
Abstract
Abstract
Background:
Fulminant Clostridium difficile colitis (fCDC) occurs in 2%–8% of patients with CDC and carries a high death rate. Prompt operation may reduce death. Our aim was to determine whether a standardized hospital-wide protocol for surgical referral in CDC would result in earlier surgical consultation, earlier identification of patients who could benefit from surgical therapy, and reduced deaths from fCDC.
Methods:
A multidisciplinary team developed consensus criteria for surgical consultation. Compliance was evaluated by prospective review of all inpatient CDC cases. Outcomes of the prospective cohort (POST) were compared to an historic control group (PRE).
Results:
From November 1, 2010 to October 31, 2012, we identified 1,106 inpatients with CDC; 339 patients matched the consultation criteria, of whom 213 received a surgical consultation, resulting in an overall compliance rate of 62.8%. All those with fCDC received a surgical consultation, with a median time to surgical referral of three hours. Of 46 patients with fCDC, 11 (23.9%) died, compared with 34.8% in the historical control group (p = 0.15). The death rate was 14.7% in the POST group, when excluding patients with limitations of care and those transferred to our institution in a fulminant state. There was a shorter interval between admission and surgical intervention for those who required operation in the POST group—three (1–11) days versus 1.5 (0–3) days, respectively, in the PRE and POST groups (p = 0.018), and a shorter adjusted median hospital length of stay (adjusted difference 9.0, 95% CI 2.2–12.3, p = 0.007)
Conclusions:
A hospital-wide protocol with established criteria for surgical consultation resulted in faster intervention and a shorter adjusted median hospital length of stay. The overall death rate for fCDC patients without limitations of life-sustaining treatment who presented to our emergency department or in whom fCDC developed while they were admitted to our hospital was 14.7%.
C
We developed a hospital-wide protocol based on consensus-derived criteria for surgical referral of patients with CDC. We hypothesized that this protocol would result in earlier surgical consultation, earlier surgical treatment in fCDC patients requiring surgery, and reduced death from fCDC.
Methods
Design
This study has a before-after design across the time of implementation of a hospital-wide surgical referral protocol for patients with CDC. Data on fCDC patients after the protocol (POST group) were recorded prospectively. Data on fCDC patients before the protocol (PRE group) were extracted retrospectively [11].
Protocol development
The main sources of fCDC patients in our hospital are the general medical wards, the emergency department, and the medical intensive care unit. Between August and October 2010, we coordinated a series of meetings with representatives of these departments. Consensus was reached about appropriate criteria for surgical consultation based on predictors of death [11–13,17–19,25,28,29,31,33]. The resulting protocol called for immediate surgical consultation for patients with known or suspected CDC and any of the additional criteria listed in Table 1 indicating possible risk of progression to fCDC.
ICU = intensive care unit; WBC = white blood cell; bands = bandemia; HR = heart rate; BP = blood pressure.
Any two of the eight listed criteria.
The protocol initially called for consultation for every patient with a single criterion. At a four-month interim analysis, we found that there was no development of fCDC in patients with only one criterion. Within the multidisciplinary study group, it was decided that the threshold for consultation should be increased to two criteria. The consensus criteria for surgical consultation were disseminated through departmental meetings and conferences, the Massachusetts General Hospital intranet, and emails to staff members, fellows, and residents throughout September and October 2010. Starting November 1, 2010, the protocol was applied to all patients arriving to the emergency department or already hospitalized in any hospital unit.
Compliance with the protocol
To monitor compliance with the protocol, we prospectively identified all patients with positive C. difficile immunoassays from our Infection Control Registry, ascertained whether those patients reached the threshold of two criteria (or one criterion during the first four months of the study), and recorded whether a surgical consult was called. Compliance with the protocol was promoted through departmental meetings and conferences, and the intranet throughout the complete study period. In addition, the representatives from each department included in the study were charged with ongoing education to maintain compliance with the agreed on management protocol. Individual cases of non-consultation or delayed consultation were reviewed and fed back to the responsible clinicians by their department representatives.
Definitions and measurements
The CDC was defined by the identification of C. difficile in symptomatic patients using either the toxin A/B enzyme immunoassay or a PCR test for toxigenic C. difficile. Fulminant CDC was defined by the presence of septic shock [34], need for intubation or vasopressors, admission to the ICU because of CDC, need for colectomy, or death from CDC. Subtotal colectomy was performed in patients with fCDC who were determined to be in too toxic a state for a trial of non-operative therapy or were treated medically, but deemed to have failed medical therapy. In patients undergoing subtotal colectomy, CDC was confirmed by histopathologic analysis of the surgical specimen.
