
Abstract
Abstract
Background:
Organisms trapped in biofilms cause more than 80% of medical infections. Significant investments are being made to develop methods of removing these biofilms. The endOclear® device is reported to remove biofilm from endotracheal tubes (ETTs) and to decrease pneumonia rates and ventilator time.
Methods:
This was an observational study performed at a university Level 1 trauma center intensive care unit. A series of 40 ETTs were collected at extubation, with half of the patients having been treated daily with the endOclear® device. Biofilms were quantified from a standardized point on the distal ETT. The patients' standard and biofilm cultures were reviewed.
Results:
The mean hours of intubation for the control group was 135 and for the device group 138. This difference was not statistically significant (p = 0.91). Eleven patients in the device group were found to have pneumonia compared with six in the control group (p = 0.34). Ventilator data after device use showed a mean increase of 29.9 cc in tidal volume and a mean decrease in peak pressures of 0.39 cm H2O. Comparisons between biofilm stage or hours of intubation and a diagnosis of pneumonia found no correlation. Only nine of 40 ETTs had congruence between the microbiata of the biofilm and standard bronchoalveolar lavage (BAL) fluid, a divergence rate of 78%.
Conclusions:
Comparison of the endOclear® group and controls demonstrated a trend toward a higher pneumonia rate in the former. Additionally, the device achieved very small, clinically insignificant, changes in ventilator settings, and no difference was seen in the time on the ventilator. Comparisons between biofilm and standard BAL cultures continue to show the biofilm is more diverse than previously thought. In this study, no statistical significance was found between biofilm stage and the pneumonia rate. This study provides additional evidence that there is no correlation between biofilm stage and duration of intubation.
B
One of the most important survival characteristics of bacteria in biofilms is that they can evade host defenses and withstand antimicrobial chemotherapy through the use of a glycocalyx coating or extracellular polymeric substance (EPS) [14]. The difficulty in studying biofilms hinges on their unique architecture and this protective coating. Routine microbiologic techniques, such as aspirates, can identify only planktonic (free-floating) bacteria, not the sessile (biofilm-incorporated) bacteria. These bacteria are commonly cultured from within the accretions found inside an endotracheal tube (ETT). The accretions are not representative of the biofilm or the bacteria present therein. The sessile bacteria and surrounding protective glycocalyx are the major component of the biofilm. The resulting architecture and coating make the biofilm strongly adherent to surfaces such as ETTs. As a result, the biofilm is resistant to breakdown except by mechanical debridement or sonication. To better understand the complex infections we encounter in healthcare, a better understanding of biofilms is necessary.
Endotracheal tubes are an area of biofilm research that continues to develop. The tubes are a target for infectious as well as mechanical research. Analysis of extubated ETTs reveals that biofilms form in as little as a few hours of intubation [15,16]. Advanced biofilm stage is associated with pneumonia, but the duration of intubation does not predict biofilm stage [16]. Accretions that line the internal aspect of the ETT are not cleared by routine suctioning [17]. These accretions cause significant increases in drug resistance in ETT-associated bacteria. Wilson et al. demonstrated greater resistance across the tube, to as much as 20 cm H2O, which may increase the work of breathing or pressures on the ventilator and ultimately can influence providers' decisions on the timing of extubation.
Because of the greater present knowledge of biofilms in medicine, new devices are beginning to be tailored specifically for the removal of these films. There are multiple new devices that are reported to decrease accretions and biofilms on the internal aspect of an ETT in the hope of reducing tube resistance and the likelihood of pneumonia. One U.S. Food and Drug Administration-approved device is the endOclear®. This device is inserted through the ETT, after which a wiper is deployed and the instrument withdrawn. As it is withdrawn, it pulls mucous, and theoretically biofilm, back to the end of the ETT, where it can be removed (Fig. 1).
