
Abstract
Abstract
Background:
Surgical site infections (SSI) contribute to surgical patients' morbidity and costs. Operating room traffic may be a modifiable risk factor for SSI. We investigated the impact of additional operating room personnel on the risk of superficial SSI (sSSI).
Patients and Methods:
In this matched case-control study, cases included patients in whom sSSI developed in clean surgical incisions after elective, daytime operations. Control subjects were matched by age, gender, and procedure. Operating room personnel were classified as (1) surgical scrubbed, (2) surgical non-scrubbed, or (3) anesthesia. We used conditional logistic regression to test the extent to which additional personnel overall and from each work group were associated with infection.
Results:
In total, 474 patients and 803 control subjects were identified. Each additional person among total personnel and personnel from each work group was significantly associated with greater odds of infection (all personnel, odds ratio [OR] = 1.082, 95% confidence interval [CI] 1.031–1.134, p = 0.0013; surgical scrubbed OR = 1.132, 95% CI 1.029–1.245, p = 0.0105; surgical non-scrubbed OR = 1.123, 95% CI 1.008–1.251, p = 0.0357; anesthesia OR = 1.153, 95% CI 1.031–1.290, p = 0.0127). After adjusting for operative duration, body mass index, diabetes mellitus, and vascular disease, additional personnel and sSSI were no longer associated overall or for any work groups (total personnel OR = 1.033, 95% CI 0.974–1.095, p = 0.2746; surgical scrubbed OR = 1.060, 95% CI 0.952-1.179, p = 0.2893; surgical non-scrubbed OR = 1.023 95% CI 0.907–1.154, p = 0.7129; anesthesia OR = 1.051, 95% CI 0.926–1.193, p = 0.4442).
Conclusion:
The presence of additional operating room personnel was not independently associated with increased odds of sSSI. Efforts dedicated to sSSI reduction should focus on other modifiable risk factors.
S
Personnel movement in and out of operating rooms is identified as a risk factor for SSIs in the Centers for Disease Control surgical practice SSI reduction guidelines [19–21]. These recommendations are based on investigations suggesting that human beings are vectors of bacterial transmission [19,22,23] and that the disruption of intra-operative airflow can potentially lead to an increased risk of SSI [24–26]. Operating room traffic is often associated with transitions of care and handoffs, which are believed to contribute to adverse patient outcomes [27–32], including infection [33]. It is unclear whether operating room traffic in general or the traffic of specific personnel groups impacts SSI risk [34].
We used a case-control study design to test the impact of increased operating room personnel traffic on the risk of superficial SSI (sSSI) while controlling for patient factors and surgical case mix. We tested associations for (1) all operating room personnel and (2) for three groups of personnel defined a priori as scrubbed surgical personnel, non-scrubbed surgical personnel, and anesthesia personnel.
Patients and Methods
Human subjects protections
The Institutional Review Board at Mayo Clinic, Rochester, MN, approved this study. The requirement for written informed consent was waived.
Identification of cases
For the purpose of quality improvement and external reporting, our institution maintains an internal database of SSIs (Infection and Prevention Control SSI database, Department of Infection Prevention and Control), which uses an electronic search algorithm, microbiology data, admission and surgical diagnostic listing to identify patients with potential SSIs from our electronic medical record. Two independent health-care providers (physicians and a nurse) validated these cases identified by this algorithm by manual chart review.
During the study period of January 2003 through December 2012, all adult patients with clean surgical incisions (uninfected/clean classification with primary closure) were identified [35]. Infections were classified as either superficial, deep, or organ space in our database, and only sSSIs were included in our final analysis for homogeneity of cases. The SSIs must have occurred within 30 days after the index surgery. Patients less than 18 years old or pregnant at the time of surgery were excluded.
To reduce misclassification of personnel exposure, we also excluded cases cared for by student registered nurse anesthetists [30]. To reduce potential spurious effects of after-hours care, we also excluded operations defined as those starting between 5
Identification of control subjects
Patients were matched by age (± 5 years), gender, American Society of Anesthesiology Physical Status (± 1), date of surgery (± 2 y) (to account for secular trends in SSI prevention practices), and Common Procedural Terminology® code. As many as three control subjects were assigned via proportional matching per patient based on availability of well-matched control subjects.