Data collection
The following data were collected prospectively from November 1, 2010 until October 31, 2012, for the POST group: Demographics; important co-morbidities, measured by the age-adjusted Charlson Comorbidity Index (CCI) [35]; history of hospitalization and antibiotic therapy during the two months before the current admission; previous CDC in the six months before the current admission; vital signs; physiologic parameters; abdominal examination findings; mental status; radiographic or endoscopic findings; medical intervention; surgical intervention; time interval between diagnosis (defined as a confirmed/suspected C. difficile infection and two positive criteria) and surgical consultation; time interval between diagnosis and surgical intervention; indication for surgical intervention; surgical findings; final pathology; ICU and hospital length of stay (LOS); death; admission source; admitting service; referral source; primary department that provided care; and discharge disposition.
We also recorded whether the patients had any limitations of care, defined as a refusal by the patient or legal representative to undergo operation or other life-sustaining treatments. Patients who were transitioned to comfort measures after failure of an aggressive course of treatment were not considered to have limitations of care. The same data were recorded for the PRE group (January 1, 1996 to December 31, 2007). The PRE group included all patients with a diagnosis of CDC during that period.
Outcomes
The primary outcome was in-hospital death. Secondary outcomes included ICU and hospital LOS, ICU-free days (30 d from the time of CDC diagnosis minus days admitted to the ICU), and time to surgical consultation and to operation. The time was measured from either arrival to the emergency department with CDC symptoms or the time from which patients met consultation criteria if they were already hospitalized for other reasons.
Statistical analysis
We compared the PRE and POST groups to identify differences in patient characteristics and outcomes. Subgroup analyses were performed based on surgical status (colectomy vs. no-colectomy) and admitting service (surgical vs. non-surgical). Continuous variables were summarized using mean ± standard deviation and compared by Student t-tests, when variables had normal-like distributions, or summarized using median with interquartiles and compared by Wilcoxon rank sum tests, when variables could not be assumed to be distributed normally. Categoric variables were summarized using frequency and percentage and compared by Fisher exact tests. In the multivariable analyses, logistic regression models were used to compare death while quantile regression models were used to compare hospital, ICU, and ICU-free LOS.
We compared the two groups controlling for age and all clinical factors that were significant at 0.1 level from the univariable analysis, which included CCI, immunosuppression, admission source, hospital transfer, and vancomycin use. We did not include white blood cell (WBC) count and serum albumin level; we believe these two variables may have been influenced by our intervention because patients in the PRE group may have been allowed to progress to higher WBC count and lower serum albumin level than patients in the POST cohort. Statistical significance was considered as a two-sided p < 0.05. All statistical analyses were performed using SAS version 9.4 (The SAS Institute, Cary, NC). This study was approved by our Institutional Review Board.
Results
Over a two-year period of prospective data collection, 1,106 patients had a positive toxin assay for C. difficile. Of those patients, 339 met our criteria for surgical consultation. A total of 213 patients were referred per protocol to the surgical service, resulting in a compliance rate of 62.8%. During the first four months of the study, when the threshold for surgical consultation required one criterion, compliance with the protocol was 53.6%. This increased to 65.2% after we changed the threshold for consultation to at least two criteria. Forty-eight patients with fCDC were included in the POST group. The overall incidence of fCDC in the POST group was 4.3% (48/1,106), compared with 4.1% (198/4,796) in the PRE group. We excluded two patients from the analysis who were treated with an experimental procedure (loop ileostomy with colonic lavage) as part of another research study. All 46 patients included in the analysis underwent surgical consultation, resulting in a compliance rate of 100% for patients with fCDC. The median time from diagnosis to consultation was three hours (interquartile range [IQR], 1–7.75 h). The majority of patients with fCDC met either four (34.8%) or five (26.1%) criteria on surgical consultation (Fig. 1).
