
Abstract
Abstract
Background:
Coccidioidomycosis, commonly called “valley fever,” “San Joaquin fever,” “desert fever,” or “desert rheumatism,” is a multi-system illness caused by infection with Coccidioides fungi (C. immitis or C. posadasii). This organism is endemic to the desert Southwest regions of the United States and Mexico and to parts of South America. The manifestations of infection occur along a spectrum from asymptomatic to mild self-limited fever to severe disseminated disease.
Methods:
Review of the English-language literature.
Results:
There are five broad indications for surgical intervention in patients with coccidioidomycosis: Tissue diagnosis in patients at risk for co-existing pathology, perforation, bleeding, impingement on critical organs, and failure to resolve with medical management. As part of a multidisciplinary team, surgeons may be responsible for the care of infected patients, particularly those with severe disease.
Conclusion:
This review discusses the history, microbiology, epidemiology, pathology, diagnosis, and treatment of coccidioidomycosis, focusing on situations that may be encountered by surgeons.
C
Although coccidioidomycosis was limited historically to individuals living in specific geographic locations, the expansion of its endemic range, the increased frequency and availability of domestic and international travel, and a growing number of immunosuppressed patients have expanded the potentially susceptible population. As part of a multidisciplinary team, surgeons may be responsible for the care of infected patients, particularly those with severe disease. This review discusses the history, microbiology, epidemiology, pathology, diagnosis, and treatment of coccidioidomycosis, focusing on situations that may be encountered by surgeons.
History
The first description of a case of coccidioidomycosis was published in 1892 by Alejandro Posadas, an intern (and future surgeon) working in Buenos Aires [1]. As a medical student, he described a 36 year-old soldier who developed recurrent fever, ulcerative cutaneous vegetations, and papules [2]. The condition was initially believed to be a malignant skin disease, but biopsies of the lesions revealed organisms similar to the protozoan Coccidia. The next reported case occurred in a manual laborer in the San Joaquin Valley, who developed cutaneous lesions similar to those described by Posada. During autopsy of this man, organisms appearing similar to the protozoan were identified through a collaboration between a surgeon at Cooper Medical College in San Francisco (later to become Stanford Hospital) and pathologists at Johns Hopkins Medical School [1,3]. The route of transmission remained unknown. However, in 1929, a Stanford medical student inhaled Coccidioides spores while performing research and developed the reported signs and symptoms. This infection triggered an investigation into the respiratory transmission of the organism [1,3].
