
Abstract
Abstract
Background:
The U.S. Centers for Disease Control requires 90 days after surgery using an implant to diagnose or show the absence of a surgical site infection (SSI). However, many databases only track outcomes up to 30 days. The cost and effort to increase follow-up to 90 days after surgery is high and the benefit is unclear. We hypothesize that the majority of SSIs after ventral hernia repair occur within 30 days of surgery.
Patients and Methods:
All patients who underwent ventral hernia repair (with or without mesh) from 2010–2015 at a single institution were evaluated for evidence of SSI. The duration between surgery and the diagnosis of a post-operative SSI was assessed. Baseline and operative characteristics were compared between patients with an early SSI (within 30 days of surgery) and those with a late SSI (more than 30 days after surgery).
Results:
Among 1,635 patients who underwent ventral hernia repair, 117 (7.2%) developed an SSI. The median (range) of days between surgery and SSI was 15 days (range, 2–763). There were 20 (17.1%) late SSIs diagnosed; of these, 17 were diagnosed between 31–90 d and three were diagnosed later than 90 days. Patients with a late SSI were more likely to have had a prior ventral hernia repair and have had biologic mesh (p = 0.001).
Conclusions:
Whereas the majority of SSIs after ventral hernia repair occurred within the first 30 days, a substantial number of late SSIs occurred. It is worthwhile to follow patients for at least 90 days post-operative in order to capture a more accurate picture of the true rate of SSI.
S
The follow-up recommended to identify an SSI is important in assessing clinical outcomes. Many databases, including the National Surgical Quality Improvement Project, only track outcomes for up to 30 days [4]. The cost and effort to increase follow-up to 90 days or even one year after surgery is high and the benefit is unclear. We hypothesize that most SSIs after ventral hernia repair are diagnosed within 30 days of surgery.
Patients and Methods
After receiving Institutional Review Board approval, records from a county-wide health care system (Harris Health System) were identified using ICD-9 and ICD-10 codes and reviewed for all ventral hernia repairs performed between 2010 and 2015. All ventral hernia repairs were included, including those with and without mesh and those that underwent concomitant procedures. Electronic medical records of these patients were assessed for development of an SSI after ventral hernia repair. Because this county-wide health care system has shared electronic medical records among 32 locations, robust long-term clinical follow-up is feasible.
Baseline characteristics, hernia details, and operative details were recorded. Mesh location was categorized as inlay, sublay, underlay, or multiple layer. Onlay repair was defined as mesh secured to the exposed anterior fascia. Inlay repair was defined as mesh placed within a defect and secured circumferentially to the edges of the fascia. Sublay repair was defined as either retrorectus or pre-peritoneal and is also referred to commonly as Rives-Stoppa. Finally, underlay repair was defined as mesh placed in the intra-peritoneal position and secured to the anterior abdominal wall. Patients who had mesh placed in more than one location were said to have multiple layer repair [5].
Surgical site infection was defined using the CDC definition and divided into superficial, deep, mesh, and organ/space infection. Superficial infections involved skin and subcutaneous tissues only. Deep infections involved the fascia or muscle layers. Mesh infections had specific documentation of mesh involvement. Finally, organ/space infections involved a part of the body deeper than the fascial/muscle layers. For all patients, days to initial diagnosis of an SSI were calculated. For patients with multiple types of SSI (i.e., superficial, deep, mesh, and organ/space), days to initial SSI were calculated from whichever SSI was diagnosed first, and days to the first presentation of each type of infection were also reported. Early SSI was defined as initial diagnosis of an infection 30 days or less after surgery, and late SSI was defined as initial diagnosis of an infection more than 30 days after surgery. Patient demographics, hernia characteristics, and operative details were compared between patients with early and late infections. Type of initial SSI was also compared between those with early and late infections.
Statistics
Categorical variables were compared using χ2 analysis. Parametric continuous variables were compared using Student t-test, whereas non-parametric continuous variables were compared using Kruskal-Wallis test. All analysis was performed using Stata® version 14.0 (StataCorp, College Station, TX).
Results
A total of 1,635 ventral hernia repairs were performed from 2010–2015 with a median (interquartile range, IQR) follow-up was 568 days (range, 163–1,102). Of these, 117 (7.2%) developed an SSI. Eleven patients developed a mesh infection. The median (range) of days between surgery and initial SSI diagnosis was 15 days (range, 2–763). There were 20 (17.1%) late SSIs. Of the late SSIs, 17 (14.5%) were diagnosed between 31–90 days, and three (2.6%) were diagnosed later than 90 days.
Patient demographics and hernia characteristics were similar between patients with early and late SSIs (Table 1). Patients with late SSIs were more likely to have had a prior ventral hernia repair. Operative details were similar between patients with early and late SSIs, except that patients with a late SSI were more likely to have had biologic mesh placed (Table 2).
Median (range).
SSI = surgical site infection; ASA = American Society of Anesthesiologists score.
Median (range).
SSI = surgical site infection.
