
Abstract
Abstract
Background:
In contrast to studies evaluating the negative effect of bacterial infections on clinical outcomes after liver transplantation, there is little evidence with regard to pre-transplant bacterial infections. We aimed to investigate the impact of pre-transplant bacterial infections on post-transplant outcomes in patients after liver transplantation.
Patients and Methods:
We retrospectively analyzed clinical data from 33 consecutive patients who underwent primary liver transplantations. Patients were divided into two groups based on the occurrence of a bacterial infection within the 30 days before transplantation.
Results:
Of the 33 patients, 23 patients did not have pre-transplant bacterial infections, while 10 patients did have pre-transplant bacterial infections. Pre-transplant bacterial infections were urinary tract infections (n = 4), spontaneous bacterial peritonitis (n = 3), and one each of pneumonia, bacteremia, and cellulitis. There were no differences in clinical characteristics between the two groups. Post-operative clinical outcomes, including post-operative bacterial infection, intensive-care unit re-admission, 30-day re-hospitalization, and 90-day mortality rate were not significantly different between the two groups. The two-year overall survival rate was 76.7% in patients with pre-transplant infections and 80.0% in those without pre-transplant infections.
Conclusions:
Patients with pre-transplant bacterial infections did not have inferior clinical outcomes, compared with those without pre-transplant bacterial infections.
B
Although studies concerning the negative effect of bacterial infections after transplantation have been well-reported [3–6], there has been little analysis of pre-transplant bacterial infections. Because liver transplantation is a major surgical procedure that is often performed on critically ill patients who are highly immunosuppressed, the importance of pre-transplant infection status should be focused. This study aimed to investigate the impact of pre-transplant bacterial infections on post-transplant clinical outcomes in patients after liver transplantation.
Patients and Methods
Clinical data of consecutive adult patients who underwent primary liver transplantation from March 2009 to December 2015 were extracted from our database and reviewed. Among the 33 patients eligible for this study, 23 patients did not have pre-transplant infections, and 10 patients had pre-transplant infections.
Pre-transplant bacterial infections
In this study, pre-transplant bacterial infections were defined as bacterial infections developing within the 30 days before liver transplantation. All infections were defined according to the standard criteria proposed by the Centers for Disease Control and Prevention [7]. Diagnosis of spontaneous bacterial peritonitis (SBP) was established by a positive ascites bacterial culture or an elevated ascites absolute polymorphonuclear leukocyte count ≥250 cells/mm3 in cases of culture-negative SBP.
Species identification and antimicrobial susceptibility assessments were performed for each infection case. Once bacterial infection was diagnosed, broad-spectrum antibiotics were administered initially until identification of the causative species. Then, species-specific antimicrobial agents were prescribed.
Pre-transplant bacterial infections were regarded as managed well according to the following criteria: (1) Disappearance of clinical symptoms or signs suggestive of sepsis, and (2) normalization or improvement of laboratory and/or imaging findings [8], and/or (3) negative conversion of bacterial culture.
Pre- and post-operative treatment protocols
The standard immunosuppression regimen included tacrolimus and low-dose prednisone. Induction therapy with the interleukin-2 receptor antibody (basiliximab) was used, except for cases of identical human leukocyte antigen matching. Anti-metabolites were administered depending on patient conditions and adverse events after operation.
Intravenous third generation cephalosporin (3 g/d) and moxifloxacin (400 mg/d) were administered as a peri-operative prophylactic antimicrobial regimen and continued for 48 hours after the surgical procedure. In patients with pre-transplant infections who had not completed treatment, the previous regimen was maintained.
Statistical analysis
All statistical analysis was performed using SPSS software, version 20.0 (SPSS, Chicago, IL). For analysis of categoric variables, chi-square tests or Fisher exact tests were used. Continuous variables were analyzed using Mann-Whitney U tests. Overall survival was defined from the date of operation to the date of death or last follow-up. Survival curves were plotted using the Kaplan-Meier method, and intergroup differences were assessed by log-rank test. A p value <0.05 was considered statistically significant.