During the early part of the 20th Century, migrants leaving the Dust Bowl in the American Midwest traveled to the Central Valley of California seeking employment. This influx of migrant agricultural workers rapidly increased the population exposed to infective Coccidioides spores and to the numbers of persons infected. As the U.S. was entering World War II, military personnel, Japanese-American internees, and Axis prisoners of war were moved to bases and camps in the San Joaquin Valley [1]. These populations permitted a series of large epidemiologic studies during the 1930s and early 1940s that provided local researchers and public health authorities the opportunity to further our understanding of the microbiology, epidemiology, and pathophysiology of coccidioidomycosis [1].
Microbiology and Pathogenesis
The dimorphic fungal organism responsible for coccidioidomycosis, genus Coccidioides, is comprised of two genetically distinct species, C. immitis and C. posadasii, historically termed “Californian” and “non-Californian,” respectively [3–5] Coccidioides spp. are saprophytic fungi limited to the Western Hemisphere between the north and south 40° latitudes. These fungi grow in mycelial form in dry desert soil, specifically the Lower Sonoran Life Zone, an area characterized by low rainfall (10–50 cm per year), rare winter freezes, and alkaline soil [4,6]. In the United States, these areas include parts of Texas, Arizona, New Mexico, and central and Southern California. Outside of the United States, endemic regions for Coccidioides spp. include Mexico, Brazil, Argentina, Bolivia, and Paraguay (Fig. 1) [4]. When growth conditions are favorable, the saprobic phase predominates, with the fungus commonly existing in mycelial form about 10–30 cm beneath the surface [3,5]. However, when the soil dries or nutrients are limited, hyphal death occurs, leaving arthroconidia (spores). Under ideal conditions for the organism, these spores remain viable, and infective, for many years [7]. They are easily aerosolized when the host soil is disrupted by environmental or human activities.
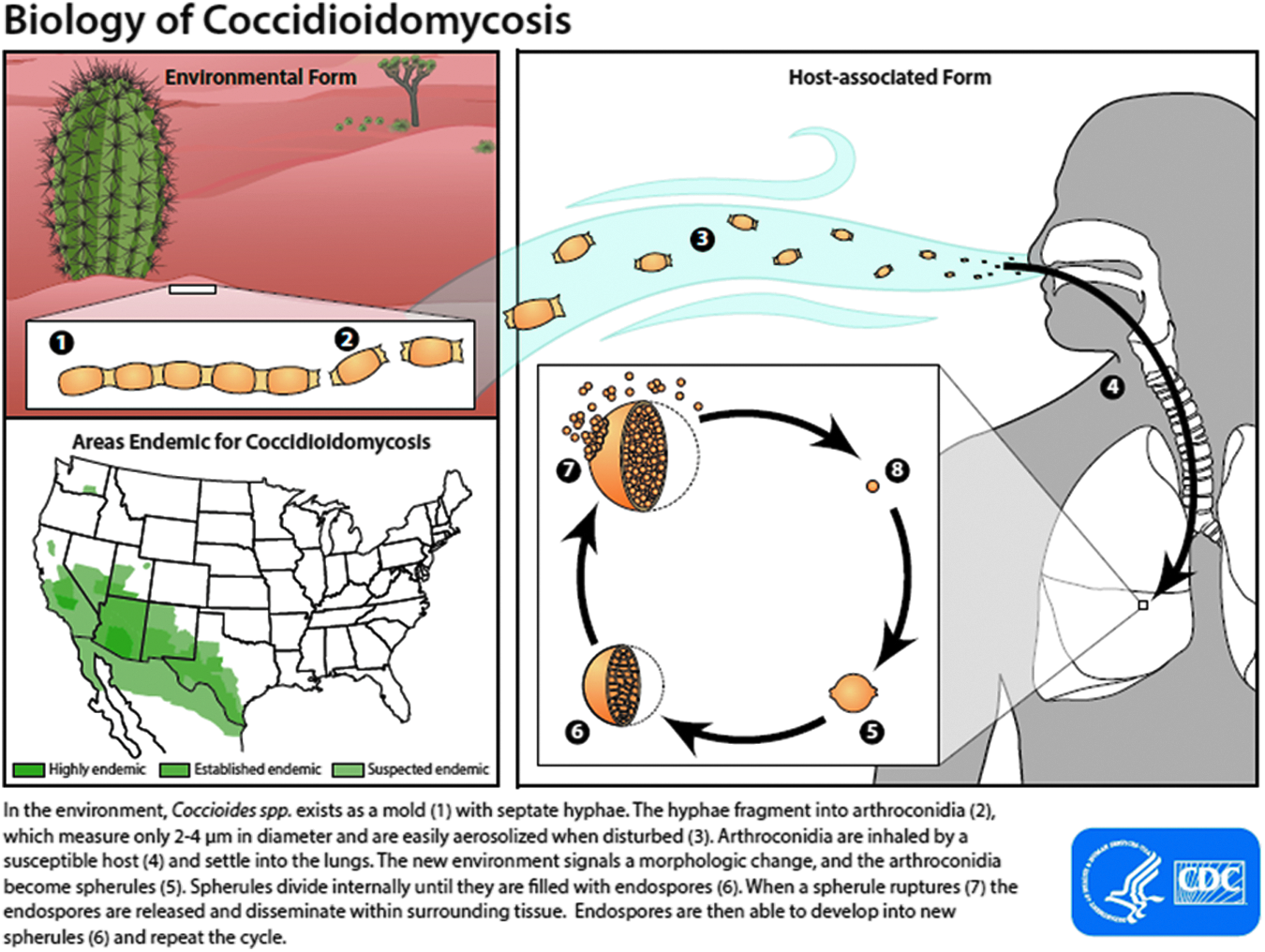
Figure legend incorporated into image provided courtesy of the U.S. Centers for Disease Control and Prevention. Color image is available online at www.liebertpub.com/sur
As a rule, coccidioidomycosis is not transmitted from person to person; nearly all infections are associated with exposure to contaminated dust or soil [4]. Rare cases have been described of transmission through direct inoculation among laboratory workers or through organ transplantation [5,8]. Patterns of human infection are believed to parallel the geographic distribution of the organism; in fact, what is commonly believed to be the geographic range for Coccidioides spp. has been extrapolated from the epidemiology of human infections and sero-reactivity [3]. Most infections in the United States occur among persons living in the desert Southwest [9]. Additionally, rates of coccidioidomycosis tend to increase during the summer and fall, which correspond to periods of low rainfall and drier soil [3,5]. Notably, fungi transported by infected travelers can establish new micro-foci of endemicity, as has been observed in Washington State [10].
