
Abstract
Abstract
Background:
Despite the excellent negative predictive value of sterile respiratory cultures, antibiotics often are continued after negative endotracheal aspirate (ETA) or bronchoalveolar lavage (BAL) for critically ill trauma patients. We hypothesized that persistent elevation of the Clinical Pulmonary Infection Score (CPIS) would predict continued antibiotic therapy after a negative respiratory culture for intubated trauma patients, and that prolonged antibiotics would provide no benefit.
Methods:
We performed a four-year retrospective cohort analysis (May 1, 2011–September 30, 2015), including patients from our trauma database with ETA or BAL, excluding patients with any infection other than pneumonia or bacteremia. Cultures with <2+ organisms on gram stain and <2+ or 104 organisms on culture were considered negative. The CPIS was assessed at the time of culture and five days later, when all cultures were final. Multiple logistic regression was used to identify predictors of long-term antibiotic therapy.
Results:
A series of 106 patients with negative cultures were included, of whom 61 had ≤5 d of antibiotics and 45 had >5 d of antibiotics. There were no differences in injury severity, head or chest trauma, initial CPIS, or subsequent culture results between the groups. Long-term antibiotic therapy did not affect intensive care unit (ICU) length of stay (LOS), ventilator days, hospital LOS, or death. Factors predicting long-term antibiotic therapy included development of a localized chest radiograph infiltrate (odds ratio [OR] 6.8; 95% confidence interval [CI] 1.7–28), CPIS >5 five days after culture (OR 6.1; 95% CI 1.2–32), and a colonized culture (OR 3.3; 95% CI 1.3–8.3).
Conclusions:
Long-term antibiotic therapy for intubated trauma patients with negative respiratory cultures provided no benefit and was predicted by development of a localized chest radiograph infiltrate, persistently elevated CPIS, and a contaminated/colonized culture. Although long-term antibiotic use did not worsen outcomes, better strategies are needed to diagnose pneumonia accurately and ensure timely discontinuation of antibiotics when appropriate.
E
The purpose of this study was to characterize antibiotic prescription patterns following negative respiratory cultures for intubated trauma patients, compare outcomes between patients whose antibiotics were discontinued after negative culture and patients who remained on antibiotics, and identify factors predicting prolonged antibiotic administration. We hypothesized that persistent elevation of the CPIS would predict continued antibiotic therapy after a negative respiratory culture for intubated trauma patients and that prolonged antibiotics would provide no benefit.
Patients and Methods
Study subjects were identified by searching our institutional trauma database for patients age 18 or greater who received at least 48 h of mechanical ventilation and had at least one of three tests while intubated: Semi-quantitative endotracheal aspirate (ETA), fiberoptic bronchoscopy and semi-quantitative bronchoalveolar lavage (SQ-BAL), or fiberoptic bronchoscopy and quantitative bronchoalveolar lavage (Q-BAL) during a four-year period ending September 2015. Institutional Review Board approval was obtained. During the study period, methods for diagnosing pneumonia in intubated trauma patients primarily consisted of Q-BAL yielding ≥104 pathogenic colony-forming units (CFU)/mL or CPIS >6 as described by Pugin et al. [10]. This study included ETA, SQ-BAL, and Q-BAL samples in order to depict a broad population of patients with negative respiratory cultures. Although BAL techniques have the theoretical advantage of sampling the lower airways, and ETA cultures have a tendency to produce false-positive results [25], ETA results were included for their strong negative predictive value [18,19] and evidence that invasive and non-invasive tests each have a role in evaluating mechanically ventilated patients for pneumonia [26]. Trauma patients managed at an outside facility for >24 h prior to admission were excluded. Trauma patients on scheduled antibiotics prior to culture and those with any infection other than pneumonia or bacteremia were excluded to ensure that antibiotic prescription patterns reflected empiric treatment of presumed pneumonia. In order to isolate the influence of clinical factors on antibiotic administration, the final study population consisted only of patients with a negative gram stain, finalized negative culture, and survival for at least six days after cultures were obtained (Fig. 1). Although previous work has shown that preliminary BAL cultures at 24–36 hours correlate well with final culture results [27, 28], the final 96-h result was evaluated in this study in order to select the group of patients with definitive evidence of airway sterility.