Measurement of operating room personnel
Intra-operative provider data were abstracted from the surgical information reporting system, which logs all surgical and anesthesia personnel who enter the operating room as part of the patient care team (including those providing meal/bathroom breaks). Each person is accounted for once during the case, and our system does not account for multiple badging.
Persons were grouped according to role and included surgical scrubbed personnel (staff surgeons, resident surgeons, surgical assistants, surgical technicians, physician assistants, nurse practitioners, and visiting clinicians), surgical non-scrubbed personnel (circulating nurses, peri-operative nurses, and surgical recorders), and anesthesia personnel (anesthesiologists, resident anesthesia physicians, and certified registered nurse anesthetists [CRNAs]). Rarely, additional personnel were also present in the operating room including product sales representatives and guest or medical/nursing student observers, whom we classified in this study as “other” personnel. Operating room personnel were classified by quartile for data analysis.
Demographic and co-variable data
Baseline demographic information and potential risk factors for sSSI were abstracted from the electronic medical record. Cases were grouped by surgical specialty (general, neurosurgery, orthopedic, spine, vascular). Times of day and operative duration were obtained from our surgical information reporting system.
Analytic approach
We present data as mean (± standard deviation) for continuous data or number (percent) for categoric data. Simple comparisons between the patient and control groups were performed with t-test or chi-square test as appropriate. Before hypothesis testing, we investigated potential multi-collinearity among variables specifying specific personnel groups and operative duration, and tolerance among the personnel groups and operative duration were greater than 0.5.
Conditional logistic regression was used to test the extent to which one additional operating room personnel, either in general or within each personnel group, was associated with sSSI while adjusting for known confounding variables. For the purpose of this study, we are assuming a direct relation between intra-operative personnel volume and operating room traffic. To avoid a potentially spurious finding, we explored multiple variable forms for operative duration to achieve maximal adjustment and to minimize residual confounding. To do this, we selected the variable form that resulted in the smallest odds ratio and least significant p value for effect of operating room personnel. All statistical analyses were performed using SAS® 9.4, Cary, NC.
Results
Baseline comparison of patients and control subjects
In all, 474 patients and 803 matched control subjects were included. There was a significantly higher proportion of patients with diabetes mellitus (23.6% vs. 16.6%, p = 0.0019), cerebrovascular disease (7.8% vs. 4.9%, p = 0.0314), and operative duration (2.5 ± 1.6 vs. 2.2 ± 1.5 h, p = 0.0004) compared with the control group (Table 1).
SD = standard deviation; BMI = body mass index (kg/m2); ASA = American Society of Anesthesiologists; COPD = chronic obstructive pulmonary disease.
Distribution of personnel by case status
Distributions of operative duration and total personnel among patients and control subjects were similar (Fig. 1), although more intra-operative personnel participated in the cases versus control subjects (14.4 ± 3.0 vs. 11.8 ± 2.8, p = 0.0002) (Table 2). The mean number of anesthesia in-room providers (defined as resident physicians and CRNAs) was greater among cases versus control groups (2.3 ± 0.9 vs. 2.2 ± 0.9, p = 0.0035). The mean number of surgical assistants/technicians was greater among cases versus control groups (1.7 ± 0.8 vs. 1.6 ± 0.7, p = 0.0353).