Human infection, heralding the parasitic phase of the organism, begins after inhalation of aerosolized arthroconidia. The number of arthroconidia needed to produce infection is presumed to be quite small, given the brief exposure in an endemic area that may result in symptomatic infection [3]. These arthroconidia, which are 2.5 to 4 mcm in width and 3 to 6 mcm in length, are small enough to reach the alveoli of the lungs when inhaled [5]. In the alveoli, the fungus begins a unique life cycle of alternating large spherules and progeny endospores. First, in the lungs, over a four-d period, the inhaled arthroconidia change morphologically into large endospore-containing structures called spherules; these are capable of containing 100–300 endospores [4]. These spherules can rupture, resulting in lymphatic or hematogenous spread of endospores (Fig. 2) that are associated with satellite nodules. Each of these endospores is capable of developing into an independent spherule and can propagate another cycle, resulting in the seeding of distant organs [7].
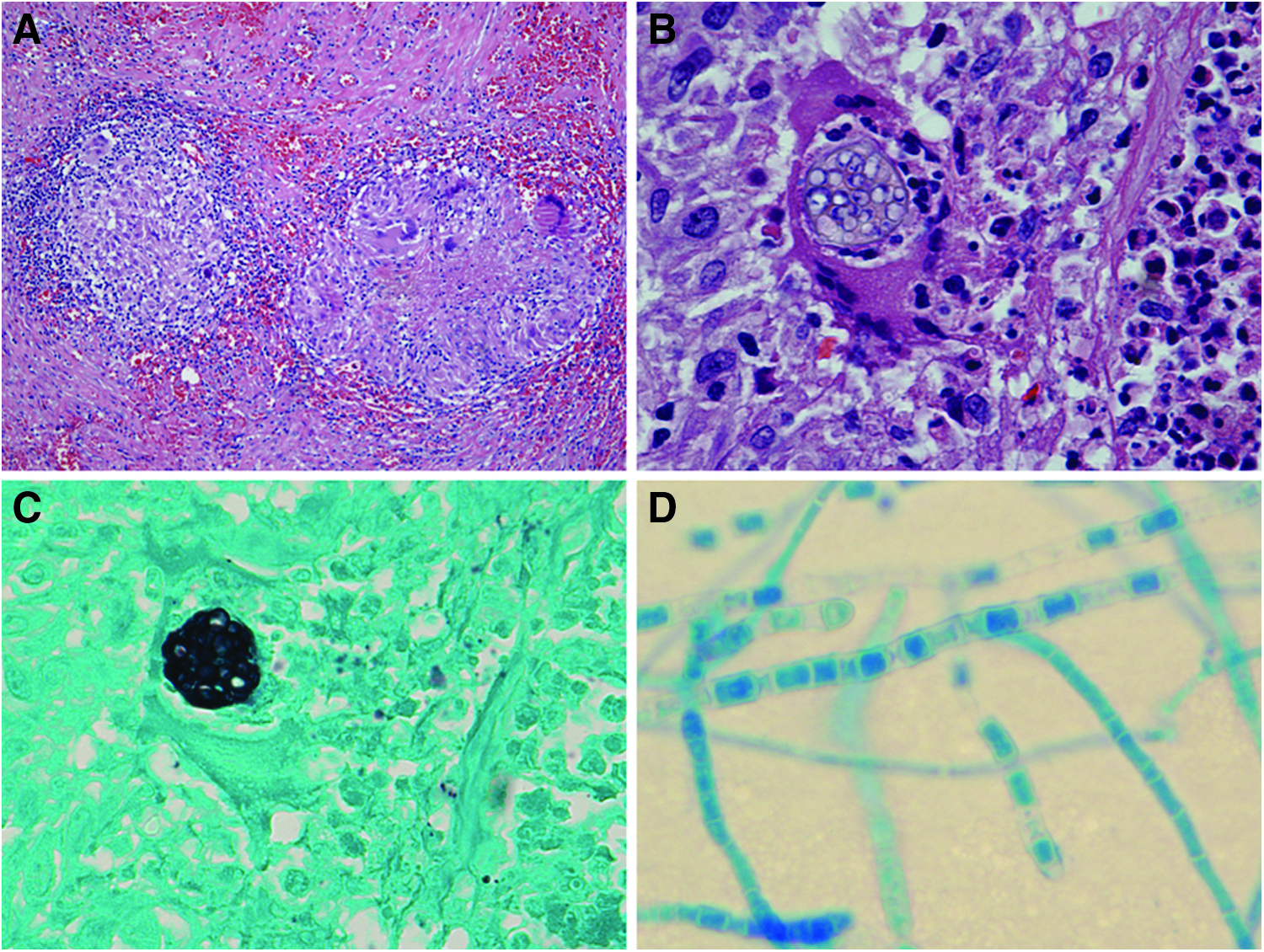
Histopathology review and fungal culture. (
Clinical Manifestations
Primary pulmonary disease
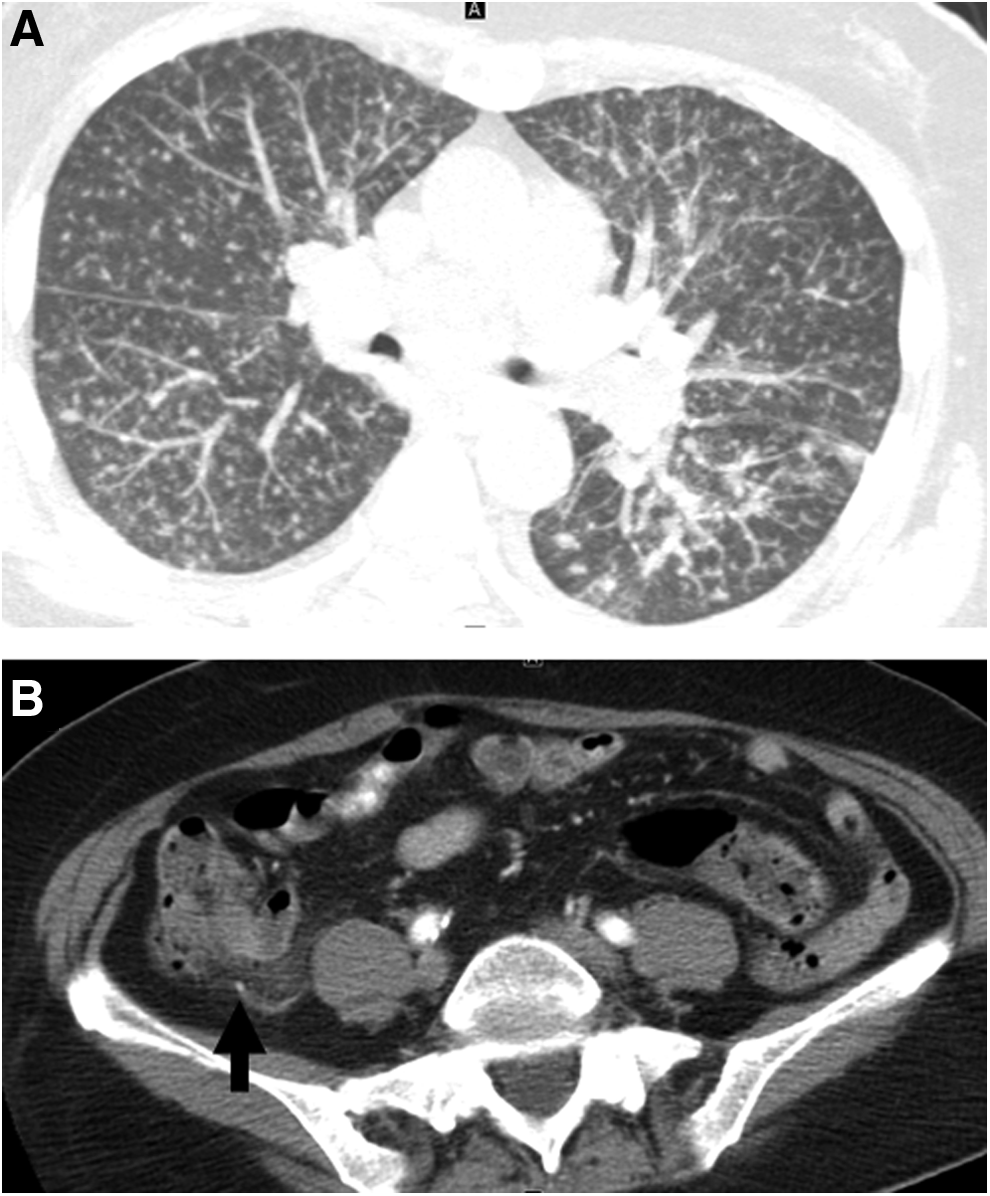
The majority of Coccidioides spp. infections are asymptomatic or subclinical (60%); only 30%–40% of persons who inhale arthroconidia ever display symptoms [3,11]. When symptomatic, coccidioidomycosis most commonly presents as a flu-like illness with signs and symptoms that include cough, fatigue, chest pain, fever, hemoptysis, weight loss, dyspnea, malaise, night sweats, and chills [11–13]. These signs typically become evident one to three wks after infection [11]. In endemic areas in the U.S., primary pulmonary coccidiodomycosis may account for 15% to 30% of persons with community-acquired pneumonia [13,14]. On radiographs or computed tomography (CT) scans, primary pulmonary coccidioidomycosis can appear as patchy unilateral or bilateral consolidations, isolated nodules, or cavitary lesions (Fig. 3) [15]. Pleural effusions and hilar adenopathy may be present also [5]. For patients with mild disease, symptoms may persist for weeks to months; fatigue may be particularly problematic, interfering with the activities of daily living [11]. Approximately 10%–30% of primary pulmonary infections are associated with a diffuse erythematous rash, which commonly resolves prior to medical evaluation but which should not be confused with valley fever [5,16].