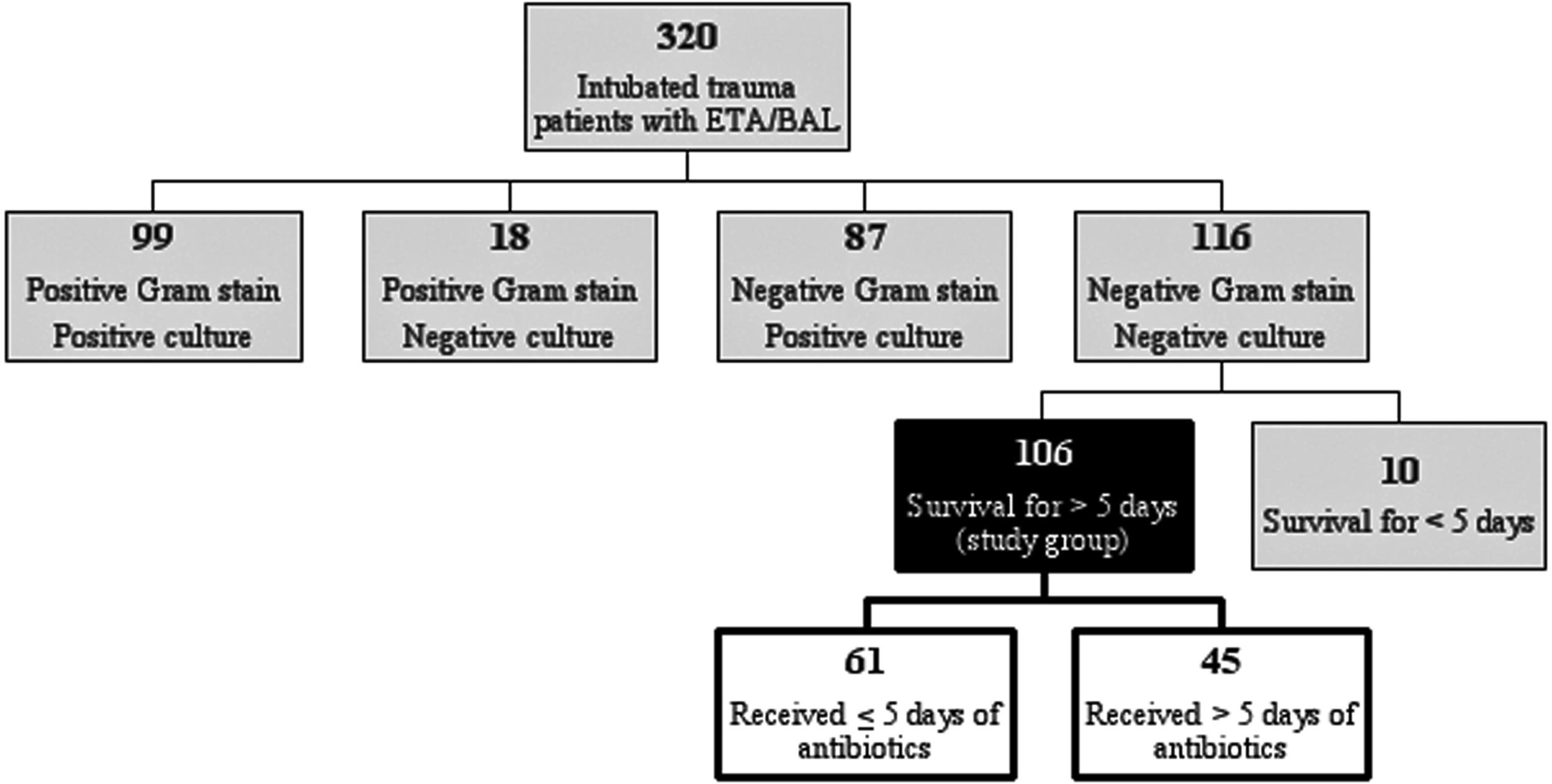
Study group selection (ETA = endotracheal aspirate, BAL = bronchoalveolar lavage).