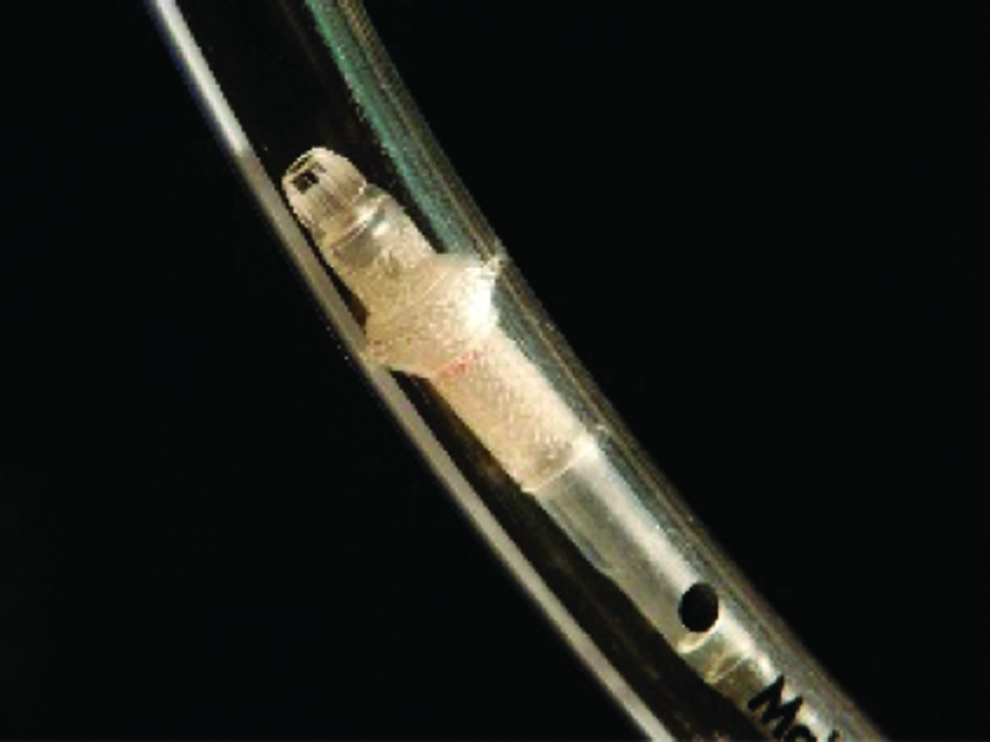
endOclear device with wiper deployed. Color images available online at www.liebertpub.com/sur
There were three aims of this study. The first was to evaluate the effect on ventilator pressures after the endOclear® device was used to remove the internal debris from the ETT. The second was to compare ETTs after extubation in patients in whom an endOclear® device was used vs. in those who had standard care. The third was to define and describe the characteristics of the biofilms that remained in the ETTs treated by the two methods.
Patients and Methods
Patients and ETTs
This study was conducted at West Virginia University and was approved by the Institutional Review Board (KC#1302021546). It was performed as a nested observational study within a broader evaluation of biofilms in ETTs in the intensive care unit (ICU). The study population consisted of adult surgical and medical critical care patients who were intubated. For each ETT, the following clinical data were collected: Patient age, weight, primary diagnosis, smoking status, bacterial cultures, hours of ventilation, ICU length of stay, and development of pneumonia. Using the U.S. Centers for Disease Control and Prevention Guidelines for PNEU2, pneumonia was defined as a new infiltrate on chest radiograph, fever, leukocytosis, or leukopenia and a positive quantitative culture.
Forty ETTs were collected. The first 20 were collected consecutively from patients whose care included the daily use of the endOclear device. Another twenty (control) ETTs were collected from patients who had not had the device used. All tubes were obtained after extubation, and no ETT was removed for the sole purpose of this study. After removal by a respiratory therapist, the ETT was placed immediately in a biohazard bag with a piece of gauze wetted with 4 mL of sterile saline to maintain appropriate hydration. Both the date and time were noted on the bag, and an abstractor was called to collect the sample. All samples were sealed and were delivered to the laboratory within two hours of extubation. All patient identifiers were removed, and a study number was used to track the sample. All data and statistics were evaluated by a biostatistician.
Clearing device methods
The endOclear® device was instituted as a respiratory protocol as an aspect of the routine ventilator checks done by the therapist. Patients who were mechanically ventilated for longer than 24 h had their tubes cleaned daily using the endOclear® device at a standard time each day. The respiratory therapists followed a standardized process for utilizing the device, strictly following the instructions for use provided by the manufacturer. All therapists had passed a competency test prior to being credentialed to use the device. The therapist documented the ventilator settings and the pressures before and immediately after use of the device. The amount of accretions removed was quantified and documented. Data collected before and after the device use included the peak inspiratory pressure, tidal volume, and airway resistance.