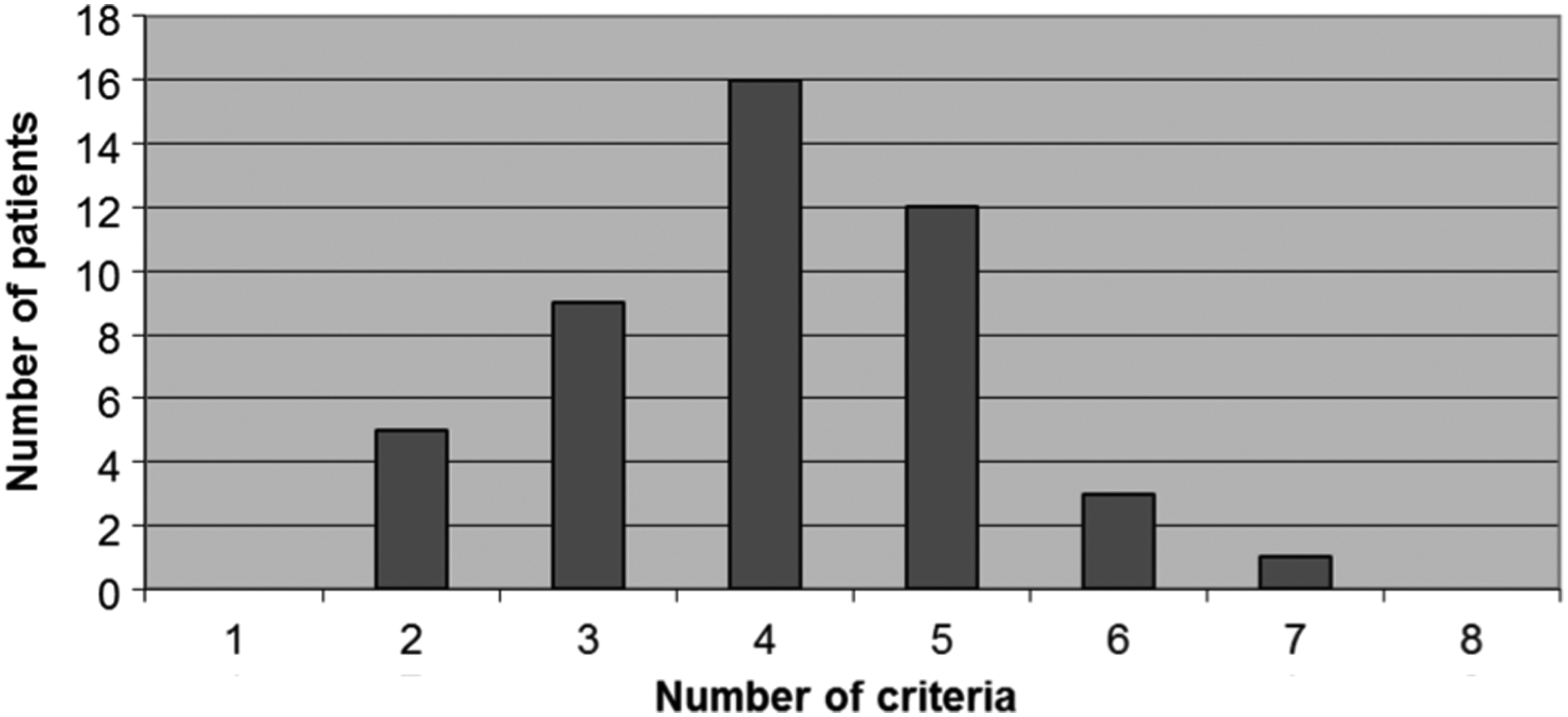
Number of criteria met by patients with fulminant Clostridium difficile colitis on surgical consultation.
Patient characteristics for both the PRE and POST groups can be found in Table 2. There was a higher age-adjusted CCI in the POST group, while the PRE group had a higher mean WBC count and lower mean serum albumin level. In addition, patients in the POST group were treated more often with enteral vancomycin. After our intervention, a higher percentage of patients were directly admitted to the surgical service, while there was also a shorter time interval between hospital admission and surgical intervention in patients undergoing surgery.
PRE = before implementation of surgical referral protocol; POST = after implementation of surgical referral protocol; SD = standard deviation; CCI = Charlson Comorbidity Index; WBC = white blood cell; CT = computed tomography; CDC = Clostridium difficile colitis; PO, per ora; IV, intravenous.
CT was not performed for 48 from the PRE group and 8 from the POST group.