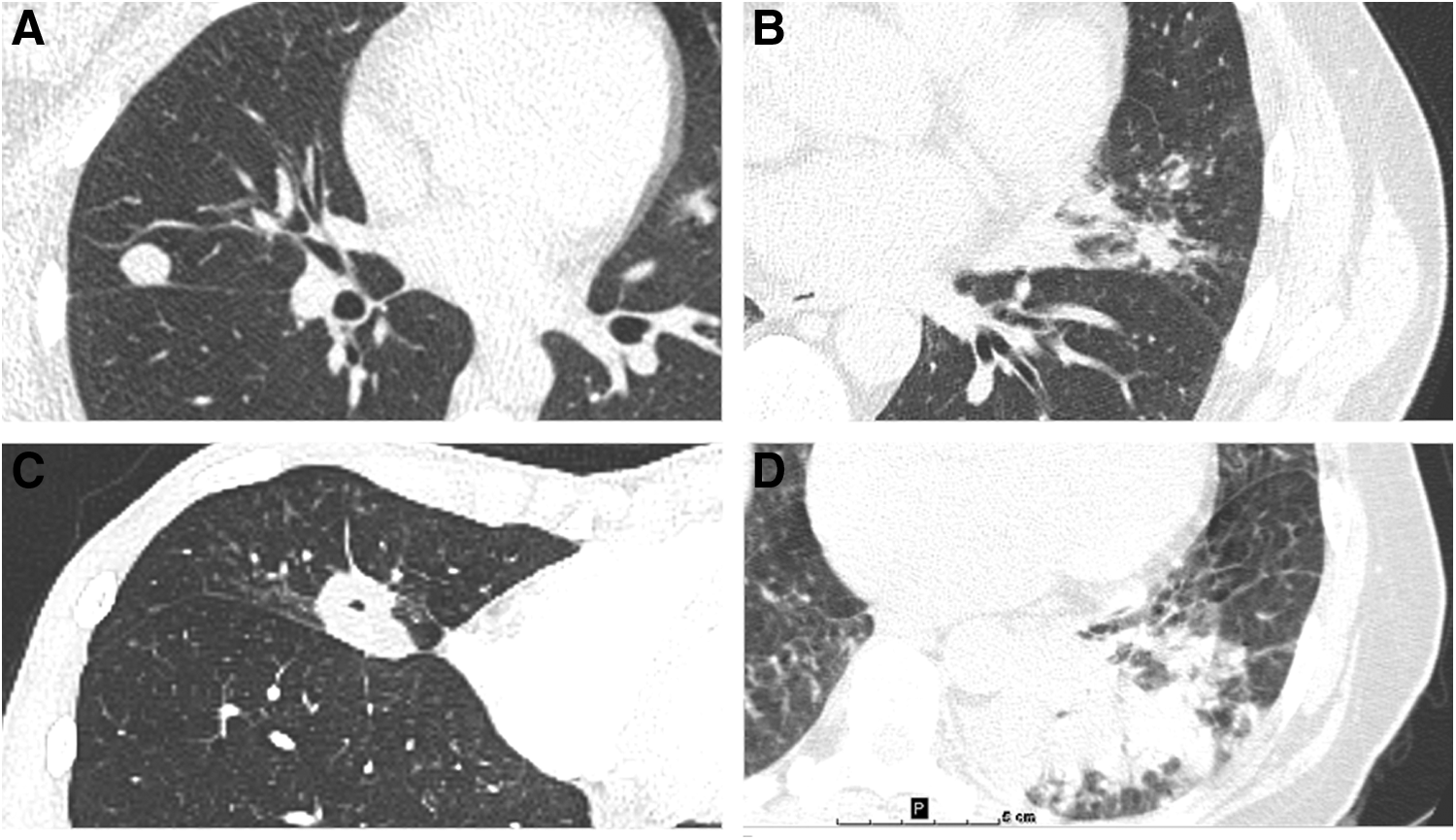
Pulmonary manifestations of coccidioidomycosis from four patients. (
Valley fever
Approximately 5% of all infected patients develop valley fever, characterized by erythema nodosum, erythema multiforme-like exanthem, arthralgia involving the ankles and knees, and mild conjunctivitis. Erythema nodosum typically begins as bright red lesions on the lower limbs that become darker red or purple within days and is most commonly found in Caucasian females [5]. As these lesions heal, they appear bruise-like [5]. Both the development of erythema nodosum and the erythema multiforme-like exanthema are considered favorable prognostic signs, portending an immunologic response to the infection [17,18]. Arthritis occurs in approximately one-third of the patients with these dermatologic lesions [5]. Fungal elements are not observed in either the dermatologic lesions or the joints affected; the symptoms are believed to be attributable to the immune response to the primary pulmonary infection [5].
Persistent pulmonary disease
Although most coccidioidal infections are self-limited and resolve irrespective of anti-fungal use, approximately 5%–10% of primary infections result in pulmonary sequelae (Fig. 4) [11,12]. Persistent pulmonary infections manifest as solitary nodules (coccidioidomas), chronic pneumonia, miliary disease, or pulmonary cavitation (Fig. 5). Unlike histoplasmosis lesions, coccidioidal nodules rarely calcify [19]. Peripheral blood eosinophilia is a common hematologic derangement observed with persistent pulmonary disease [5]. The classic radiographic sign of persistent pulmonary coccidioidomycosis is the thin-walled cavity without surrounding tissue reaction [5]. When compared with malignant lesions, cocciodioidal lesions tend to be less 18fluorodeoxyglucose avid on positron emission tomography with CT [20].