Results
The pre-transplant bacterial infections consisted of urinary tract infections (UTI) (n = 4), SBP without bacteremia (n = 3), and one case each of pneumonia, bacteremia, and cellulitis (Fig. 1.). The causative pathogens of UTI were Enterococcus species (n = 2), Klebsiella pneumoniae (n = 1), and Escherichia coli (n = 1). In patients with SBP, gram negative Acinetobacter species were confirmed in two patients, and Enterococcus faecalis was found in one patient. Unusually, Vibrio vulnificus was identified from the blood of one patient.
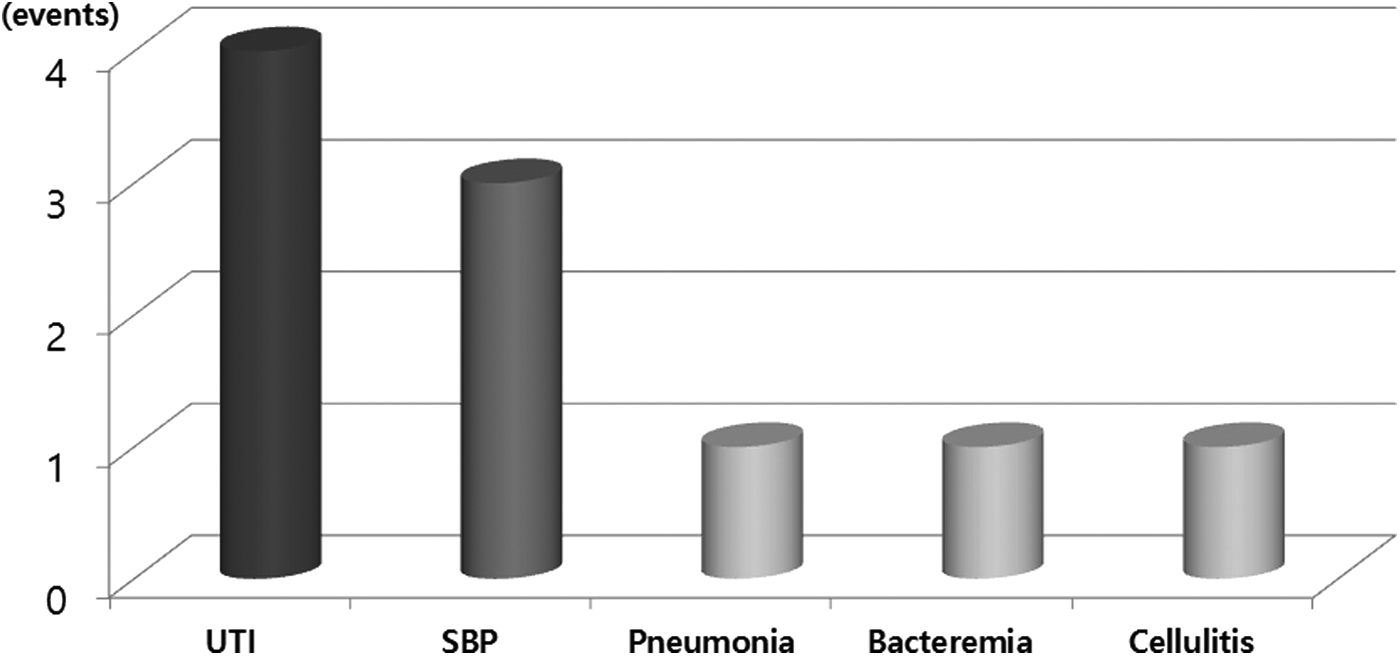
Types of pre-transplant bacterial infections. The most common pre-transplant bacterial infection was urinary tract infection (UTI), followed by spontaneous bacterial peritonitis (SBP) without bacteremia.
Comparisons of clinical characteristics between the two groups
There were no significant differences in age, gender, or etiology of liver disease between the two groups. The rate of pre-transplant hospitalization tended to be higher in patients with pre-transplant infections, but there was no statistically significant difference. Other factors, including Model for End-stage Liver Disease score and Child-Pugh score, were not different between the two groups (Table 1).
