
Abstract
Abstract
Background:
Soft tissue infections are a common reason for general surgical consultation. Necrotizing soft tissue infections (NSTI) are a rapidly progressive form of this infection that account for significant morbidity and many deaths.
Methods:
Review of relevant English-language publications.
Results:
There are approximately 500–1,500 cases of NSTI annually in the United States, although accurate estimates of their frequency are difficult to obtain. These infections may be polymicrobial or monomicrobial, and substantial regional heterogeneity exists regarding anatomic location and the involved organisms. Source control with early surgical debridement and targeted anti-microbial therapy are the mainstays of treatment.
Conclusion:
Necrotizing soft tissue infections remain a common indication for general surgical consultation. Early diagnosis and prompt surgical treatment are essential for effective control.
N
History
As alluded to above, NSTI have been recognized for centuries as a rapidly progressive and frequently fatal disease. The earliest descriptions were provided by Hippocrates [1,2], and cases of NSTI have been described in medical writings by numerous authors since that time [3]. Fournier published his description of the disease that bears his name in the late 19th Century [4], and the Civil War provided numerous cases of “hospital gangrene” in the U.S. [1,2,5]. The term “necrotizing fasciitis,” perhaps the most frequently used reference for this condition by physicians in all areas of medicine, generally is attributed to Wilson [1,2,5]. Recently, the more generic term “necrotizing soft tissue infection” (NSTI) has become popular to describe progressive infections of all layers of the soft tissue regardless of body location [6]. As will be described, however, there often are distinct etiologies and differences in microbiology for NSTIs in different regions of the body. These infections are the most severe subset of skin and soft tissue infections and, for standardization in clinical trials, are classified as “complicated” by virtue of their involvement of deeper soft tissue layers [7].
Epidemiology
Reliable epidemiologic studies of NSTI are difficult to find, so the true incidence can only be estimated. The numerous International Classification of Diseases, 9th Revision codes that can be applied to fasciitis or gangrene complicate coding of the disease by medical records abstractors, so using large administrative datasets is challenging.
It has been estimated that there are between 500–1,500 cases of NSTI in the U.S. [1,2,5], 500 cases in the United Kingdom [8], and as many as 200 cases in Canada [3] annually. The U.S. Centers for Disease Control and Prevention (CDC) tracks cases of invasive Group A Streptococcus (GAS) infections from selected reporting areas and estimates that there are 650–800 cases of necrotizing fasciitis yearly caused by these organisms [9]. As will be described, there is a great deal of regional heterogeneity in the microbiology of the organisms causing NSTI, so the true incidence of polymicrobial NSTI or non-GAS monomicrobial NSTI is even more difficult to determine.
Necrotizing soft tissue infection can be classified according to anatomic location (extremity, perineum, trunk), the invading organism, or, less commonly, the depth of invasion [1–5,10]. Depth of invasion is less useful for classification because, by definition, NSTIs involve deeper structures and exclude simple skin infections (cellulitis) or localized subcutaneous infections (abscesses). Whether superficial fascia or the deeper fascia investing muscle layers is involved is determined at the time of surgical debridement and is an important factor in defining the extent of debridement but is not particularly helpful in determining the severity of disease.
The anatomic location and the microbiology of the infection are intimately related when classifying NSTI. Type I NSTI are polymicrobial, frequently involving a mixture of gram-positive cocci, enteric gram-negative bacilli, and possibly anaerobes [1,2,5]. Necrotizing infections of the trunk and perineum are typical examples of Type I NSTI and often occur in patients with numerous medical co-morbidities such as obesity, diabetes mellitus, vascular disease, renal insufficiency, immunosuppression, or cirrhosis [1,2,5]. Historical causes of Type I NSTI of the trunk and perineum such as urinary strictures, instrumentation of the urinary tract, or recent operative procedures seem to be less frequent sources of NSTI today. More commonly, other inciting medical problems such as infected cysts, furuncles, or subcutaneous abscesses are associated with progression to NSTI. However, advanced or neglected gastrointestinal perforations or infected post-operative incisions can present as NSTI and should be kept in mind. Depending on the population of patients involved or referral patterns, Type I NSTI also can occur in the extremity and include cases of progressive or neglected lesions in diabetic patients with peripheral vascular disease (Fig. 1).