Of the patients who developed an infection after 90 days, the first had a 1-cm incisional hernia from a previous trocar site at the umbilicus and underwent a laparoscopic hernia repair with mesh. The patient was started on antibiotics on day 93 for purulent drainage from the site. The second patient with an SSI after 90 days had a 2-cm incisional hernia from a previous trocar site at the umbilicus and underwent open hernia repair with mesh. When observed in clinic on post-operative day 526, this patient complained of a five-month history of purulent and bloody drainage from the site and ultimately underwent explantation of the mesh. The third patient with an SSI after 90 days had a 1-cm incisional hernia at the umbilicus and underwent suture-only umbilical hernia repair. The patient was observed in the emergency department on post-operative day 763 with one week of purulent drainage from an umbilical wound.
There was no difference in type of initial infection between patients with early and late infections (Table 3). The median days to infection by type of infection (superficial, deep, mesh, or organ/space) are shown in Table 4. Mesh infection had the longest median time to infection, at 29 days (Fig. 1). For mesh infections, almost half (5/11; 46%) were diagnosed after 30 days.
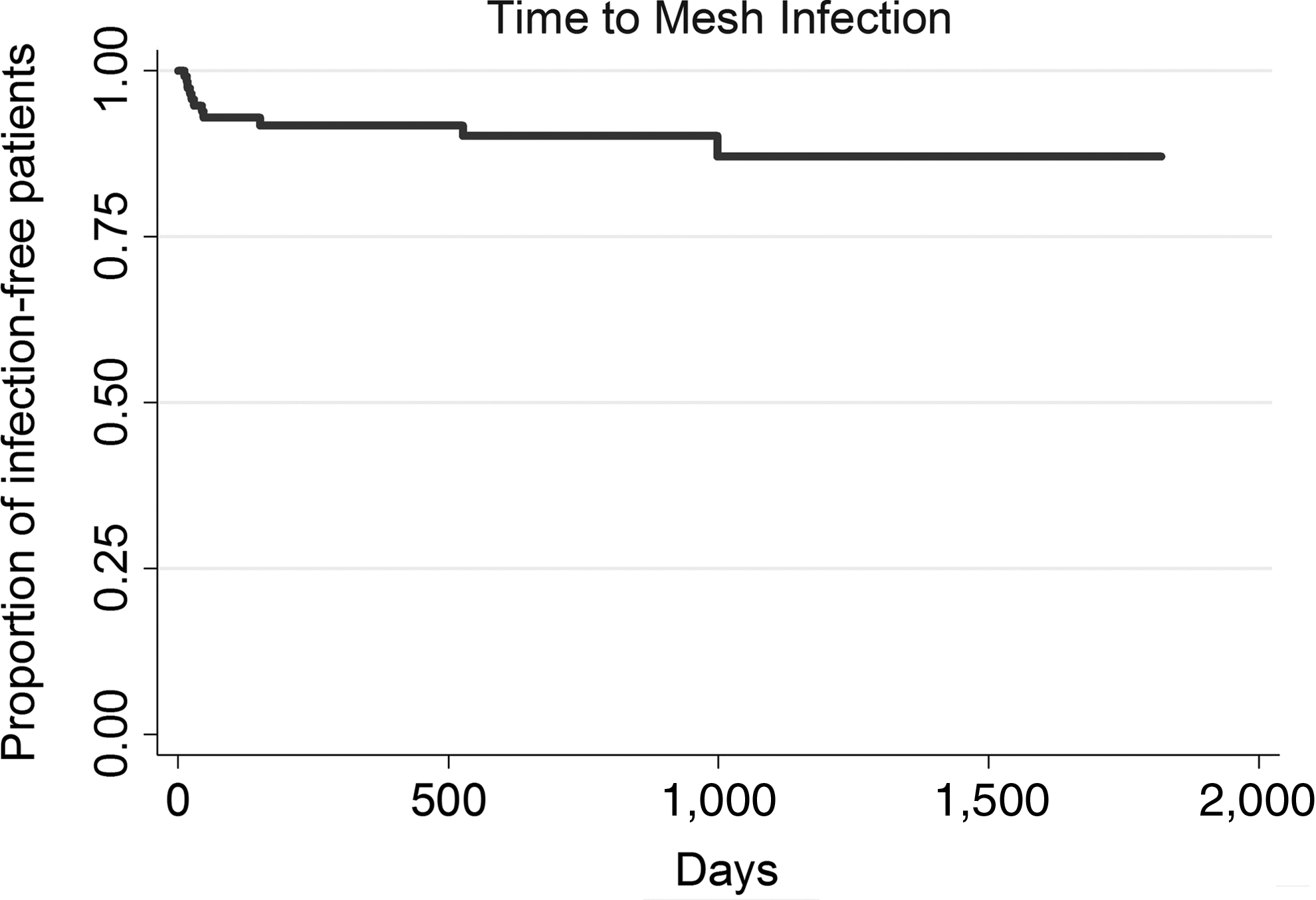
Kaplan-Meier curve showing time to mesh infection.