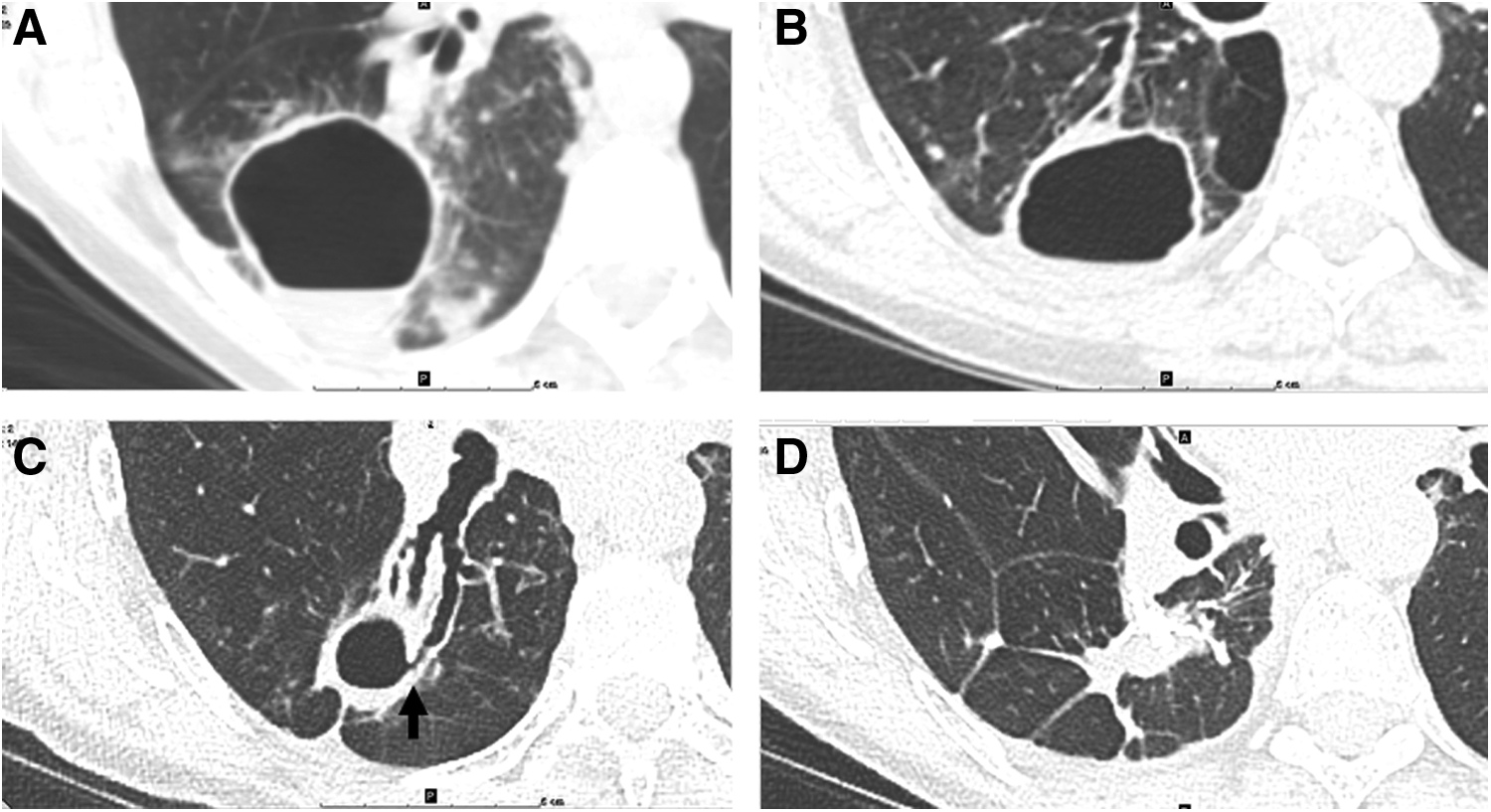
Evolving coccidioidomycosis cavity in 52 year-old female from the California Central Valley with longstanding cough and fever. (
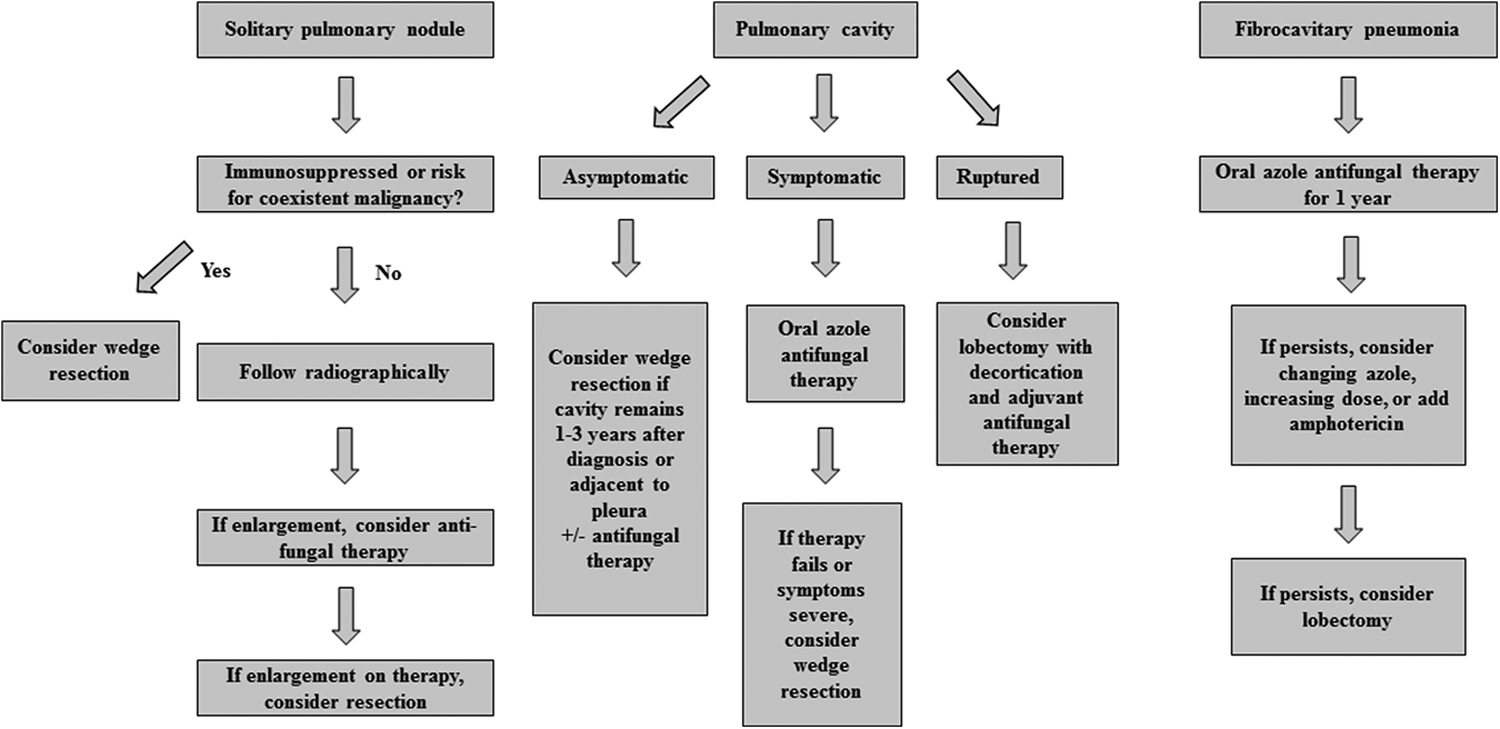
Decision-making algorithm for patients with pulmonary coccidioidomycosis.
