
Abstract
Abstract
Background:
For any anti-adhesive barrier developed for abdominal surgery, the use under conditions in which anastomotic healing is compromised needs to be investigated. The current study evaluates the effect of a new ultrapure alginate gel on early healing of high-risk anastomoses in the ileum and compares this with the gold standard used in clinical practice.
Materials and Methods:
In 75 adult male Wistar rats, a 5 mm ileal segment was resected and continuity was restored by construction of an inverted anastomosis. Rats were divided randomly into a control group and groups receiving either alginate gel or a sodium hyaluronate carboxymethylcellulose (HA/CMC) film around the anastomosis (n = 25 each). Carprofen, given in a daily dose of 1.25 mg/kg, was used to compromise anastomotic healing. At day three, animals were killed and scored for signs of anastomotic leakage and the presence of adhesions.
Results:
The incidence of adhesion formation was 95% in the HA/CMC film group, which was significantly higher than in the controls (64%, p = 0.010) and the alginate gel group (52%, p = 0.004). The adhesion score was nearly 40% lower in the alginate gel group compared with the HA/CMC film group. The incidence of ileal leakage in the HA/CMC film group (92%) was significantly higher than in the controls (68%, p = 0.016). Leakage rate did not differ between the alginate gel and control groups. There was no significant difference between groups in either incision bursting pressure or incision breaking strength.
Conclusion:
Ultrapure alginate gel does not interfere with repair of ileal anastomoses constructed under conditions in which chances of anastomotic dehiscence are high. The alginate gel performs better than the HA/CMC film.
I
Separating the injured tissue surfaces using anti-adhesive barriers seems to be the best way to prevent adhesion formation and subsequent complications [5,6]. At present, of the few compounds used in abdominal operations, only one product consisting of sodium hyaluronate carboxymethylcellulose (HA/CMC) has been shown to reduce the incidence of post-operative adhesion formation [7,8]. Sodium hyaluronate carboxymethylcellulose has several drawbacks: it is brittle and sticky, making handling during open surgery difficult; it is not designed for laparoscopic surgery; and its routine use is expensive [7,9]. In addition, the anti-adhesive effect of HA/CMC membrane seems to compromise anastomotic healing as reflected by an increased incidence of leakage and related abdominal abscess and fistula formation [10–14]. From the results of a clinical study it was hypothesized that HA/CMC membrane, wrapped around an anastomosis, turned a sub-clinical leak into an overt leak by reduction of peri-anastomotic adhesions [12,15].
Recently we showed excellent anti-adhesive effects of a new ultrapure, easy to apply, alginate gel in a cecal abrasion and peritoneal sidewall excision rat model [16]. To use the gel safely in visceral surgery it is mandatory to demonstrate that it does not interfere with anastomotic healing under various conditions. As a first step, we showed recently that the gel reduces adhesion formation in a rat model of uncompromised anastomotic healing of the colon, without interfering with anastomotic repair [17]; as a second step, it should be demonstrated that the gel can be applied safely under conditions in which anastomotic repair is compromised and chances for dehiscence are high. Such conditions are present inhibitors of cyclo-oxygenase-2 (COX-2) are administered to rats before and after construction of an ileal anastomosis [18,19]. It is of particular clinical interest to ascertain that in such conditions, in which adhesion formation protecting the suture line might be more important than in normal healing, alginate gel can be used without negative effects on incision repair.
The present study investigates the effect of ultrapure alginate gel, in comparison to HA/CMC membrane, on anastomotic healing and early adhesion formation in rats that are treated with a COX-2 inhibitor, leading to high rates of anastomotic dehiscence.
Materials and Methods
Animals and experimental design
Seventy-five male Wistar rats (Charles River, Sulzfeld, Germany) were used in the experiment. Rats weighed between 240 and 280 g and were housed in filter-topped cages (two per cage) under clean, non-sterile, standardized conditions for at least five days prior to the experiment. Animals were checked daily and had free access to water and standard rodent chow (Ssniff R/M-H, Bio Services BV, Uden, The Netherlands) during the entire experimental period.
All animals underwent resection and anastomosis of the distal ileum. The rats were allocated randomly to one of three groups (n = 25 each). Animals in the first group received no further treatment and served as controls. Animals in the second group received ultrapure alginate gel and animals in the third group received HA/CMC film. All animals were euthanized on post-operative day three for analysis of anastomotic wound strength (n = 23), early adhesion formation (n = 25), and descriptive histology (n = 2). The study protocol was approved by the Animal Ethics Review Committee and performed in the Good Laboratory Practices (GLP)-certified animal research laboratory of the Radboud University Medical Center, Nijmegen, The Netherlands. Prior to the experiment, humane end points were defined to avoid unnecessary suffering of animals during the study period.