Bacterial identification
Biofilm harvesting for culture was performed using a finger scalpel to scrape a section of sample into 1 mL of phosphate-buffered saline (PBS). This section was determined by measuring the ETT and cutting the tube into three equal sections: Proximal, middle, and distal. Measuring from the distal end of the middle piece, a 1-cm section was removed for testing. After rinsing this cut section in 0.9% physiologic saline, both the inner and outer lumens of the ETT were scraped. Once this was completed, the sample was placed in a 40-KHz sweep frequency sonic bath (Fisher Scientific, Pittsburgh, PA) for 5 min. This low-frequency sonication helps to remove any biofilm remaining on the ETT and breaks up any biofilm aggregates in preparation for culturing. Sample culturing was performed in accordance with standard clinical microbiology methods [18].
Confocal laser scanning microscopy
Biofilm visualization was performed to establish the stage of the biofilm. Using two fluorescent nucleic acid stains, we were able to examine both bacteria and glycocalyx. Images were acquired point-by-point and reconstructed with a computer, allowing three-dimensional reconstructions of topologically complex biofilms so that height and depth could be measured. A 3-mm biopsy punch (Integra® Miltex®, Plainsboro, NJ) was used to cut a consistent sample from the now-distal end of the middle section of each ETT and fixed in buffered Formalin for four h. Samples were rinsed and then stained using SYTO 9 green fluorescent nucleic acid stain for biofilm visualization and tetramethylrhodamine (TRITC) for visualization of glycocalyx according to the manufacturer guidelines (Invitrogen Molecular Probes®, Carlsbad, CA). After staining, the samples were brought to the WVU Microscope Imaging Facility and, using a Zeiss LSM510 microscope, viewed; and a series of photos were captured at different focal lengths through the biofilm sample. Using the LSM Image Browser, these photographs were brought together for a complete focal view of the biofilm. These images were looked at to determine the biofilm stage (I–IV) according to our previous research [16] (Table 1).
Quantification of stained biofilm
Utilizing the MIF Zeiss Axiovert 40 CFL Microscope and NIH ImageJ software, the stained sample was used to acquire an image of the biofilm to be used for quantification. An image was captured and analyzed for total area of the middle (1.29 × 0.97 mcm) mcm2 of the absolute center of the 3-mm punch. Both numerical and visual data were collected.
Results
In the control group, the average age was 51.9 y and in the endOclear® group 61.3 y. The average weight of patients in the endOclear® group was 90.3 kg, whereas in the control group, it was 89.9 kg. Both groups had nine patients who were smokers (Table 2).
None of the differences is statistically significant.
Respiratory data were analyzed for patients treated with the endOclear® device both before and after treatment. A total of 43 treatments were provided to the 20 patients in that group. Tidal volumes increased by a mean of 29.9 ± 62 (standard deviation [SD]; range −150 to +198). Peak inspiratory pressures decreased by a mean of 0.39 ± 1.8 cm H2O (range −9 to +3 H2O). Resistance was found to decrease a mean of 1.67 ± 4.3 cm H2O (range −17 to +3 H2O). Accretion volumes were classified as greater than or less than 1 cc, and 24 of the treatments resulted in >1 cc of accretion removal.
T-tests were used to compare groups. The mean hours intubated for the control group was 135, with a range of 3 to 346. Within the endOclear® group, the mean hours intubated was 138, with a range from 59 to 229. This difference was not statistically significant (p = 0.91). There was no significant difference in ICU length of stay (endOclear® 9.9 d and control 11.85 d; p = 0.55).
Eleven pneumonias were diagnosed in the endOclear® group and six in the control group, but this difference was not statistically significant (p = 0.36). Analysis comparing biofilm stage and diagnosis of pneumonia showed no correlation (p = 0.13). Analysis comparing hours of intubation and development of pneumonia also found no correlation (p = 0.28). Pneumonia patients did not have a significantly greater biofilm mass area, 29.6% vs. 36.7% (p = 0.38).
