history of drug use and the potential risk of end organ injury resulting from it. Second, the PDD patients are at a greater infection risk because of their longer length of stay in the hospital, which exposes them to other patients with infections. Moreover, these patients have a history of previous high-risk behavior such as the sharing of intravenous needles, which also could increase their infection rates.
Critical illness has a significant impact on a person's physical and mental health. The younger patients may not be able to handle the stress associated with their medical illness. In addition, age, co-morbidity, and frailty play a critical role in determining the long-term outcomes of patients requiring intensive care [13]. Perhaps one of the issues that may be contributing to the poorer outcomes for the patients with PDD is that these patients' critical illness negatively impacts their physical and mental health, which leads to a bad cycle that ultimately leads to poor long-term outcomes.
Intravenous drug users predominate in the younger population, and the overall incidence of IE in this group is 1%–5% per year [14]. The tricuspid valve is infected in >70% of patients, and the majority have no known pre-existing cardiac disease [15]. Staphylococcus aureus species predominate in this patient population, although unusual infections including Pseudomonas aeruginosa, fungi, Bartonella, Salmonella, and Listeria may also be encountered [16].
The study has several limitations that we would like to acknowledge affecting the interpretation of our study. First, as a retrospective study, we acknowledge the inherent issues that come with this form of study. In addition, as with prospective cohort studies, retrospective studies are not good for very rare diseases. Although IE is not extremely rare, it is not as common as coronary artery disease or cerebrovascular accidents. Further, there is frequently an absence of data on potential confounding factors if the data were recorded in the past.
This study is based on a review of a database that also has inherent shortcomings. First, follow-up is generally not as standardized as in randomized trials; therefore, ascertainment of outcomes may be incomplete. Second, because data collection for registries is often more passive than data collection in randomized trials, missing data may be a greater potential problem for registries. Despite these limitations, our data do demonstrate significant findings.
Taken together, our results indicate that there is an association between PDD and increased complications with IE. The association between the two should help healthcare providers treat their patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.