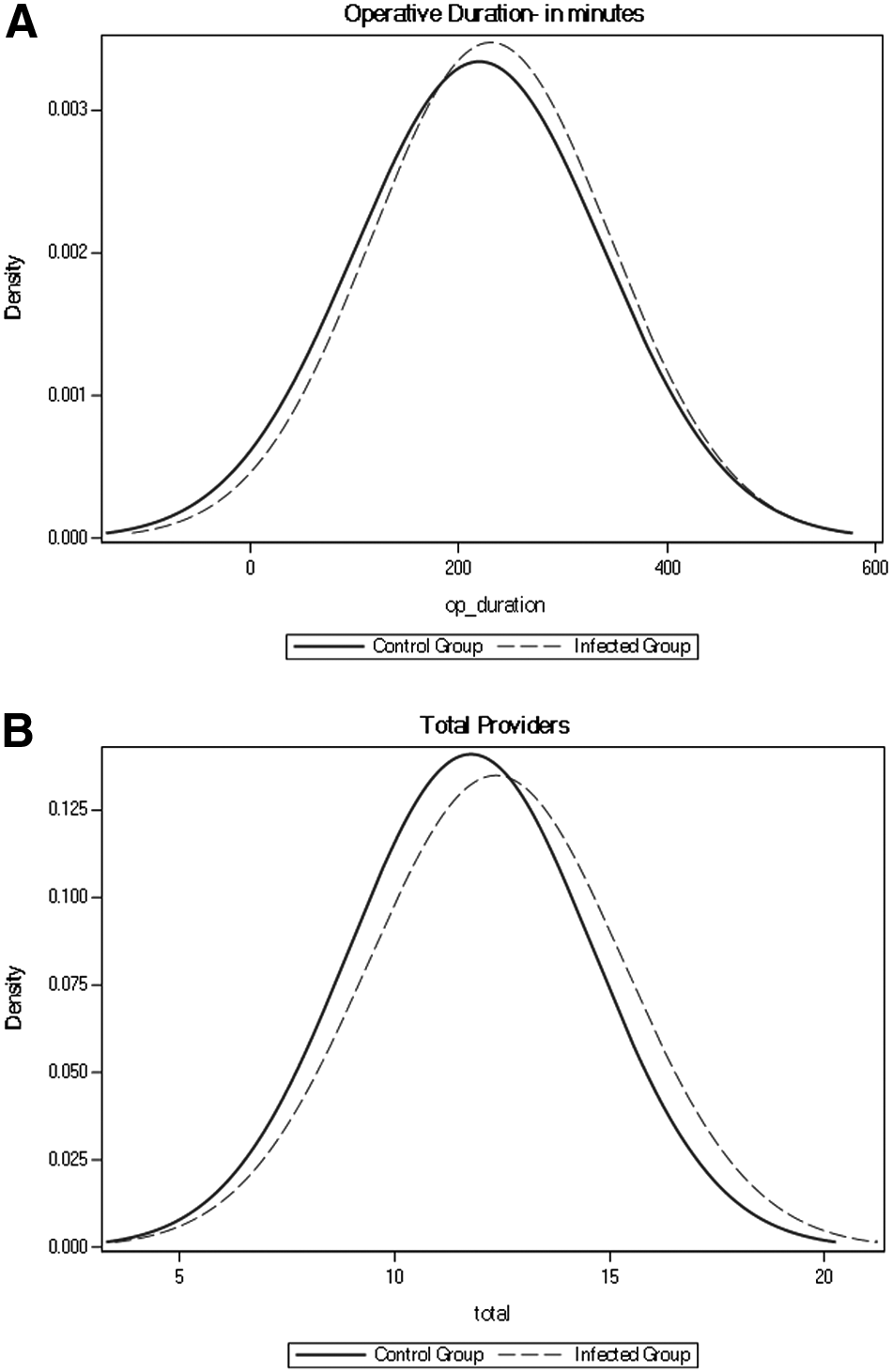
Distribution of operative duration (
SD = standard deviation; IQR = interquartile range.
Matched, unadjusted associations among personnel groups
Additional intra-operative personnel was associated with greater odds of infection in an unadjusted conditional regression model (odds ratio [OR] 1.082, 95% confidence interval [CI] 1.031–1.134, p = 0.0013). This association remained significant within each personnel group: surgical scrubbed personnel (OR 1.132, 95% CI 1.029–1.245, p = 0.0105), surgical non-scrubbed personnel (OR 1.123, 95% CI 1.008–1.251, p = 0.0357), and anesthesia personnel (OR 1.153, 95% CI 1.031–1.290, p = 0.0127). In an exploratory analysis including all three personnel groups in the same model, these associations were not statistically significant (Supplementary Table 1; see online supplementary material at ftp.liebertpub.com).