Multiple means more than one type of infection was present upon initial presentation.
Days to first presentation of specific type of infection, regardless of whether it was initial infection.
Median (range).
SSI = surgical site infection.
Discussion
In this study of more than 1,600 ventral hernia repairs, 17% of patients who developed a SSI were initially diagnosed 31 days or more after their surgery. This suggests that 30-days post-operative follow-up may be inadequate to identify and capture a substantial proportion of SSIs. Despite this, 30-days follow-up is accepted commonly and may result in an underestimation of the true prevalence of SSI. In addition, nearly half of all mesh infections were diagnosed after 30 days.
Other studies on the timing of SSIs have conflicting results. A study of breast implant-associated infections (n = 47) demonstrated that only 50% of infections were diagnosed within 30 days after surgery [6]. In contrast, a study of SSIs after total hip replacement and hemi-arthroplasty (n = 761) showed all infections—including superficial, deep and joint infections—occurred within 30 days post-operative [7]. However, the generalizability of these studies to ventral hernias is not clear. There are several hernia studies looking at the time to SSI, but most are limited by small sample size (n = 7–29) and the inclusion of inguinal and femoral hernias along with ventral hernias [8–10]. Despite these limitations, the results from these studies, all (including ours) seem to draw the same conclusion regarding mesh infections: on average, mesh infections present many months (range, 5.6–11.3) after surgery [10].
Of note is that the late infections did not follow complex ventral hernia repairs, but rather all followed small, simple hernia repairs. This suggests that even simple hernia repairs have the potential to lead to substantial complications later. Furthermore, the use of mesh was no different for those with early infections and those with late infections, further suggesting that we may not be able to predict who will develop a late infection. Surgical site infection has been shown to lead to a vicious cycle of complications, including hernia recurrence, re-operation, and repeat hernia repair [11]. Given these findings, it may be prudent to change the current paradigm in the perception and management of patients with a ventral hernia. Drawing a parallel from the field of oncology in which annual follow-up with clinical and radiographic re-assessment is common and routine, ventral hernias may need to be considered a chronic illness in which re-operations and recurrences are common and infections can present months or years after surgery [11]. Consideration of measuring outcomes in terms of complication-free months after surgery may provide a more useful measure of the risks and benefits of management plans.
In tracking clinical outcomes, increasing the length of follow-up to better capture SSI is not without challenges. Longer follow-up means higher cost, which may be a prohibitive barrier to a study, institution, practice, or health care system. In addition, attempting to reach patients months after surgery may not be feasible in a highly mobile society. However, several studies have identified possible methods for SSI surveillance [12–14]. Office visits with direct observation of the site by the surgeon may be the most reliable method for detecting an SSI and other complications (such as hernia recurrence), however, this can be costly, time consuming, and sometimes not feasible if the patient has moved away. Alternatives include telephone interviews and patient questionnaires asking patients about visits to outside clinics or hospitals and to describe their incisions [12]. However, several studies have attempted to validate patient self-diagnosis of an SSI with only moderate success [12]. Another study has suggested telephone calls by a trained surveillance nurse augmented by a home visit when alerted to a potential infection [14]. Furthermore, this study suggests that the cost of the surveillance nurse and home visits is less than the cost of an untreated SSI [14].
Although only 2.6% of patients in this study developed a late SSI, other long-term complications after ventral hernia repair are common. At 10 years of follow-up, the hernia recurrence rate has been reported as 37% for primary ventral hernias and 64% for incisional hernias [11], further suggesting that ventral hernias should be considered as a long-term disease. In order to achieve a paradigm shift in the care of patients with ventral hernias, collaboration among patients, clinicians, health care systems, and payers is needed. A push for annual follow-up and on demand imaging, reimbursement for long-term follow-up, and development of a medical counterpart to a surgical herniologist (i.e., cardiology to cardiac surgery, oncologist to surgical oncologist) may be needed. The first step to achieving these goals may be to consider a ventral hernia a chronic disease.
There were several limitations to this study. The definition of SSI is complex and can be difficult to determine using medical records alone. To improve reliability, we used two independent, trained reviewers to determine SSI. In addition, patients who followed up at an institution outside our county system would have been missed. However, as a safety-net hospital, the number of patients who seek care elsewhere is low and not likely to change our results drastically. With more robust follow-up, only more late SSIs would be identified, reinforcing our findings. In addition, some SSIs may have developed before they were diagnosed, which could have decreased overall time to initial infection. Because this was a retrospective study, we were limited to the date of infection as documented in the medical record. Furthermore, the generalizability of these results to other types of surgery is unknown and further research is warranted.
Conclusions
Whereas the majority of SSIs after ventral hernia repair occurred within the first 30 days, a substantial number of late SSIs occurred. It may be worthwhile to follow patients for at least 90 days post-operative in order to capture a more accurate picture of the true rate of SSI. In addition, a paradigm shift to think of ventral hernias as a chronic disease may be in order.
Footnotes
Author Disclosure Statement
No competing financial interests exist.