Polymicrobial necrotizing soft tissue infection originating in a diabetic foot lesion. The extensive medial eschar and bullae at the lateral malleolus indicate advanced disease. Distant proximal extension associated with severe sepsis necessitated amputation.
Type II NSTIs are monomicrobial and frequently involve the extremities. Necrotizing infections caused by GAS or Staphylococcus aureus are typical examples of Type II NSTI [1,2,5]. These NSTIs frequently are associated with some sort of inciting event such as a puncture wound, intravenous drug injection, or other traumatic injury leading to introduction of the organism into deeper tissues. For Type II NSTI, Streptococcus is the most common organism reported, but local population factors and regional referral patterns will dictate the predominant organism in many institutions. Some authors have reported more staphylococcal than streptococcal NSTIs [11,12] Other authors have reported increasing numbers of NSTIs caused by methicillin-resistant S. aureus (MRSA) [13]. Kao et al. found MRSA to be the most common organism in Type II NSTIs in their area [14].
Necrotizing soft tissue infections caused by marine organisms commonly are classified as Type III [1,2,5], although some authorities have classified clostridial myonecrosis as Type III NSTI [5]. Type III NSTIs caused by marine organisms are more common in Asia, where Vibrio organisms are endemic [12,15]. However, having recently seen a case of NSTI caused by invasive Vibrio infection in our institution in a restaurant employee working with shellfish, we caution that it bears keeping these unusual organisms in mind for all cases of NSTI. Type III NSTI often are associated with an inciting traumatic event introducing the organism into an extremity such as skin puncture from a marine organism or other type of injury, but NSTI associated with shellfish ingestion also has been reported [12]. Hepatic cirrhosis is associated with marine Type III NSTI [1,12], but the reason for this association is unclear. Whether cirrhosis predisposes to Type III NSTI or whether this association is attributable to cirrhosis from hepatitis being endemic to the same areas as Vibrio infections has not been defined.
Some authors have described a Type IV NSTI caused by fungal infections, but NSTI attributable to fungus is exceedingly rare, occurring most often in immunocompromised hosts. Necrotizing soft tissue infection caused by traumatically introduced Aspergillus or zygomycetes has been reported [15,16].
Much of the conflicting information on the microbiology and epidemiology of NSTI appears to stem from the substantial heterogeneity in anatomic location and microbiology for NSTI observed in different medical centers. Even in the same metropolitan area, substantial institutional variation is observed in the location of NSTI and the organisms involved [14]. This undoubtedly is secondary to a combination of local environmental factors, local and regional referral patterns, and population characteristics [3,15]. These regional differences likely are responsible for the wide variability in the frequency of different types of NSTI. Type I NSTI has been reported to account for 10%–80% of all NSTIs in different series. Whereas some areas report a preponderance of monomicrobial upper-extremity NSTIs [17], others see a greater incidence of polymicrobial truncal NSTIs [11,15]. Predicting future patients and the organisms involved in NSTI at any institution may be achieved best by reviewing past facility experience.
Diagnosis
A high index of suspicion for the presence of an NSTI is critical, because delays in treatment are associated with greater mortality rates [12]. As discussed above, a history of an inciting medical event such as a simple abscess or a portal of entry from a puncture or other injury often can be elicited but is infrequently diagnostic in differentiating NSTI from a simple abscess or cellulitis. A history of erythema, swelling, and pain are common with NSTI, whereas blisters/bullae, necrotic eschars, or a history of drainage are warning signs of more advanced disease [1] (Fig. 2). Pain frequently is out of proportion to the physical examination findings, and erythema that has progressed despite antibiotic therapy is a cause for serious concern [6,10].

Bullae, necrotic skin changes, and edema are evident in this polymicrobial perineal necrotizing soft tissue infection (NSTI). This obese patient had many of the medical co-morbidities frequently associated with truncal Type 1 NSTI. Note the left groin scar from a prior perineal NSTI.