Surgery has long been utilized as a therapeutic and diagnostic intervention for persistent pulmonary coccidioidomycosis [21–23]. Common indications for surgery include the need for diagnosis of an asymptomatic nodule, symptomatic nodules, cavities that do not resolve with antibiotic therapy, thin-walled cavitary lesions that rupture, or, rarely, coccidioidal empyema [12,15]. Thoracic disease is the most common indication for surgery in children with coccidioidomycosis [24]. Surgical intervention for coccidioidomycosis can be broken down broadly into operations performed for diagnostic purposes and those performed for therapeutic reasons. The surgical decision-making algorithm differs according to the indication (Fig. 5).
Differentiating early lung cancer or metastatic pulmonary disease from coccidioidoma can be challenging based solely on clinical and radiographic findings. In a single-institution series, 17 (29%) of 58 patients who underwent pulmonary resection for asymptomatic nodules suspected to be coccidioidomycosis had a concomitant diagnosis of lung cancer, underscoring the importance of resecting these lesions [15]. Particularly in patients with risk factors for lung cancer, resection should be discussed early. In this series, patients with cavitary lesions were more likely to be symptomatic on presentation (70%) than those with solitary nodules (10%); regardless of etiology, symptoms resolved in most patients after surgery (97%) [15]. Cavitary lesions that ruptured were associated with a longer median hospitalization (five days; range: Three–eight days) and accounted for a greater percentage of attributable morbidity (56%) and deaths [12,15]. Both nodules (68%) and cavitary lesions (47%) were commonly treated successfully with wedge resection [12].
Pleural effusions are estimated to occur in 5%–15% of patients with primary pulmonary infection and tend to occur more frequently on the left [25,26]. These effusions are often exudative with lymphocyte or eosinophil predominance [19]. Coccidioidal empyema occurs in approximately one quarter of pleural effusions [25,26]. Notably, coccidioidal involvement of the pleura necessitating decortication has been reported in 7% of patients requiring operative intervention for pulmonary disease; this is more common among patients with cavitary lesions [27]. Encouragingly, the mortality rate is low in patients who undergo surgical intervention for coccidioidal empyema [28].
Although historically, open thoracotomy has been the operation of choice for pulmonary coccidioidomycosis, video-assisted thoracoscopic surgery (VATS) is a demonstrably efficacious modality. A recent retrospective review of patients with pulmonary coccidioidomycosis treated by VATS or thoracotomy demonstrated reduced complications (n = 11/55 [20%] vs. 1/3 [33%]; p < 0.05) and hospital length of stay (3.3 ± 1.65 days vs. 6.0 ± 1.25 days; p < 0.05), respectively, although the duration of anti-fungal therapy was equivalent [12]. In another single-institution study, morbidity was statistically similar for the two surgical modalities, although a selection bias against VATS is evident in patients with more severe disease [15]. However, as surgeon comfort with VATS increases, it is probable that VATS will be used increasingly to treat complicated pulmonary coccidioidomycosis. For example, at the Mayo Clinic, the proportion of coccidioidomycosis cases performed using VATS doubled between 1998–2004 and 2005–2008 [15]. As more cases are performed using VATS, it will be critical to track outcomes; the geographic focality of coccidioidomycosis makes it an ideal condition for developing inter-institutional collaborations to optimize management [29].
Disseminated disease
Dissemination occurs early in infection, with common affected sites being the skin, lymph nodes, bones, and joints (Figs. 6 and 7). Less common but more severe infections occur at sites such as the central nervous system and the abdominal cavity [6]. When dissemination occurs to more than one site, the overall mortality rate is greater than 50% [5]. Approximately 1%–3% of immunocompetent persons of Caucasian ancestry with primary infection will experience disseminated disease [6]. This percentage is several times greater for persons of African or Filipino ancestry. Among immunosuppressed persons, dissemination occurs in approximately 30%–50% of symptomatic patients [9,11]. Dissemination is more common in adults than in children and among pregnant women, particularly those in their third trimester [30]. During outbreaks, the frequency of patients with disseminated disease may increase to 4%–5%, which is believed to be attributable to a larger inoculum [5].
Hematogenously disseminated coccidioidomycosis. (
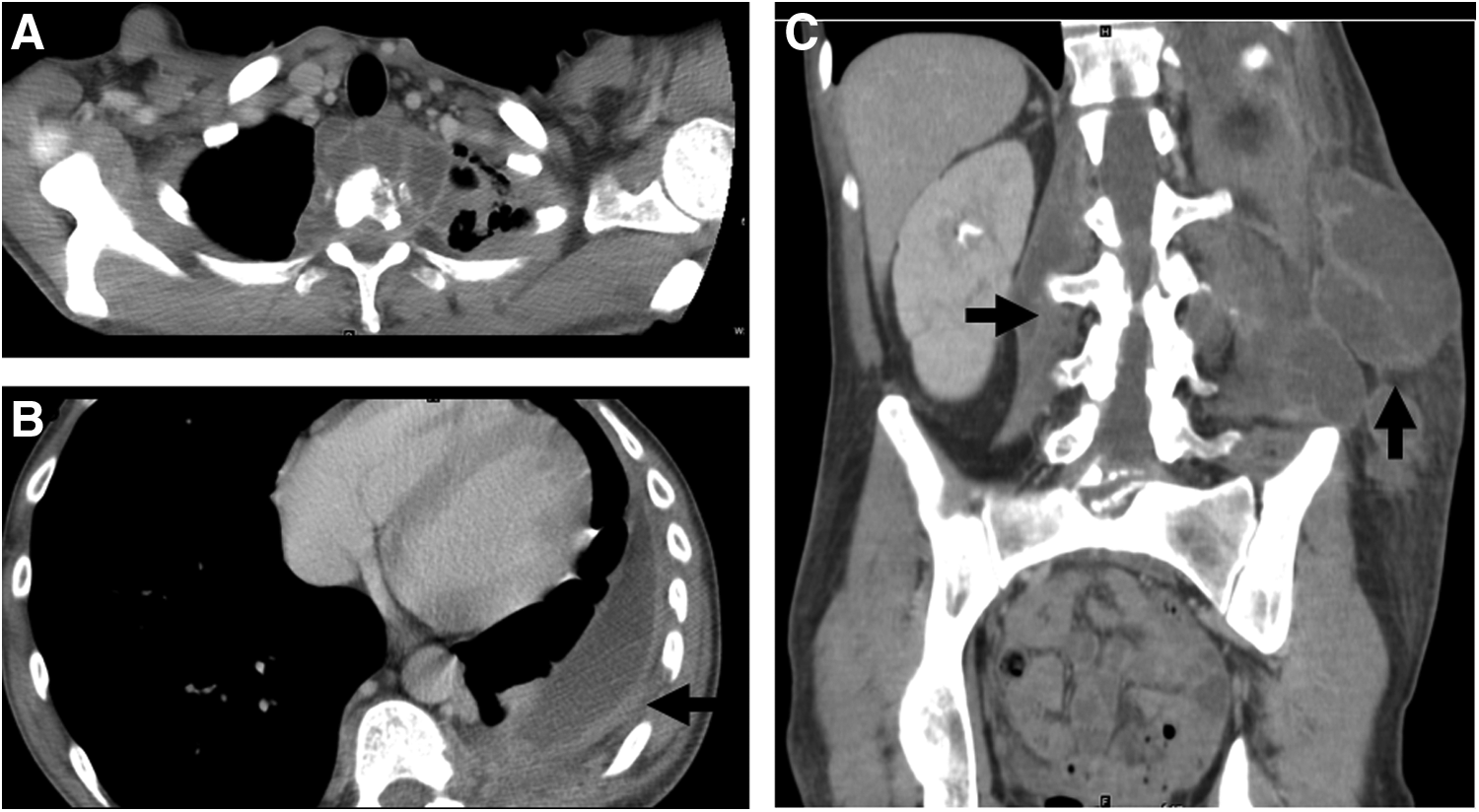
A 31 year-old man with night sweats, anemia, and 100 lbs of unintentional weight-loss over prior 12 months, who presented with multi-focal pain. (
Central nervous system