Including autoimmune hepatitis, cholestatic liver disease, or unknown origin.
Events within 30 days before liver transplantation.
ICU = intensive care unit; MELD = Model for End-stage Liver Disease.
Treatment course of each recipient with pre-transplant bacterial infections
Each recipient received various schedules of antibiotic treatment for pre-transplant bacterial infections. Only 2 recipients who had pneumonia and cellulitis could not reach complete recovery from pre-transplant bacterial infections before liver transplantation. Even though post-operative infections developed in five of 10 recipients, the sources of post-operative infections were not closely related to those of pre-transplant infections (Table 2).
F = female; UTI = urinary tract infection; PO = per os; IV = intravenous; M = male; SBP = spontaneous bacterial peritonitis.
Comparisons of clinical outcomes between the two groups
When compared with patients without pre-transplant infections, patients with pre-transplant infections did not have inferior clinical outcomes (Table 3). Intra-operative outcomes, measured by operative time and intra-operative blood loss, were not significantly different between the two groups. Other clinical events, including the rate of post-operative infection, re-admission to the ICU, and 30-day re-hospitalization, did not differ between the two groups (Fig. 2).
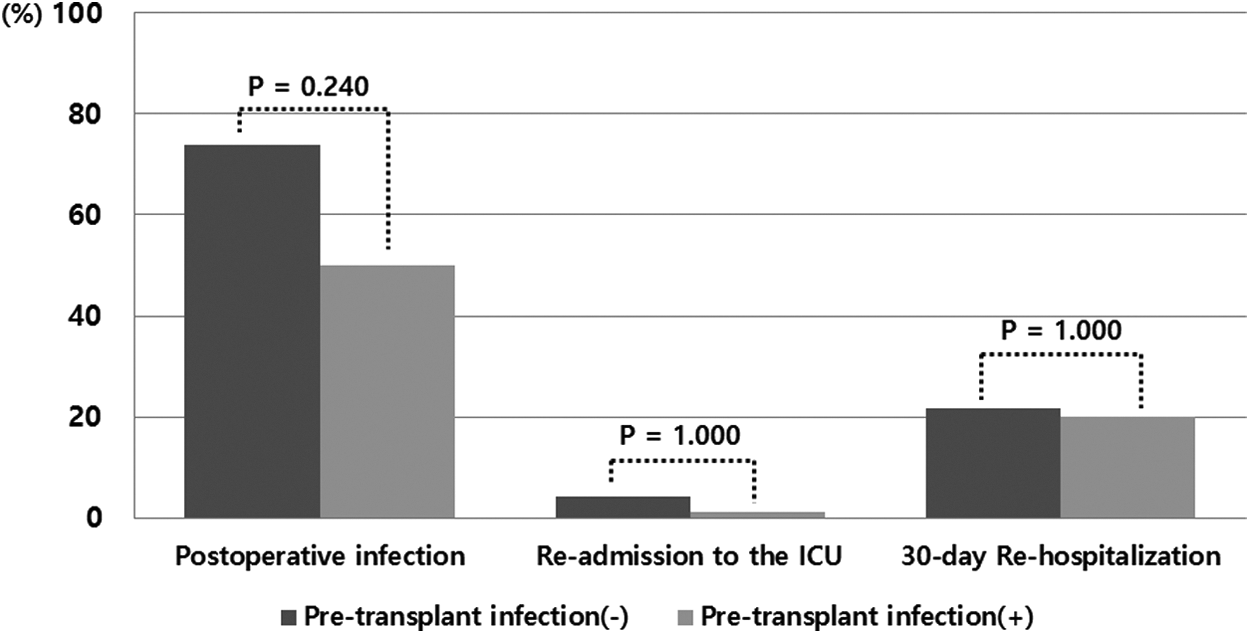
Comparison of post-operative clinical outcomes between the two groups. The post-operative clinical outcomes, including the rate of post-operative infections, re-admission to the intensive care unit (ICU), or 30-day re-hospitalization, did not differ between the two groups.