Cultures yielding <2+ organisms on gram stain and <2+ or 104 CFU/mL on culture were considered negative. In clinical practice, a threshold of >105 CFU/mL avoids overtreatment of colonizing organism by limiting false-positive results while maintaining a low rate of false-negative results in trauma patients [29–31]. However, for the purposes of this study, the threshold of <104 CFU/mL was chosen to identify true-negative cultures accurately and ensure appropriate classification of Pseudomonas and Acinetobacter spp. [29]. Cultures containing non-floral bacteria in quantities that did not meet the diagnostic threshold for pneumonia were considered colonized rather than infected. The CPIS was calculated at the time of culture and five d later when all cultures were final, and patients were grouped by antibiotic duration ≤5 d vs. >5 d (i.e., long-term antibiotic administration).
All variables were collected by retrospective review of the electronic medical record and institutional trauma registry. Computed tomography (CT) scans at the time of admission were interpreted by a Board-certified attending radiologist. The incidence of diabetes mellitus was determined by the International Classification of Diseases, Ninth Revison, code review and medication reconciliation evidence of outpatient oral hypoglycemic or subcutaneous insulin use. Immunosuppression was defined as medication reconciliation evidence of outpatient or inpatient chemotherapy, high-dose steroids (>30 mg prednisone equivalent/d) [32], or the presence of an active disease that suppresses resistance to infection (i.e., leukemia, lymphoma, and acquired immune deficiency syndrome). Smoking status was determined by medication reconciliation evidence of outpatient or inpatient nicotine replacement therapy and by the documented social history. Blood stream infection was defined as two of four bottles positive for likely contaminants (i.e., Staphylococcus epidermidis, Propionibacterium acnes, and Corynebacterium spp.), or one of four bottles positive for other organisms. Antibiotic administration before culture was defined as any systemic antibiotic given within the 72-h window preceding culture in view of evidence that antibiotic therapy within this window may affect culture results [33]. Secretions described as both thick and discolored were considered purulent. Chest radiographs were interpreted by a Board-certified attending radiologist with no knowledge of study group assignment. Multi-drug resistance was defined as non-susceptibility to at least one agent in three or more antimicrobial categories [34].
The ETA cultures were obtained by advancing a single-use 14F suction catheter kit (Medline Industries, Mundelein, IL) 2 cm past the end of the endotracheal tube and then releasing vacuum suction without use of irrigation. Fiberoptic bronchoscopy and BAL were performed as described by the Memphis International Consensus Report [35]. Specimens were considered adequate if they had <25 epithelial cells under 10 × magnification. Semi-quantitative respiratory cultures were performed by inoculating the culture plate and then streaking the specimen into four quadrants. Semi-quantitative cultures were reported as “Few” if there were <25 colonies, “1+” if there were at least 25 colonies within the first quadrant, “2+” if colonies spread to two quadrants, “3+” if colonies spread to three quadrants, and “4+” if colonies spread to four quadrants.
A protocol for Q-BAL within 48 h of admission for intubated trauma patients with traumatic brain injury or chest trauma was instituted November 1, 2013. In order to abrogate confounding effects on the data, all protocol inclusion criteria were assessed for all patients before and after protocol initiation, and outcomes were compared across ETA, SQ-BAL, and Q-BAL specimens. A protocol for preventing ventilator-associated pneumonia (VAP) was instituted prior to the study start date. The VAP protocol bundle included daily sedation holidays, daily spontaneous breathing trials, head-of-bed elevation to 30o, routine peptic ulcer prophylaxis, daily oral hygiene with chlorhexidine, and use of the Hi-Lo Evac endotracheal tube in order to clear subglottic secretions.