Central nervous system (CNS) involvement can be a particularly debilitating manifestation of disseminated disease and occurs in 30%–50% of these patients [5]. Often manifesting as epidural abscess or meningitis, it can present as rapid quadraparesis, cerebral abscess, and multiple lytic bone lesions (Fig. 7) [31–33]. Central nervous system vasculitis leading to ischemia, infarct, and hemorrhage is highly morbid and can be life-threatening [11]. Without treatment, CNS disease is nearly always fatal within two years of the primary infection [5]. Obstructive hydrocephalus may be encountered as a result of meningeal coccidioidal disease. In a review of 44 patients with hydrocephalus as a result of cranial coccidioidomycosis, a total of 99 shunting procedures were required [34]. The mean age of the patients in this series was 37 years; 63% were male, and patients of Asian or African descent were over-represented, consistent with the known demographic at risk for disseminated disease [34]. Shunt failure was common, with an average of 2.5 shunt revisions (range 1–8) being needed, most often (81%) as a result of mechanical blockage [34].
Musculoskeletal/cutaneous infections
Although joint inflammation associated with valley fever is a sterile arthritis, disseminated disease results in infected bone and joints in 20%–50% of cases [35]. The axial skeleton is the most common site of dissemination, the vertebral column in particular [35,36]. Infection typically begins in the cancellous bone, spreading to the periosteum and eventually extending into adjacent soft tissue [35]. Radiographically, lesions tend to appear lytic or “punched out” and often are multi-focal [37]. Given common presentation patterns and radiographic signs, spinal coccidioidomycosis may be confused with Pott's disease. Isolated coccidioidal lytic bone lesions also may mimic primary neoplastic processes [38]. Spinal involvement may be particularly troubling to treat. In a series of 16 patients with spinal disease, surgery was required in 12, often without achieving eradication of the organism [39]. Bone and joint disease associated with disseminated coccidioidomycosis also affects children, and the need for surgical intervention and debridement has been equivalent to the rate in the adult population in the few published series [40–42]. One particularly dramatic and severe site of dissemination is the chest wall, which necessitated sternal resection and radical reconstruction in the two cases in which it was described [43].
Although the joint space is a less common site than skeletal coccidioidomycosis, it can result in morbid disease in both infected native and prosthetic joints, thus necessitating surgery [44,45]. The knee is the joint most commonly affected, although infection of most major joints has been described [35,42,46]. Coccidioidal tenosynovitis is less commonly observed than skeletal or joint infection, yet it can be debilitating. A review of nine patients with tenosynovitis showed a relapse rate of nearly 50%, suggesting the importance of long-term anti-fungal use potentially combined with surgical intervention [47]. Operation for bone or joint coccidioidomycosis should focus on debridement or removal of all infected tissue or the prosthesis [48]. Infection at these sites can be particularly troubling to treat and in many cases at best result in arrest of further infection rather than “cure.” These patients often require lifelong antibiotic therapy after surgery.
Skin and soft tissue cocccidiomycosis may occur in 15% to 67% of patients with disseminated disease and may present as papules, nodules, pustules, verrucous plaques, subcutaneous abscesses, phlegmon, or sinus tracts [16]. These lesions commonly are painless. As many as 90% of patients with skin and soft tissue disseminated disease will have foci in other sites, necessitating a search for other infectious metastasis in these situations [16,49]. Lymph node infection is common after dissemination, and the supraclavicular and cervical nodes are commonly involved [16]. Nodal disease may lead to retropharyngeal abscess or neck mass, or the abscess may develop on its own, irrespective of nodal disease [28,50]. Once abscesses have developed, surgical drainage and control in addition to anti-fungal therapy often is necessary, particularly in lesions recalcitrant to initial anti-fungal therapy. Head, neck, and retropharyngeal abscess in particular require prompt surgical drainage [51].
Abdominal infection
Abdominal manifestations of coccidioidomycosis are rare. They commonly mimic other conditions such as abdominal malignant disease or abscess [52]. Patients with abdominal coccidioidal infection might be believed to have malignant disease, as they often presented with intra-abdominal deposits, plaques, and ascites, sometimes with an elevated CA-125 concentration in the limited case reports available [28,52–61]. Often, these patients are erroneously believed to have peritoneal carcinomatosis or tuberculosis. In patients living in endemic areas or with a history of travel, serology can help the astute clinician explore coccidioidomycosis as a possible cause. Similarly, abdominal coccidioidomycosis has been misdiagnosed as appendicular abscess, iliopsoas abscess, adnexal abscess, and pancreatic mass, as these presentations are similarly infrequent [62,63]. Retroperitoneal abscess may represent extension from the spinal cord, and osseous involvement should be evaluated prior to abdominal operation if possible. One case of small bowel disseminated disease has been described [64]. In historic autopsy series, splenic abscess from coccidioidomycosis was found to be common, although currently, it is reported rarely [36].