Operative procedure
Each animal was prepared for surgery by shaving and cleaning the lower abdomen with 70% alcohol. For analgesia, rats were given buprenorphine (Temgesic, Schering-Plough, Houten, The Netherlands), 0.02 mg/kg subcutaneously 30 min before surgery and the same dose every 12 h for the next two days. In addition, rats received carprofen (Rimadyl, Pfizer Animal Health, Capelle aan de Ijssel, The Netherlands) 1.25 mg/kg subcutaneously on days 0, 1, and 2 in order to create conditions that favor anastomotic leakage [18,19]. Carprofen is an analgesic that is widely used in veterinary medicine that inhibits COX activity with selectivity for COX-2 [20,21].
The rats were anesthetized by inhalation of a mixture of isoflurane (3%) and 1:1 oxygen-pressurized air. Surgical procedures were performed using a Zeiss operation microscope (Carl Zeiss AG, Oberkochen, Germany). During the operation and shortly thereafter rats were placed on a warm plate to avoid hypothermia.
All rats underwent a mid-line laparotomy and a 0.5 cm segment of the ileum was resected, 15 cm proximal to the cecum. Ileal continuity was restored by an inverted single-layer end-to-end anastomosis with eight interrupted sutures of 8-0 monofilament material (Ethicon, Norderstedt, Germany). Controls received no further treatment. In the second group animals received 1 mL of ultrapure alginate gel (Rebasol™, EMCM, Nijmegen, The Netherlands) around the anastomosis. In the third group a 10 × 30 mm sheet of HA/CMC bioresorbable film (Seprafilm®, Genzyme, A Sanofi Company, Cambridge, MA) was wrapped around the anastomosis. The abdomen was closed in two layers using Vicryl™ 3-0 suture (Ethicon, Norderstedt, Germany) for the fascia/muscle layer and incision staples for the skin. Animals were resuscitated immediately after abdominal closure with 10 mL isotonic sodium chloride (0.9%) solution administered subcutaneously.
Early adhesion formation
Animals were euthanized by carbon dioxide asphyxiation on post-operative day three. The abdomen was re-opened and inspected for adhesion formation by a blinded experienced observer (R.L.). Adhesions were scored by an investigator who was blinded to the group assignment, using Zuhlke grading system [22]. Adhesions were classified macroscopically as 0 = no adhesions; 1 = filmy adhesions: easy to separate by blunt dissection, no vascularization; 2 = mild adhesions: blunt dissection possible but partly sharp dissection required; 3 = strong adhesions: lysis possible by sharp dissection only, clear vascularization; 4 = very strong adhesions: lysis possible by sharp dissection only (organ strongly attached with severe adhesion). The organs and structures involved in the adhesion formation with the anastomosis were also noted.
Anastomotic leakage
The abdomen was inspected for signs of anastomotic leakage defined as presence of fecal peritonitis, macroscopic dehiscence, and gap in the anastomotic line with or without an abscess near it [18]; an abscess was defined as any walled off collection containing pus.
Bursting pressure and breaking strength
Ileum segments, approximately 4 cm in length containing the anastomosis were resected and adhesions were dissected carefully without affecting the anastomosis. After removal of intra-luminal fecal material, the segments were attached to an infusion pump and a device recording the internal pressure for measuring the bursting pressure representing the capability of the suture line to withstand intra-luminal force. Pressure was increased by constant infusing (2 mL/min) of water containing methylene blue into the segment, which was kept under water. The maximum pressure (mm Hg) recorded immediately before the sudden loss of pressure was taken as the bursting pressure. The site of perforation (within or outside the anastomotic line) was indicated by the loss of methylene blue.
After determining the bursting pressure, the breaking strength representing the capability of the suture line to withstand the longitudinal forces, was measured in the same segment [23]. The segment was clamped in a tensiometer (AIKOH model [9500 series], Aikoh Engineering Co. Ltd., Higashi-Osaka, Japan) that exerts a steadily increasing force in longitudinal direction. The peak force required for tearing the segment apart was recorded as the breaking strength (g).