Physical examination findings can be subtle, and visible external signs often are minimal or unimpressive despite substantial deeper tissue involvement. Erythema, violaceous skin changes, and bullae may be visible in advanced disease (Fig. 3). Brawny or woody induration of the subcutaneous tissues can distinguish NSTI from simple cellulitis, and, as discussed above, tenderness to palpation out of proportion to visible abnormalities is noted frequently. Crepitus may be evident in advanced cases or in infections caused by anaerobic organisms [2]. Signs of systemic shock or sepsis should prompt aggressive evaluation for NSTI regardless of the minor nature of other clinical features, especially if no other source of infection is identified.

Extensive blisters/bullae and violaceous skin changes associated with rapidly progressive and advanced NSTI.
Laboratory values often are non-specific, revealing leukocytosis and bandemia, and are consistent with an infection but do not identify the etiology. Laboratory findings that reflect the severity of illness, such as dehydration, metabolic acidosis, and organ dysfunction, also are nonspecific but should raise concern about a substantial systemic illness and the presence of an NSTI. A scoring system, the Laboratory Risk Index for Necrotizing Fasciitis (LRINEC), has been derived from several common laboratory values (white blood cell count and hemoglobin, sodium, creatinine, and glucose concentrations) and showed good predictive ability for NSTI [18]. However, the LRINEC is heavily weighted toward C-reactive protein values [18], which are measured infrequently by many surgeons when evaluating patients with a suspected NSTI. Also, this score has not been validated by other investigators.
Radiographic studies to help diagnose NSTI have met with limited success. Plain radiographs, ultrasound scans, computed tomography scans, and magnetic resonance imaging can demonstrate subcutaneous air (Fig. 4), infiltration of deeper tissues, fluid between tissue planes, and thickening of fascial layers, which should heighten one's suspicion for an NSTI. These findings are useful when present, but their absence does not exclude NSTI, and they have low specificity [6]. In our experience, radiographic studies are more commonly ordered by non-surgeons such as internists or emergency medicine physicians and in many cases are diagnostic when confirmatory clinical findings are evident on physical examination.