All ETTs had biofilm, and the stage was determined for all. The totals by stage were Stage I 6, Stage II 17, Stage III 13, and Stage IV 4 (Table 3) One-way analysis of variance (ANOVA) between hours of intubation and biofilm stage showed no significant difference when all ETT were considered (p = 0.34). Subgroup analysis of the endOclear® group demonstrated a correlation between hours of intubation and biofilm stage, with a higher incidence of stage 3 vs. stage 1 (p = 0.005) and stage 2 vs. stage 1 (p = 0.035) when hours of intubation increased. The control group did not show any correlation between hours of intubation and biofilm stage (p = 0.702), although this comparison did appear to be underpowered.
Among all ETTs, the most common biofilm organisms were Candida (10), Enterococcus spp. (10), Staphylococcus aureus (9), and coagulase-negative staphylococci (4). The most common culture results from bronchoalveolar lavage fluid (BAL) were Candida (10), staphylococcal spp. (5), Streptococcus spp. (5), and Enterococcus (5). Only nine of the 40 patients had congruence between the microbiota of the biofilm and that of the BAL, a divergence rate of 78%.
Biofilm mass analysis was performed on the basis of the predominant species found in the biofilm. Candida was most common; the biofilm in these patients covered a mean of 32.47% of the standardized sample surface. Staphylococcus aureus was second, with a mean biofilm area of 29.15%. Enterococcus was third, with a mean area of 28.2%. When ANOVA was performed for the six most common species, no difference between species and percent area covered was found (p = 0.44). The ANOVA comparing hours of intubation for the same six organisms found no difference (p = 0.98) for percent area covered. There also was no correlation between percent area covered and stage of biofilm (p = 0.45) (Table 4).
Discussion
New technologies are emerging daily to aid in the care of the critically ill [19–22]. In today's healthcare environment, issues such as pneumonia, particularly ventilator-associated pneumonia (VAP), are of interest because of the significant costs and patient morbidities associated with the development of VAP [23,24]. Physicians and administrators alike are searching constantly for novel ways to reduce the time a patient is on mechanical ventilation and the length of stay, particularly ICU length of stay. Given these forces, new technologies may be implemented without defined efficacy. It is commonly known that standard suctioning is ineffective in the removal of accretions and biofilm that line the inside of ETTs. Accretions increase airway resistance and, potentially, the patient's work of breathing. Biofilms form on the ETT, and biofilm stage is associated with the development of pneumonia. Therefore, removal of accretions and biofilm from the ETT may decrease the time of mechanical ventilation and the rate of pneumonia. There are several commercial devices that are designed to remove these accretions. The ability of these devices to remove biofilms is not as well defined. More importantly, the efficacy of these devices in impacting the clinical problems of time on ventilation and decreasing pneumonia rates has yet to be defined.
Knowledge of the characteristics and lifecycle of biofilms is necessary to understand the lack of response to antibiotics contained therein and the ability of biofilms to be the source of clinical infections. Biofilms are a community of bacteria that attach themselves to their base by excreting a sticky EPS that encases them [12]. By doing this, they can develop a complex three-dimensional, resilient, and attached material that protects them from washing away or being eradicated by antibiotics [25]. There is a definite cycle of development and death of a biofilm, and four developmental stages have been identified (see Table 1). These growth cycles incorporate the universal principles of microbial growth. The practice of antibiotic use in a diseased patient appears to help remove underlying infection initially; however, if the infection is associated with a biofilm, antibiotic failure is inevitable, regardless of reported antibiotic sensitivity information and appropriate antimicrobial choice. The reason for this failure is that only the bacteria exposed to the antibiotic can be killed, namely free-floating, planktonic bacteria. However, bacteria encased in a mature biofilm are not exposed to the antibiotic and thus are protected from it. Only bacteria in a Stage 1 biofilm are not yet covered by glycocalyx and thus may be exposed to antibiotic.
Other pathologies that involve biofilms often require technics such as mechanical debridement or sonication. The mechanical removal of biofilm from indwelling medical devices may be an option. The endOclear® System offers a new option for removing mucus and secretions from ETTs. The manufacturers state that use of the device decreases biofilm on ETTs and therefore can reduce ventilator days and decrease the risk of pneumonia in the mechanically ventilated patient (visit www.endOclearinc.com for details).