Histologic analysis
Intestinal samples (two from each group) of approximately 1 cm, containing the entire anastomosis in the middle, were collected, opened at the mesenteric side, washed gently with 0.9% sodium chloride, and spread out in a cassette for paraffin embedding. From paraffin-embedded tissue, 4 mcm sections were prepared and stained with hematoxylin and eosin (H&E). Sections were analyzed using a binocular light microscope.
Statistical analysis
Historical data from our group show that ileal anastomotic strength in rats treated with carprofen can vary substantially. A representative value for anastomotic bursting pressure at day three is 64.5 ± 27.5 (standard deviatoin [SD]) mm Hg. Sample size for the current experiment was determined as being sufficient to detect a change of strength of 50% in experimental group at day three. Using an α of 0.05, a power of 0.8, and a two-tail test the group size is calculated (G*Power 3.1.2) to be 23. Two rats were added to each group for descriptive histology. Differences between the incidence of adhesion formation and ileal leakage in the various groups were analysed by a (one-tailed) χ2 test. Statistical analysis of continuous parameters was performed using a one-tailed Mann-Whitney U test. A Bonferonni correction was applied in case of multiple comparisons. A p value less than 0.05 was considered significant.
Results
Clinical observation and mortality
All animals survived the surgical procedure. Three animals died prematurely in the HA/CMC film group from dehiscence of the ileal anastomosis and fecal peritonitis (Fig. 1). No animal died in the control and alginate gel group. All animals experienced weight loss after operation up to the day of sacrifice, losing approximately 9% of their pre-operative weight (Fig. 2). The relative body weight was similar in the three groups at any time point.
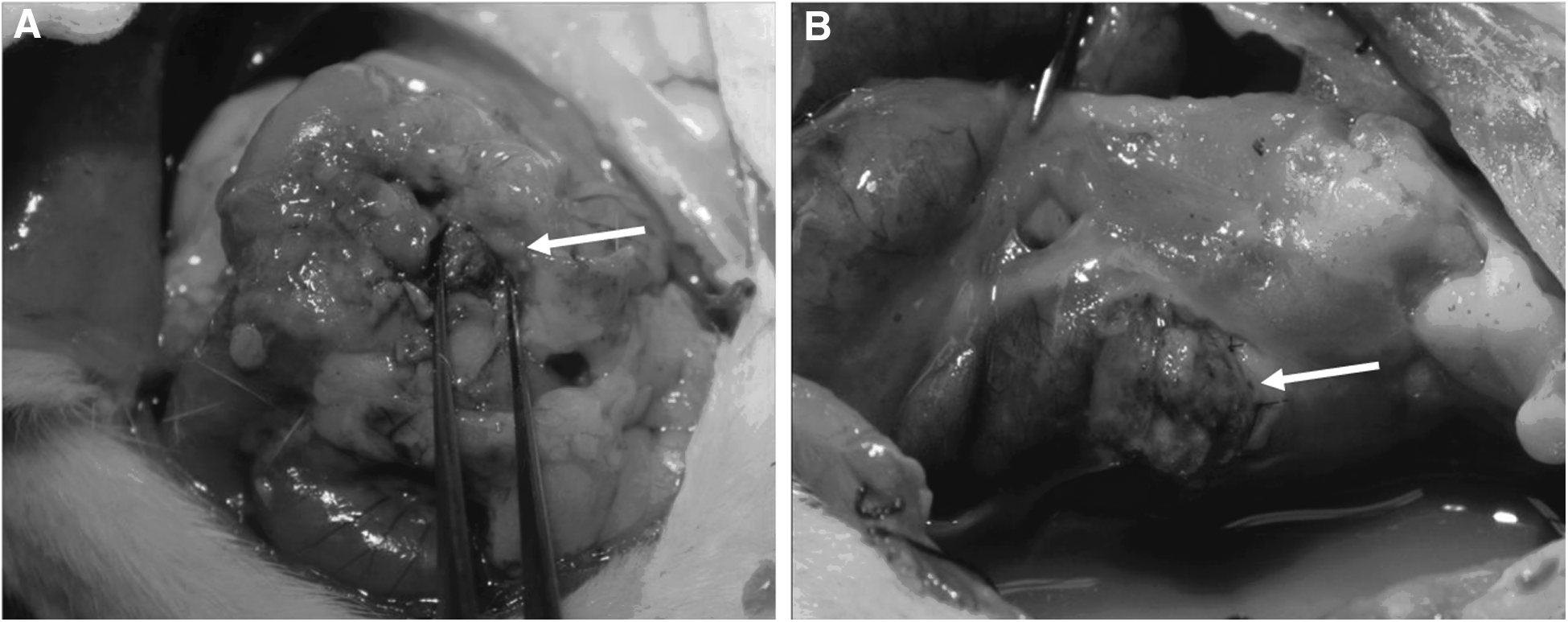
Macroscopic aspects of anastomotic leakage. (

Post-operative course of body weight. Data represent average relative body weight, in relation to the weight prior to operation.