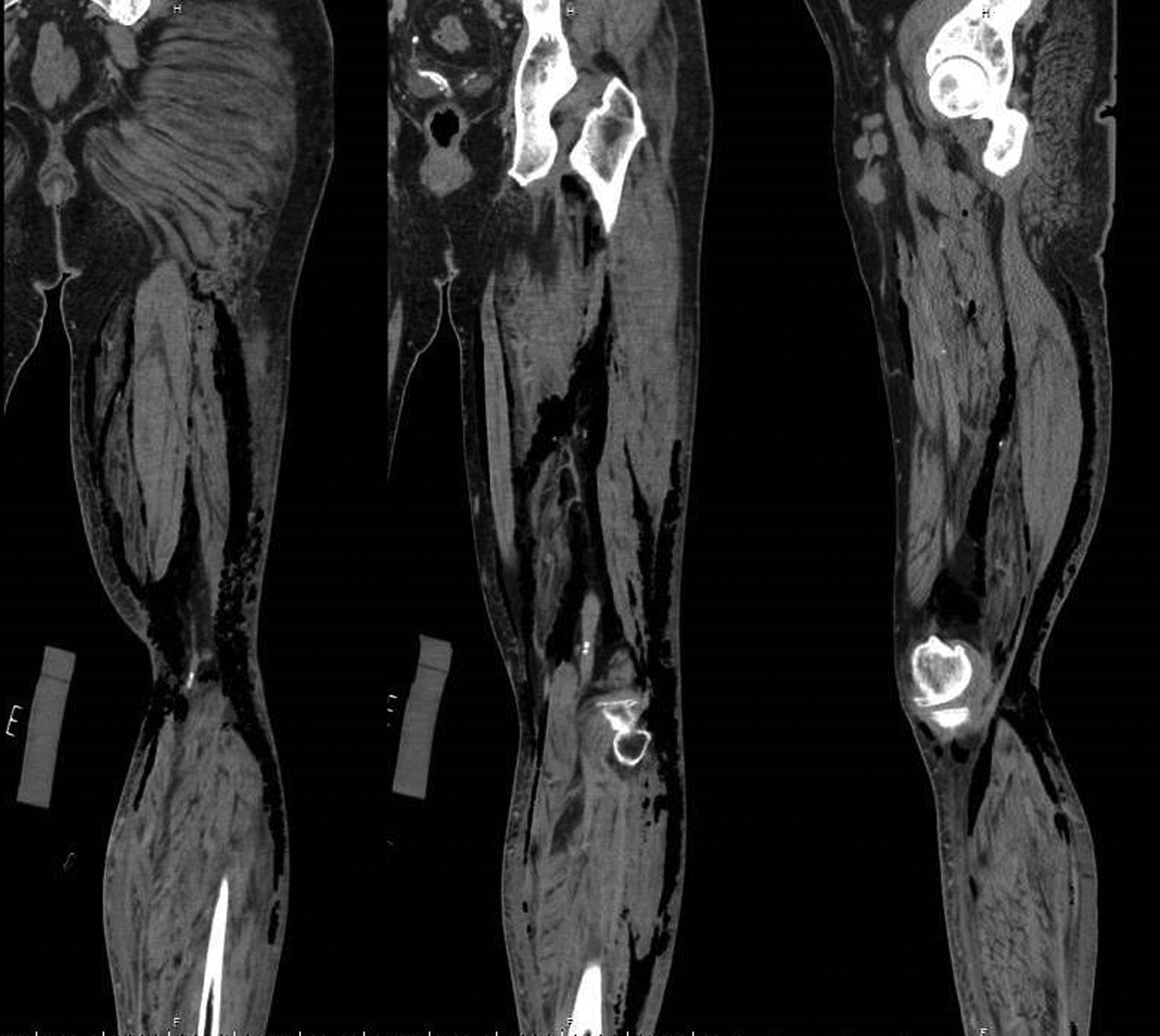
Subcutaneous air demonstrated on computed tomography scan in a patient with a clinically obvious necrotizing infection of the extremity.
A high index of suspicion for an NSTI and early consultation with an experienced surgeon probably is the most effective diagnostic modality. Despite the fact that delays in treatment are associated with a greater mortality rate [12], visible progression of the disease can be rapid (up to 2.5 cm/h)[3], and frequently, the diagnosis is obvious by the time the surgeon becomes involved. For equivocal cases, surgical exploration may be indicated to assess the integrity of the deeper tissues in order to avoid further delay or misdiagnosis. The presence of a foul odor, edema, purulence, necrotic tissue, thrombosed perforating vessels, dishwater drainage, or loss of the normal adherence of tissue layers are operative findings consistent with an NSTI. Microscopic evaluation and frozen-section pathologic assessment have been suggested as useful in making the diagnosis of NSTI [2,15], but we have not found these measures necessary or useful, as other clinical and operative findings typically confirm the diagnosis.
Treatment
The essential components of treatment of NSTI have remained the same for a long time: Antimicrobial therapy directed against the most likely pathogens, prompt surgical debridement, and aggressive supportive care [10,19,20]. The extent of debridement should include all clearly nonviable, necrotic, and grossly infected tissue back to healthy, bleeding, viable tissue. Visibly normal-appearing skin may need to be removed if there is extensive deep tissue involvement. Tissues where the normal adherence of subcutaneous layers to fascia has been lost generally mark continued involvement and usually will need to be excised up to a point where normal tissue integrity is restored. Excision down to and often including the fascia can be required, and involvement of deeper layers of fascia investing muscle groups occasionally is found. For extremity NSTI, an assessment of the magnitude of systemic illness, the extent of debridement required, and the likelihood of a functional extremity are factors to consider when determining if amputation will be required for source control.