In this study, the standard daily use of the endOclear® device resulted in only minute, clinically non-significant increases in tidal volume and decreases in peak inspiratory pressure and airway resistance. There was no statistical difference between these ventilator measures before and after device use, even though the device did demonstrate an ability to remove accretions from the ETT during use. Given the lack of a significant change in these clinical measures, claims that the device reduces the work of patient breathing cannot be supported at this time.
The secondary aim of this study was to evaluate any clinical differences between patients in whom the endOclear device was used routinely and those in whom the device was never used. Although this was a convenience sampling based on consecutive patients, the groups were well matched in demographics, including smoking status (see Table 2). The mean hours of mechanical ventilation were almost equal in the two groups. The endOclear® group had almost double the number of pneumonias (11 vs. 6); however, this difference did not achieve statistical significance. Given these results, the claim that use of this device can decrease time on the ventilator and the pneumonia rate cannot be supported.
The third aim of this study was to describe the characteristics of the biofilms that remained in the ETTs after treatment with the endOclear®. Biofilms develop on the interior of an ETT within a very short time after intubation and establishment of mechanical ventilation. According to published data, there is no correlation between the duration of intubation and the stage of a biofilm. Indeed, advanced biofilms have been demonstrated in as little as three hours after intubation [15,16]. This suggests that biofilm formation and maturation is related to patient factors rather than to the ETT. Additionally, the distribution of the stage of a biofilm compared with duration of intubation is random [26]. However, the stage of an ETT biofilm was a significant indicator of the likelihood of the development of pneumonia. In particular, stage IV biofilms were associated routinely with pneumonia in the intubated patient. In this study, biofilm was present on all ETTs, and the distribution of stages was no different in the two groups, being primarily stage II and III in both groups. Consistent with previous studies, the stage of biofilm was variable with respect to duration of mechanical ventilation.
To estimate the amount of ETT that was covered by biofilm, a standard sample was obtained, and biofilm surface area was calculated. This sample was harvested from a standardized location in the tube that has been reproducible in having the maximum biofilm formation. Although no statistical differences were found, there was a trend toward smaller surface area coverage by stage I and stage IV biofilms in the group treated with the endOclear device. Figure 2 depicts the distribution of biofilm surface area coverage by stage of biofilm in both the control and the endOclear use groups. Understanding the differences in the characteristics of biofilm stages makes this easily comprehensible and supports the idea that the device was appropriately used and may be able to remove some biofilm. In stage I, the bacteria are loosely adherent, and the glycocalyx is just beginning to form and does not yet cover all the bacteria. This loose adhesion and lack of mature glycocalyx makes this stage of biofilm more amenable to removal with gentle scraping or friction. In stage IV biofilm, the glycocalyx is brittle and dehydrated. As part of the lifecycle, parts of the biofilm will break off spontaneously secondary to this brittle, fragile state and embolize to other locations. This allows propagation of the biofilm to a new area. This brittleness and fragmentation of the glycocalyx also makes this stage amenable to removal of the topical, exposed surface. In stage II and III, on the other hand, the glycocalyx is mature and robust, making removal more difficult. Given these factors and the surface area data, the endOclear device may help reduce coverage of the ETT by some stages of biofilm, but others will remain despite treatment with the device.