All outcomes for both the PRE and POST groups are listed in Table 3. Death, our primary outcome, was decreased, although not statistically significant, after implementation of the protocol (34.8% vs. 23.9%, PRE vs. POST, p = 0.17). The death rate in the POST group, when excluding those with limitations of care, was 18.6% and dropped to 14.7% when excluding both patients with limitations of care and those transferred to our institution with pre-existing fCDC. Death was not significantly different between the PRE and POST groups in the multivariable logistic regression model (adjusted odds ratio [OR] = 0.74, 95% confidence interval [CI] 0.31–1.79, Table 4).
PRE = before implementation of surgical referral protocol; POST = after implementation of surgical referral protocol; IQ = interquartiles; ICU = intensive care unit.
Limited to the patients who received surgical intervention.
POST = after implementation of surgical referral protocol; PRE = before implementation of surgical referral protocol.
There were no significant differences in median hospital LOS, median ICU LOS, or median ICU-free days in univariable analysis (Table 3). After adjusting for the clinical factors listed in Table 4, there was a significantly shorter median hospital LOS (adjusted difference 9.0, 95% CI 2.2–12.3, p = 0.007) in the POST group, but no significant differences in median ICU-free LOS (adjusted difference 6.62.3 d longer, 95% CI 2.0-7.9-8.49.7, p = 0.66), or median ICU LOS (adjusted difference 1.6 days shorter, 95% CI −0.7–3.2, p = 0.27).
The percentage of patients undergoing subtotal colectomy with ileostomy did not differ significantly between the PRE and POST group (37.9% vs. 41.3% p = 0.67). Patients in the POST group were admitted to the ICU sooner after admission to the hospital than patients in the PRE group, while there was also a shorter interval between admission and surgical intervention for those who required surgery in the POST group (Table 3). In the PRE-group, the time intervals between hospital admission and surgical intervention and between ICU admission and surgical intervention (measured in days) were significantly shorter in patients admitted to the surgical service than to a non-surgical service. In the POST-group, such differences were not found. The death rate dropped significantly on the non-surgical services (37.5% PRE vs. 13% POST, p = 0.02), but at the same time, there was a trend toward higher deaths on the surgical service (20% PRE vs. 34.8% POST, p = 0.23).
Discussion
With three million new cases every year in the United States and rising prevalence, C. difficile is the leading cause of nosocomial diarrhea in both North America and Europe. C. difficile colitis is not only increasingly common but has also become more serious with the emergence of hypervirulent strains linked to increasing morbidity and death [1,6,8,11,15,28,36–39]. As serious infections have become more common, the role of surgical procedures in their management has been refined. Current guidelines recommend operation only for advanced disease, but recommend performing it before shock or irreversible organ damage has intervened [32].
Studies by Sailhamer et al [11], Hall and Berger [12], Seder et al. [31], and Ali et al. [17], suggest improved outcomes, including benefits regarding death, when surgical intervention is performed early in the course of fulminant disease. Still, a study from our own institution showed that surgical consultation was often undertaken relatively late, sometimes days after the occurrence of multi-system organ failure [11]. We found that our early surgical consultation initiative reduced the time to surgical consultation for patients with fCDC. It also reduced the time from hospital admission and ICU admission to operation for patients with fCDC undergoing surgery, but did not result in a statistically significant difference in deaths. While our intervention did not result in a significant reduction in deaths, it was associated with a reduced hospital LOS. While earlier surgical consultation may not have lowered deaths, earlier surgical consultation and, when necessary, colectomy, may have allowed survivors to recover more quickly.
Currently, there are no evidence-based guidelines for when to obtain surgical consultation in cases of CDC, although a number of risk factors for transition to fCDC have been identified. These include older age, profound leukocytosis, immunosuppression, inflammatory bowel disease, previous intravenous immunoglobulin treatment, surgery within 30 days of presentation with CDC, and evidence of peritonitis on physical examination [15,19,40]. Our consultation criteria were developed through multidisciplinary consensus and based largely on our own retrospective data [11,12]. Our priority was to identify patients in whom fulminant disease would develop, early in their course. We consciously developed criteria that we believed would be highly sensitive for fCDC, at the cost of some specificity. Hospital-wide compliance with our protocol was almost 65% over the 24-month study period. Although this may appear low, all patients in whom fCDC developed were caught early in their disease course, with a median time to surgical consultation of three hours, resulting in 100% compliance in that group, which was an important goal of our initiative.