Regardless of the location of the NSTI, consideration of future function or reconstruction may be useful early but should not be the dominant consideration in determining the extent of debridement. Source control is of paramount importance and can be achieved only by effective tissue removal. Given the progressive nature of NSTI, a single debridement often is not adequate. Several authors report a mean of two to seven procedures per NSTI to achieve adequate infection control [14,17,21–24]. The timing of re-debridement and rapid achievement of source control may impact the final outcome [25]. During the initial debridement, samples should be obtained for culture to help direct future antibiotic therapy. If localized fluid collections are present, the fluid can be submitted. Cutaneous swabs may not yield reliable culture results, and we prefer to submit tissue obtained from deeper, obviously involved areas for culture.
Antimicrobial therapy directed against the organisms likely to be involved is an important component of therapy, and empiric broad-spectrum coverage should be given until more specific culture information is obtained. Guidelines have been created to help guide initial antibiotic selection, and combinations of agents may be desirable [19,20]. Agents that inhibit production of toxins from Clostridium or Streptococcus are favored by some surgeons [26]. As discussed above, however, substantial regional variability exists regarding the anatomic site of NSTI, likely etiology, and most common infecting organisms. Therefore, local experience should play a role in initial antibiotic selection. The increasing frequency of community-acquired MRSA infections leading to NSTI also may need to be considered [13]. Once culture data are available, de-escalation of therapy to target only the specific organism(s) involved is recommended.
Although selection of antibiotic therapy is evidence based, there are no good studies identifying the optimal duration of such therapy. The duration of antibiotic administration is rarely described or controlled for in retrospective studies of NSTI. The recommendation to continue antibiotics until regular debridements are no longer required, clinical improvement has occurred, and fever has been resolved for 48–72 h is reasonable [19,20]. For subjects who remain critically ill or develop multiple organ dysfunction, these goals may be difficult to achieve. The appearance of the site and evidence of source control will support cessation of antibiotic therapy and should, in general, be achieved by 10–14 d.
Site Care
Site care for patients with NSTI can be complex, depending on the anatomic location of the infection and the extent of debridement necessary. Most NSTIs are cared for in facilities that are not burn centers [27] and therefore may have variable experience in dealing with large, complex dressing changes. Knowledge of local resources is essential to establishing an effective site care program for NSTI. The extent of the infection and associated other clinical factors such as critical care resources will dictate how frequent and in what location (floor, intensive care unit [ICU], operating room) dressings can be placed safely with adequate pain control and ensured patient safety. An optimal site care regimen for NSTI has not been defined clearly. Even when the extent of deep soft tissue involvement is less than anticipated, the nature of NSTI mandates that the site be left open for drainage. Whether topical antiseptics (sodium hypochlorite, iodine, silver nitrate) provide any advantage over simple saline wet-to-dry gauze dressings has not been established. Topical antiseptics or enzymatic agents certainly should not be relied on in lieu of adequate surgical debridement. In vitro data demonstrating the cytotoxic properties of topical antiseptics do not appear to be relevant to clinical sites of NSTI [28], and there is no proved advantage to their use.
Site care with vacuum-assisted (VAC) devices has become increasingly popular [29]. Whether VAC devices accelerate healing and re-epithelialization in sites affected by NSTI has not been established. In our experience, VAC devices have both advantages and disadvantages that should be tailored to the clinical features of the specific case. The VAC dressings need be applied only every second or third day, decreasing bedside dressing frequency and its potential discomfort. They may therefore be less painful on the non-dressing days. Such dressings tend to be associated with substantial discomfort on the day of changes, require experienced personnel for their application, may limit freedom of movement because of the hose/suction apparatus, and may be problematic in body areas such as the groin or perineum, where skin folds make application of the adhesive difficult.
Once a clean healing site is present, the options for closure and reconstruction can be considered. Groin and perineal sites, depending on the magnitude of the lesion and patient body habitus, often can be allowed to heal by secondary intention if they are small, there is excess subcutaneous tissue, and the lesions run parallel to natural tissue creases so that the site edges fall toward each other. Selected lesions such as small sites on the extremity can be closed with delayed primary techniques, although in our experience, this form of closure is seldom appropriate. The most common method of reconstruction is application of split-thickness skin grafts, which can be applied to any anatomic location once the recipient bed is properly prepared.