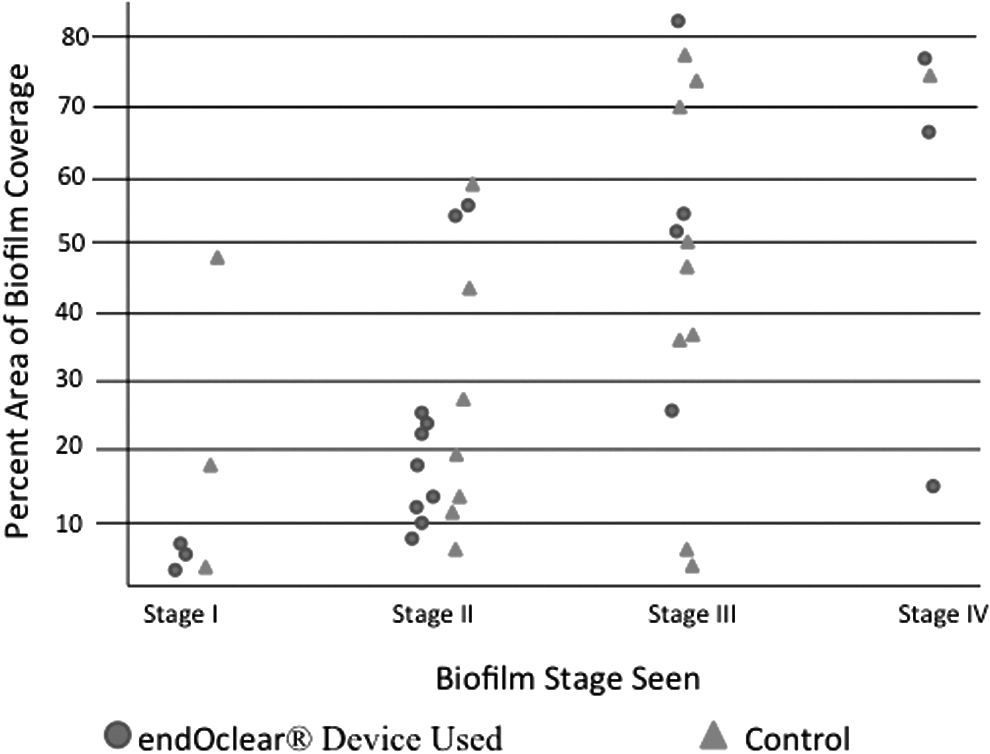
Area of biofilm coverage according to stage.
Evaluation of the microbiota of the biofilms in the ETT revealed that Candida and Enterococcus were the most prevalent organisms, with S. aureus the third most common. When evaluating the BAL samples, Candida was the most prevalent. The biofilm and BAL were 78% divergent in the most common bacteria. This large difference in culture data is a result of the glycocalyx covering the biofilm. Traditional culturing techniques sample the planktonic bacteria at the top of the biofilm almost exclusively. These free-floating bacteria above the biofilm are only a fractional portion of the organisms present. This leaves a large portion of the microbiota of the biofilm to be undersampled and understudied. Only by the mechanical breakdown by a sonicating bath can the full bacterial burden be analyzed. Previous work using microarray analysis identified a mean of 16 bacterial species within the biofilm of ETTs [27]. These data support the concept that the ETT biofilm is a unique environment and that the relation with pneumonia is complex and still poorly understood.
Any methods that help decrease the length of time a patient is on mechanical ventilation, and possibly even reducing the risk of pneumonia, are worth evaluating. Some devices showed promise in concept. In this study, we evaluated the clinical results of systematic use of one of these new devices. As these devices are disposable and single use, there is a cost to utilizing this technology. However, if the desired results are achieved, the cost may be warranted. Unfortunately, in our study, the time on mechanical ventilation was not reduced. Even more importantly, there was almost double the number of pneumonias in the device group. The reasons for this may be that the device is able to break up part of stage IV biofilms, which then may embolize bacteria to the distal airways. This can be hypothesized but was not proved by this study.
There are several limitations to this study. The numbers of patients in both arms were small. Several of the variables therefore may have been underpowered, and a larger study may show differences in surface area coverage or the incidence of pneumonia. This study involved both medical and surgical patients, which adds to the heterogeneity of the population. Lastly, this group of patients was intubated on average for a relatively short time, an average of 135 h. According to these data, the effect of the endOclear device in patients intubated for long periods of time cannot be evaluated fully. The potential role of this device in that population remains unclear.
Conclusions
Biofilms are present in ETTs and differ by stage in a way that is not related to the duration of intubation. Attempts to decrease biofilms on ETT with a scraper or shaver type of device may be possible, particularly in the vulnerable stages (stages I and IV), but mature biofilms (stages II and III) remain difficult to remove. New devices in critical care continue to evolve, but further study with large populations is required to confirm the efficacy of this device fully. On the basis of the data from this trial, further investigation is needed prior to widespread adoption of the endOclear device.
Acknowledgment
This manuscript was presented as a poster at the 28th Annual Meeting of the Eastern Association for the Surgery of Trauma, January 13–17, 2015, Lake Buena Vista, FL.
Author Disclosure Statement
The authors have no relevant financial disclosures or conflicts of interest to report.