The variable allows the overlapping events.
APACHE = Acute Physiology And Chronic Health Evaluation; ICU = intensive care unit.
At day 90 post-transplantation, the overall mortality rate were 13.0% in patients without pre-transplant infections, and 20.0% in patients with pre-transplant infections (p = 0.624). When we compared two-year overall survival rates between the two groups, there was no significant difference (76.7% for patients with pre-transplant infections vs. 80.0% for patients without pre-transplant infections, p = 0.847) (Fig. 3). Among 10 patients with pre-transplant infections, two patients with pre-transplant SBPs died within 90 days after operation. Post-operative sepsis derived from pelvic hematoma developed in one recipient, and the other recipient died from post-operative bleeding.

The overall survival rates in patients with or without pre-transplant infections. The two-year overall survival was not significantly different for patients with pre-transplant infections (76.7%) compared with patients without pre-transplant infections (80.0%) (p = 0.847).
Discussion
In the current study, we found that the recipients with pre-transplant bacterial infections experienced comparable post-operative outcomes and two-year overall survival rates compared with those without pre-transplant infections.
Post-transplant bacterial infections have been studied throughout the years. Bacterial infections, with frequencies ranging 20%–80%, represent one of the most serious complications after liver transplantation. They contributed to longer hospital stays and increased hospital costs [3]. Three-fourths of post-transplant bacterial infections occur in the first month after surgery [9]. We also evaluated post-transplant infection episodes in both groups and found that most bacterial infections developed within one week of operation in both groups.
Studies examining the effects of pre-transplant bacterial infections have been limited, however. One study recently evaluated the impact of pre-transplant infections in 100 consecutive patients undergoing liver transplantation [10]. The researchers suggested that pre-transplant infections treated adequately did not pose a significant risk for poor outcomes, including post-transplant death. Other studies [8,11] performed only in patients after living-donor liver transplantation also similarly reported that pre-transplant infections did not affect post-transplant outcomes.
SBP is the most common infection in patients with cirrhosis [12]. Sun et al. [10] also found that most SBP-derived pre-transplant infections comprised the highest portion of infections (35.6% of all patients with pre-transplant infections). In our cases, the most common pre-transplant bacterial infections were UTIs, followed by SBP-related infections. This discrepancy might result from time of diagnosis for pre-transplant infections, which was defined within 12 months before transplantation in their study compared with one month before our study.
As the level of knowledge about disease processes develops, the standard indication for liver transplantation is rapidly changing [13,14]. From the perspective of effective organ allocation, it is important to assess how infections correlated with post-transplant clinical outcomes. Interestingly, in our cases, patients with pre-transplant bacterial infections had shorter median follow-up periods compared with those without infections (14 months [range 0–42 months] vs. 41 months [range 0–83 months], data not shown), which may reflect that patients with pre-transplant bacterial infections were relatively excluded as candidates for liver transplantation. With growth in experiences, the indications have been extended in more recent years in our institute.
This study has several weaknesses. Because of the nature of retrospective research, selection bias could not be eliminated completely. Our small sample size was not large enough for us to allow discrimination power. To be validated, our study should be confirmed in further independent, large cohorts. Moreover, we evaluated both deceased-donor and living-donor transplantation, which might have basic differences in graft size (whole liver vs. partial liver) and operation schedule (emergent vs. elective). Especially, operation schedule might largely influence the course of antibiotic treatment in pre-transplant periods. Six of 10 recipients with pre-transplant bacterial infections underwent liver transplantation from deceased donors in an emergency, which made some of the patients not reach complete recovery from pre-transplant infections. Nevertheless, this study showed similar results to previous studies that were performed in one of the two populations (8,11,15).
Conclusion
Our data demonstrated that patients with pre-transplant bacterial infections did not have inferior outcomes compared with those without pre-transplant bacterial infections. If proper treatment with antimicrobial therapy is offered, pre-transplant bacterial infections do not negatively affect post-operative clinical outcomes.
Footnotes
Author Disclosure Statement
No competing financial interests exist.