Incidence of adhesions and ileal leakage
No significant difference in the incidence of adhesion formation was observed between rats treated with alginate gel (13/25) and the controls (16/25; p = 0.195). In the HA/CMC film group the incidence of adhesion formation (21/22) was significantly higher than in both the control (p = 0.010) and alginate gel (p = 0.004) groups (Table 1). The adhesion score was significantly lower in the alginate gel compared with the HA/CMC film group (p = 0.010; Table 1)
p = 0.010 vs. the HA/CMC film group (Mann-Whitney U test).
For adhesion parameters the three premature deaths were left out, leaving n = 22 for the calculation of adhesion incidence and score.
p = 0.010 vs. controls and p = 0.004 vs. the alginate gel group (χ2 test).
p = 0.016 vs. controls (χ2 test).
HA/CMC = sodium hyaluronate carboxymethylcellulose.
The type of structure adhered to the anastomotic site was also scored (Table 2) and a significant difference was observed between the alginate gel and HA/CMC film groups regarding adhesions between the anastomosis and fat pad (p = 0.002). The incidence of ileal leakage in surviving rats was 68% (17/25) in control rats compared with 72% (18/25) in the alginate gel group and 91% (20/22) in the HA/CMC film group. Including the three rats that died prematurely from anastomotic leakage treated with HA/CMC film (23/25; 92%), ileal leakage was higher in the film group compared with controls (p = 0.016).
p = 0.002 vs. the alginate gel group (χ2 test).
Numbers denote the number of animals with adhesions present between the structures indicated.
Anastomotic strength and histology
In all groups both the anastomotic bursting pressure (Fig. 3A) and breaking strength (Fig. 3B) were comparable. The bursting sites were always within the suture line, and when analyzing the breaking strength, tearing of the tissue invariably occurred within the anastomotic area. Treatment with either alginate gel or HA/CMC film did not significantly affect anastomotic strength at day three.
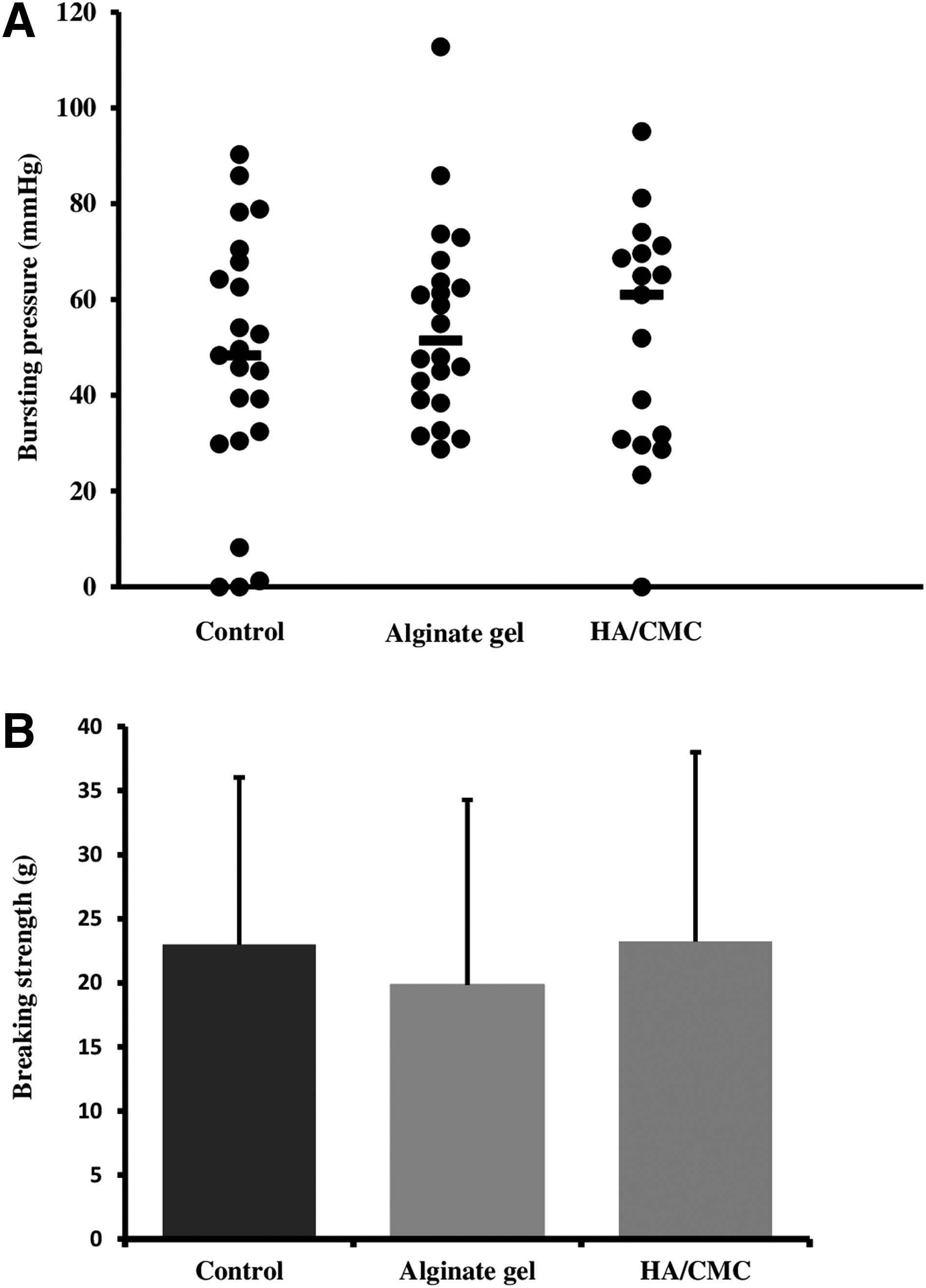
(
Discussion
The current study demonstrates that ultrapure alginate gel does not impair healing if anastomoses in the ileum are constructed under conditions that favor high leakage rates. In this respect the alginate gel tended to be safer than a HA/CMC membrane, which increased leakage to more than 90%.