Statistical analysis was performed using SPSS V. 23 (IBM, Armonk, NY) to calculate the Fisher exact test to compare categorical variables and one-way analysis of variance to compare normally distributed continuous variables. The Bonferroni correction was employed in comparing diagnostic yield, antibiotic prescription patterns, and outcomes across patients who had ETA, SQ-BAL, and Q-BAL. Clinical predictors of prolonged antibiotic therapy were identified by multiple logistic regression. Independent variables were selected based on bivariate correlation with the dependent variable and absence of significant collinearity with other independent variables. Selected independent variables were entered manually into the regression equation. Alpha was set at 0.05, confidence intervals were set at 95%, and data were reported as mean ± standard error (SE) or n (%).
Results
One third of the screened trauma patients had a negative gram stain, negative culture, and survived for at least five d after culture. These patients (N = 106) formed the study group (Fig. 1). Forty-three percent of the patients in the study group received more than 5 d of antibiotics (Fig. 2). Trauma patients who received five or more days of antibiotics and those who received more than 5 d of antibiotics were similar in terms of demographic factors, injury severity, risk factors for pneumonia, and potentially confounding factors (Table 1). The two groups also had similar individual CPIS criteria and CPIS scores at the time of culture, although colonization was more common among patients who received prolonged antibiotics (Table 2). Of the 32 patients with a colonized culture, only one was immunosuppressed, and this patient received an 8-d course of antibiotics.

Antibiotic administration after negative respiratory culture.
Data are reported as mean ± standard error or n (%).
AIS = Abbreviated Injury Score; BSI = blood stream infection; CT = computed tomography; GCS = Glasgow Coma Scale score; ISS = Injury Severity Score; WBC = white blood cell.
Data are reported as mean ± standard error or n (%).
CPIS = Clinical Pulmonary Infection Score; WBC = white blood cell.
Twenty-five percent of all patients had a second respiratory culture within 5 d, and few were positive (Table 2). Five days after initial culture, the CPIS was a full point higher among patients who received prolonged antibiotic therapy (Table 2). This group also had substantially smaller improvements in PaO2:F
Data are reported as n (%) or mean ± standard error.
ICU = intensive care unit; MDR = multi-drug resistant.
Three variables consistent with clinical concern for pneumonia were predictive of prolonged antibiotic therapy on multiple binary logistic regression (Table 4). Together, these factors formed a model that was statistically significant (χ2 (3) = 25.8; p < 0.001), explained 29% of the variability in duration of antibiotic therapy (Nagelkerke R2 0.29), and correctly classified 71% of all cases.
CPIS = Clinical Pulmonary Infection Score.
Discussion
Critically ill trauma patients commonly received antibiotics after negative respiratory cultures but did not benefit from prolonged antibiotic therapy. There also was no clear evidence of harm, although this study was underpowered to detect differences in multi-drug resistant organism isolation, and patients with Clostridium difficile infections were excluded (along with all infections other than pneumonia and bacteremia) in order to avoid confounding patterns in antibiotic administration. As expected, a persistently elevated CPIS was associated with prolonged antibiotic therapy, likely because of trends in PaO2:F
Previous work also demonstrated highly irregular antibiotic prescription patterns for critically ill patients with suspected pneumonia, particularly when clinical criteria guide management. Swoboda et al. [8] observed substantial variability in diagnosing and treating pneumonia among critically ill surgical patients when using the U.S. Centers for Disease Control and Prevention (CDC) definition of pneumonia, CPIS, or consensus by a committee of experienced clinicians. The authors reported that 50% of antibiotic days in their surgical intensive care unit (ICU) were targeting a presumed diagnosis of pneumonia that did not meet CDC or CPIS criteria [8]. Fagon et al. [36] randomized critically ill medicine patients to diagnosis by clinical criteria alone, by fiberoptic bronchoscopy with BAL, or by protected specimen brush samples and found that clinical diagnosis was associated with increased antibiotic use and a greater mortality rate than in the invasive diagnostic group. In a case-control study of intubated trauma patients, Baker et al. [37] reported that less than half of all patients with clinical suspicion of pneumonia had evidence of pneumonia on quantitative BAL. Several factors likely contribute to these findings. In trauma patients, clinical diagnosis alone is compromised by frequent colonization of the tracheobronchial tree among intubated patients [16]. Also, chest radiography has little predictive value for ventilator-associated pulmonary infection [38], clinical diagnostic criteria are subject to a large degree of inter-observer variability [14], and critically ill patients often have non-infectious instigators of the SIRS response. These factors limit the utility of the CPIS criteria in managing intubated trauma patients.