There was a trend toward decreased deaths in our POST cohort in both univariable and multivariable analysis, but it was not statistically significant. The unadjusted death rate was 23.9% in the new cohort. This dropped to 14.7% when excluding patients with limitations of care and those transferred to our center in a fulminant state. We believe this latter exclusion is relevant, because an early referral protocol would not be expected to have as significant an effect on death in this population. This is among the lowest death rates reported in the literature; most studies report death rates between 35% and 55% [8,11,16–19,21,22,24–26,29–31].
In patients who required a total abdominal colectomy, the time interval between hospital admission and surgical intervention was measured, because multiple studies have suggested improved outcomes with shortened intervals [13,17,18,25]. Compared with the PRE cohort, the time interval from admission to surgical intervention was cut in half (median of 1.5 d vs. 3 d, p = 0.024) for patients requiring colectomy, without increasing the overall percentage of fCDC patients undergoing colectomy (37.9% PRE vs. 41.3% POST). The fact that approximately the same number of patients underwent colectomy suggests that early surgical consultation does not necessarily lead to increased rates of colectomy.
There has also been debate in the literature about whether patient outcomes could be improved by direct admission to a surgical service in CDC cases [11,13,17,18,25]. Sailhamer et al. [11] showed a lower death rate in patients admitted to a surgical versus a non-surgical service (12.8% vs. 39.3%), both in all CDC patients, and in those undergoing colectomy. A study by Byrn et al [13], however, showed no difference in death based on admitting service. Our results showed a significantly higher percentage of fCDC patients directly admitted to the surgical service after implementation of the protocol (15.2% PRE vs. 50% POST, p = < 0.001), but no differences in outcomes.
When comparing PRE versus POST implementation of the protocol, the death rate within the medical service significantly decreased, while there was a trend toward increasing deaths on the surgical service. This can be explained in two ways. First, because of our intervention, patients admitted to non-surgical services in the POST group were more likely to have early surgical consultation and any associated benefits. Second, it is probable that in the PRE cohort, a highly selected subgroup of patients likely to benefit from operation were the only ones admitted directly to the surgical service. This is in contrast with the POST cohort, where early surgical consultation resulted in more surgical admissions, even for patients unlikely to undergo operation. This second contention is supported by the fact that in the PRE cohort, 66.7% of patients admitted to the surgical service underwent colectomy, compared with only 52.2% of patients in the POST cohort. It is likely that patients with CDC can be treated equally effectively on either a surgical or medical service as long as appropriate medical therapy is administered, close communication is maintained, and the need for surgical intervention is constantly re-evaluated.
Our study has a number of limitations. Our primary intervention was only adhered to 65% of the time. As discussed above, we accepted a lower specificity in the consultation criteria in the effort to capture all cases with the potential to progress to fCDC. We included all CDC patients in the analysis, not just those for whom surgical consultation was obtained; thus, the entire prospective POST cohort can be considered on an intention-to-treat basis. Further studies could seek to identify the most important criteria or factors associated with the transition to fCDC to further refine the consultation criteria.
Although our POST cohort was identified prospectively, it was compared with historic controls collected over years during which the epidemiology and management of CDC evolved considerably. General advances in critical care in recent years would tend to bias the results in favor of our intervention, suggesting a benefit to early surgical consultation that may not exist. Similarly, general trends in care aimed toward reducing LOS may have contributed to the reduced adjusted hospital LOS in our POST cohort. Conversely, the preponderance of more virulent C. difficile strains in recent years might bias the results against our intervention. We controlled for patient co-morbidities and enteral vancomycin use among other factors, but given the lack of complete microbiologic data on specific C. difficile strains and resistance patterns, we could not adequately control for all of these confounders. In addition, our institution has generated publications advocating early surgical consultation in CDC from both our general surgery and trauma and acute care surgery services [11,12]. A relatively low pre-intervention death rate and an institutional environment in which awareness of the importance of surgical consultation in CDC may have been higher than normal even before our intervention would both bias our results toward the null hypothesis.
Our study showed that a hospital-wide protocol with established criteria for surgical consultation decreased the time to surgical consultation in patients with fCDC and reduced the time from hospital and ICU admission to operation in patients requiring surgical procedures. In spite of an association with relatively low overall deaths from fCDC, our early consultation protocol itself did not independently and significantly reduce deaths. Our intervention, however, was associated with a markedly reduced LOS, suggesting that our protocol may have significantly improved recovery. Further studies are required to define the optimal role for surgical consultation and intervention in this deadly disease.
Footnotes
Author Disclosure Statement
No competing financial interests exist.