Adjuncts
Hyperbaric oxygen (HBO) therapy has been investigated as an adjunct to standard surgical debridement and antimicrobial therapy for NSTI. The theoretical benefit of HBO makes sense, particularly if anaerobes such as clostridia are involved. Although clostridial infections may be common in specific geographic areas [17], they are not an exceedingly common organism in most modern reports compared with historical series [1]. Hyperbaric oxygen has been suggested to be beneficial [10], and may be applicable, in selected cases where the extent of operative debridement may be limited, such as NSTI involving the face and neck [30]. However, most larger series have demonstrated no ability of HBO to improve the outcome of NSTI [31,32].
Intravenous immunoglobulin (IVIG) has been postulated to be a useful adjunct for NSTI, particularly those infections caused by GAS and associated with severe systemic illness or toxic shock syndrome [33]. This use of IVIG is considered “off label,” as the product has not been approved for this indication by the U.S. Food and Drug Administration. In a review of five ICUs in Canada, NSTI was the most common indication for IVIG use [34]. Intravenous immunoglobulin binds the exotoxin produced by GAS. However, IVIG is pooled from a large number of donors, so there is no way to standardize the quantity of the various antibodies present, and different IVIG preparations have different binding effectiveness for GAS exotoxin [35]. Some studies suggest a benefit for IVIG in NSTI, but these generally are uncontrolled studies with small numbers of patients [36]. Although the theoretical utility of IVIG in patients with GAS NSTI may be valid [33], evidence of efficacy is absent, and utilization of IVIG remains sporadic [37]. The immunoglobulin may be useful in subsets of patients with GAS NSTI or, similar to HBO, in patients with NSTI of the head and face, where the extent of debridement may be limited [6,38].
Another adjunct to treatment recently described is a peptide that interferes with binding of exotoxins to activating receptors on lymphocytes [39]. A Phase 2 study was published recently from a multi-center study involving 40 subjects with NSTI. This new peptide appeared to be safe with no substantial adverse events [39]. The study was not powered to evaluate outcome differences, and further trials are in progress to determine its efficacy.
Supportive Care
Aggressive supportive care during resuscitation from the acute insult and throughout the ICU stay is essential to minimize organ dysfunction and prevent additional complications. Advances in the support of critically ill patients have improved the outcome of patients with NSTI dramatically, including better resuscitation, metabolic support, and nutritional therapy. The numerous advances in critical care support cannot be described adequately in this review but may be the most important factor responsible for the better outcomes of NSTI in recent reports.
Outcomes
Survival from NSTI historically has been characterized as dismal, with mortality rates reported as high as 50%–60% in older series and 20%–30% in more recent reviews [1,2,5,6,12,23]. However, the most recent series report overall mortality rates of 7.6%–16.6% [11,14,24,40–42]. Two large national databases had mortality rates of 10.9% and 12% [27,40].
The morbidity associated with NSTI can be substantial and is related to the extent of surgical debridement required, need for amputation, severity of the systemic illness, and development of multi-organ dysfunction, as well as the frequent medical co-morbidities already present in many NSTI patients. Few studies on long-term outcomes have been reported. One study documented a greater risk of death after recovering from an episode of NSTI at a mean follow-up of 3.3 years [43]. Whether this greater risk was attributable to the frequent associated medical co-morbidities many patients with NSTI have or to some genetic predisposition to infectious problems could not be identified in this analysis [43]. The cost of hospital care for patients with NSTI is substantial [27], and the long-term costs and disability can only be estimated.
Conclusions
Necrotizing soft tissue infections remain a relatively uncommon disease that is associated with substantial morbidity and many deaths. Despite substantial regional differences in the location of NSTIs and the causative organisms, the basic treatment principles are similar. Early empiric antibiotic therapy, source control with surgical debridement, and aggressive supportive care are essential. Mortality rates from this disease appear to be improving, likely because of earlier recognition of the disease, aggressive management, and refinements in critical care support.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest to disclose.