However, non-invasive and invasive microbiologic diagnostic tests are not fool-proof, and reported efficacy differs across institutions. On systematic review, quantitative BAL specimens had a mean 73% sensitivity (range 42%–93%) and 82% specificity (range 45%–100%) for diagnosing VAP compared with biopsy-proved neutrophil infiltration of alveoli in combination with clinical and microbiologic data [39]. The true value of microbiologic specimens may lie in targeting antibiotic therapy for patients who are likely to have pneumonia and allowing for discontinuation of antibiotics when cultures are negative, although some may question the negative predictive value of respiratory cultures based on the wide range of reported results and the potentially confounding influence of antibiotic administration before cultures are obtained [33, 39]. Nevertheless, targeted antibiotic therapy is clearly superior to empiric therapy, and negative endotracheal aspirates have negative predictive value ranging from 94%–100% in the absence of recent changes in antibiotic therapy [18,19]. The strong negative predictive value of the gram stain and respiratory culture may be of particular value among trauma patients, who are commonly affected by SIRS and whose chest radiographs may be difficult to interpret if there has been chest trauma [24,40].
The major limitations of this study are its retrospective design, lack of power to detect differences in multi-drug resistant organism isolation, and propensity to produce false-positive results by making multiple comparisons. However, retrospective analysis has the advantage of avoiding the Hawthorne effect, in which behavior is modified by the knowledge that performance is being observed. When more than two groups were being compared, the Bonferroni correction was employed to reduce the family-wise error rate and avoid false-positive results. In the future, appropriate antibiotic management decisions may be supported by selective utilization of procalcitonin concentrations [41] and quantitative polymerase chain reaction of bronchoalveolar lavage samples, which has the potential to provide accurate diagnostic information within hours of sampling [42]. At our institution, strict adherence to protocolized management of intubated trauma patients with suspected pneumonia may abrogate unnecessary antibiotic administration.
Conclusions
Long-term antibiotic administration for intubated trauma patients with negative respiratory cultures was common and provided no benefit. Risk factors included development of a localized chest radiograph infiltrate, persistently elevated CPIS, and contaminated/colonized cultures. However, many cases of prolonged antibiotic administration after negative cultures could not be explained by clinical or microbiologic criteria. Protocolized antibiotic management and more accurate diagnosis of pneumonia may be necessary to ensure timely discontinuation of antibiotics for intubated trauma patients with negative respiratory cultures.
Footnotes
Acknowlegment
This study was supported in part by grants P30 AG028740 (PAE, SCB) awarded by the National Institute on Aging and by R01 GM113945-01 (PAE), R01 GM105893-01A1 (AMM), P50 GM111152–01 (SCB, FAM, PAE, AMM) awarded by the National Institute of General Medical Sciences (NIGMS). TJL was supported by a post-graduate training grant (T32 GM-08721) in burns, trauma, and perioperative injury from the NIGMS.
Author Disclosure Statement
The authors have nothing to disclose.