Abdomino-pelvic surgical procedures, which often include construction of a bowel anastomosis, cause adhesion formation with major related morbidity, e.g., small bowel obstruction, enterotomy at adhesiolysis and secondary infertility [2]. Mechanical separation of injured peritoneal surfaces by means of adhesion barriers reduces adhesion formation in colorectal surgery. However, a large clinical trial in benign colorectal surgery indicated that the barrier HA/CMC increased the clinically overt anastomotic leak rate when wrapped around the anastomosis [12,13,24–26]. The high morbidity and 10%–20% mortality rate associated with anastomotic leakage [27] increased reluctance to use adhesion barriers in colorectal surgery with surgeons preferring seemingly to accept the morbidity and mortality associated with adhesion formation. Compared with HA/CMC, the ultrapure alginate gel holds more promise regarding the balance between pros and cons of an adhesion barrier, by reducing adhesion extent and severity, and not increasing leakage rates. Previously, we demonstrated more pronounced anti-adhesive effects in a model of normal anastomotic healing in the colon, indicating better barrier function when inflammation is limited [17].
Some previous rodent studies on HA/CMC membrane wrapped around or applied in the proximity of an anastomosis failed to show a negative effect on healing [24,28]. Models used in these studies were either intact uncompromised anastomoses or anastomoses with a deliberate defect created during their construction, mainly by using an insufficient number of sutures. In the current study, we deliberately tested the effect of the new anti-adhesive ultrapure alginate gel in a model of spontaneous leakage, which represents dehiscence of a patent anastomosis with time and is of more clinical interest for determining safety of the barrier in visceral surgery than previous models. In this spontaneous leak model, HA/CMC membrane wrapped around the ileal anastomosis led to an increased incidence of anastomotic leakage without exhibiting any anti-adhesive effect at all. The absence of an anti-adhesive effect of the HA/CMC membrane was possibly because of an increased inflammatory response associated with leakage, although this was not apparent from histology results. The supposed anti-inflammatory and anti-bacterial effects of the alginate gel may have prevented further healing disturbances of the anastomosis and adhesion development [29,30]. Another explanation is that HA/CMC membrane initially performed better than the gel preventing normal tissue response sealing the anastomotic leak with an overt leak and severe inflammation of the surrounding area, followed by secondary adhesion formation as a result. Although both barriers were applied around the anastomosis, alginate gel might have had a lower concentration in comparison to the HA/CMC membrane shortly after operation because of quick dilution of the active compound and exerting less detrimental effects on anastomotic healing. Altogether, the model might have been challenging to demonstrate adhesion prevention in a largely inflamed area because of anastomotic healing disturbances.