Matched, adjusted regression models among total number of personnel and personnel groups
After adjustment for operative duration and patient factors, the association between the number of intra-operative personnel and sSSI was no longer statistically significant for total personnel or for any of the three personnel groups. Other variables, however, were found to be associated independently with increased odds of sSSI, including diabetes mellitus and operative duration (Table 3).
OR = odds ratio; CI = confidence interval; BMI = body mass index.
Overall p values for operative duration covariate are 0.0027, 0.0009, and 0.0021 for surgical scrubbed, surgical non-scrubbed, and anesthesia personnel, respectively.
Sensitivity analyses
To evaluate for potential non-linear effects, each personnel group was evaluated as a categoric variable. No dose-response effects (e.g., greater number of personnel corresponding to greater risk) were found (Supplementary Table 2; see online supplementary material at ftp.liebertpub.com). In addition, measures of care process adherence (i.e., antibiotic administration) and operative intensity (i.e., estimated blood loss and transfusion) were compared between patients and control subjects, and differences were not statistically or clinically significant (Supplementary Table 3; see online supplementary material at ftp.liebertpub.com).
Discussion
We investigated the extent to which operating room traffic was a modifiable risk factor for sSSI by determining whether the presence of additional operating room personnel was associated with greater odds of sSSI. In this retrospective, case-control study, operating room traffic was not independently associated with sSSI overall or for any specific group of operating room personnel (scrubbed surgical, non-scrubbed, or anesthesia). The validity of these null findings was supported by the observed increase in sSSI with known risk factors such as operative duration and diabetes mellitus. Together, these findings suggest that limiting additional operating room traffic is not a strong modifiable risk factor for sSSI.
National guidelines have proposed that additional operating room personnel may represent a risk factor for SSI development and should be limited when possible [21]. These recommendations, however, are based on expert opinion and mechanistic plausibility rather than clinical data [34]. Several previous articles have suggested that operating room traffic may contribute to infection risk by disrupting airflow patterns, lapses in recommended aseptic technique, operating room distractions, operative delays, and handoff errors. These studies, however, do not directly address the relationship between operating room traffic and SSI risk, but rather evaluate several indirect markers of infection [19,22–25,30,33,36].
Some studies have demonstrated that the implementation of surgical care bundles focusing on operating room staff behaviors, including limiting operating room traffic, significantly decreased SSI rates [17,18,37]. These investigations, however, were not able to demonstrate the unique benefit of limiting operating room traffic because the care bundles included multiple elements of which limiting operating room traffic was just one part. In contrast to the above studies, the present study directly examined the association between operating room traffic and SSI as a primary end point and found no strong relation across all work groups.
This study benefited from a large, multi-specialty case mix focused on clean surgical incisions. One explanation for a lack of association between additional operating room personnel and sSSI may be uniformly high or low levels of operating room personnel in our population. Perhaps a threshold has been reached where further limiting operating room traffic will not have a significant effect on infection rate.
The presence and importance of exposure homogeneity cannot be assessed because there are no external benchmarks for the number of operating room personnel. Interestingly, the models did not demonstrate a significant association of elevated BMI as would be assumed [7,14,38], perhaps because of the relatively high mean BMI in our study population. The present study did, however, corroborate previously demonstrated significant associations between known risk factors of diabetes mellitus and operative duration with greater odds of sSSI [4,5,11].
Conclusions from this study are limited primarily by the retrospective, single-center design. It is possible that occasional personnel may have entered operating rooms to carry laboratory specimens or communicate about other matters, yet not have been recorded. We have no evidence, however, of this misclassification and do not believe this measurement error would contribute to a spurious finding. In addition, although we are highly confident in the validity of our search algorithm, there is a potential that some cases of SSI were missed by our system. This would, however, be a small number and unlikely to affect our findings. Finally, our analyses were intended as hypothesis-generating primarily and did not, by intent, adjust for multiple comparisons.
Conclusion
Additional operating room personnel were not associated with increased odds of sSSI in clean surgical incisions after adjusting for operative duration, patient factors, and for individual intra-operative personnel groups (surgical scrubbed, surgical non-scrubbed, and anesthesia personnel). This investigation did not find compelling evidence that operating room traffic is a modifiable risk factor for sSSI.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.