The COX-2 inhibitor carprofen was used in this model because it is a common peri-operative painkiller in rodents with known pharmacokinetics and dynamics [18,20]. Similar spontaneous leak results were obtained in control animals when using diclofenac, a painkiller used commonly in colorectal surgery [31]. The finding of low mechanical anastomotic strength without differences between groups is probably because of the overwhelming disturbance of healing in this model as reflected by leak rates above 70% in all three groups.
Alginate gel does not further aggravate the impairment of wound repair in anastomoses constructed under compromised conditions in the rat ileum, seemingly in contrast to the HA/CMC membrane that currently represents the gold standard for anti-adhesion prevention in open visceral surgery. This result supports the suitability of alginate gel to be used for adhesion prevention in surgery of the alimentary tract (Fig. 4).
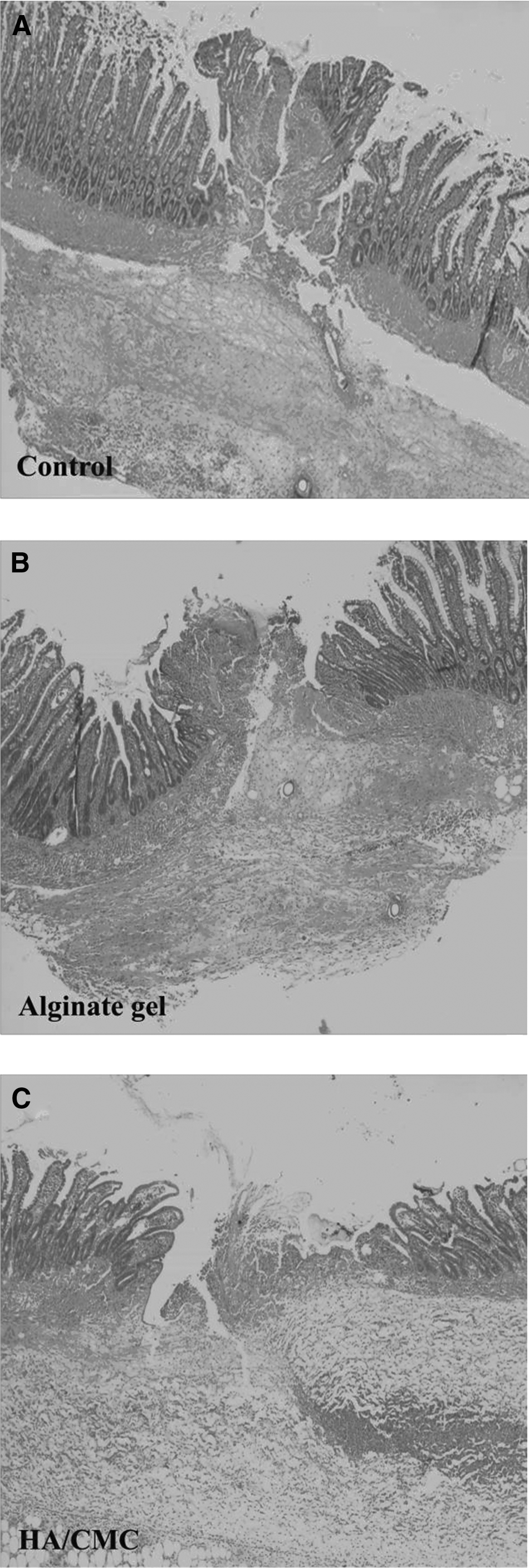
Anastomotic histology. Each panel shows a tissue segment with the anastomosis in the middle at a magnification of approximately 40 × , representing a typical example obtained at day three from (
Footnotes
Acknowledgments
The work was presented at the 26th European Congress on Surgical Infection, May 9–11, 2013, Prague, Czech Republic.
The research leading to these results has received funding from the European Community's Seventh Framework Programme; MultiTERM, grant agreement number 238551.
Author Disclosure Statement
No competing financial interests exist.