Unique manifestations
Other less common manifestations of infection resulting in surgery include endocarditis, pericarditis, infected ventral hernia mesh, prostatitis, endometritis, thyroiditis, endopthalmitis, retinitis, renal parenchymal disease, and epididymal disease (Fig. 8) [28,65–76]. The sheer variety of its presentation underscores that for any unusual infection developing in a person who lives in, or has traveled to, an endemic region, coccidioidomycosis should be considered. Readers are referred to those specific reviews for additional information.

A computed tomography scan of a patient's abdomen demonstrating 3.8-cm fluid collection (white arrow) consistent with coccidioidomycosis infection adjacent to surgically implanted mesh. Mesh was seeded hematogenously after pulmonary infection. Left side of image is patient's right; superior side of image is patient's anterior abdominal wall.
Epidemiology
An estimated 150,000 cases of coccidioidomycosis occur annually in the United States [11]. Importantly, the incidence is increasing, from 5.3 per 100,000 population in endemic regions in 1998 to 42.6 per 100,000 in 2011; this rise has been attributed predominantly to population influxes into California and Arizona [9,11]. Despite the increase in cases, the mortality rate has remained stable at approximately 0.6 per million person-years [77].
The most important risk factor for coccidioidomycosis is travel to, or residence in, an endemic area. Groups with extended and intense exposure to arthroconidia are at the highest risk [3]. These groups include construction workers, agriculture workers, persons working outside, and persons living around construction or work zones [78]. Outbreaks have been associated with large groups working in endemic areas or fixed populations (e.g., prisoners) exposed to soil or dust [79]. Three of the largest reported outbreaks occurred as a result of natural events: A dust storm in the San Joaquin Valley in 1977 [80], the Northridge earthquake of 1994 [81], and the 1998–2001 Arizona drought [82].
Risk factors for severe or disseminated disease include Filipino or African ethnicity, concomitant infection with human immunodeficiency virus (HIV), chemical immunosuppression (steroids, immunomodulators, chemotherapy, organ transplantation), diabetes mellitus, pregnancy, and cardiovascular disease [3,7,30,83–86]. In several series, persons of African-American descent were at an 8–11 times greater risk of developing disseminated disease [78,86–90]. Patients who become immunosuppressed can have reactivation of latent infection [91]. The mortality rate among patients with coccidioidomycosis is highest among men, persons >65 years, Hispanics, Native Americans, and residents of California or Arizona (likely indicating the burden of the inoculum), particularly among those who have HIV or are otherwise immunosuppressed [77,86].
The morbidity associated with infection can be substantial. In endemic areas, almost 75% of cases reported missing a median of two weeks of work or a median of nine days of school because of illness, and 40% required hospitalization [92]. Calculated yearly inpatient costs of coccidioidomycosis were approximately $30,000 per patient in endemic areas; the cost of patients with disease requiring surgery has not been calculated.
Laboratory Testing
Because of the non-specific clinical symptoms and radiographic findings, laboratory confirmation often is required to secure a diagnosis of coccidioidomycosis. Serologic tests, culture, and microscopy are the most common methods of laboratory diagnosis [93]. Enzyme immunoassay (EIA), one of the more commonly used serologic tests, can provide fast, inexpensive, and qualitative evidence of infection but may lack sensitivity in early or mild disease or in immunosuppressed hosts [19]. The sensitivity of EIA is approximately 87% in otherwise-healthy infected patients but decreases to 67% in immunosuppressed patients; repeat or confirmatory testing can raise the sensitivity to 95% and 84%, respectively [94]. In cases of an isolated EIA immunoglobulin (Ig) M positive result, serologic positivity should be confirmed with other methods [94]. Immunodiffusion can detect IgG and IgM antibodies and can confirm exposure to Coccidioides spp. with high specificity [6].
Another serologic test commonly utilized is complement fixation (CF), which can be used to assess the severity of disease and for monitoring of disease activity [6]. A CF titer greater than 1:16 is associated with a greater frequency of disseminated disease [6]. Organisms can be cultured from tissue or sputum specimens. However, the risk of this test to laboratory personnel limits its widespread use, as culture is permitted only in Biosafety Level 3 facilities [93]. Finally, microscopy can be used to examine tissue or respiratory secretions for spherules, although the sensitivity of this method is low. Mature spherules containing endospores are pathognomonic of infection.
Polymerase chain reaction (PCR) remains experimental but is promising. The PCR studies of respiratory specimens to date report sensitivities of 100% and specificities of 98.4% [93,95,96]. In fresh tissue, the sensitivity and specificity decrease to 92.9% and 98.1%, respectively [96]. Paraffin-embedded tissue is more challenging, with a reported sensitivity of 73.4% and specificity of 100% [96]. Finally, urinary antigen detection may be useful for diagnosing coccidioidomycosis in severely immunosuppressed patients [97].
Anti-Fungal Treatment
Patients with localized acute isolated pulmonary infections without risk factors for dissemination can be treated conservatively, with follow-up imaging to document resolution of infection [11]. Anti-fungal therapy regimens for various manifestations of disease have been described in depth by the Infectious Diseases Society of America, and readers interested in the nuances of anti-fungal therapy are directed to their publication [11]. When indicated, anti-fungal therapy relies on the use of azole antifungals or amphotericin B, either alone or in combination, for long times, often a year or more [11]. In patients at high risk of disseminated disease or with severe underlying immunosuppression, lifelong therapy may be required. Limited human data are available to support the use of caspofungin or posaconazole for coccidioidomycosis [6,11].
Typically, there are five broad indications for surgical intervention in patients with coccidioidomycosis: Tissue diagnosis in patients at risk for other pathology, perforation, bleeding, impingement on critical organs, and failure to resolve with medical management (Table 1). Irrespective of the indication, surgical therapy should be delivered in close collaboration with other providers, including pulmonologists and infectious disease physicians, in order to optimize anti-fungal regimens and ensure long-term compliance with therapy. Providers who are unfamiliar with coccidioidomycosis are encouraged to contact surgeons in endemic regions who are familiar with the infection while formulating a treatment plan tailored to specific patient situations.
Conclusions
Coccidioidomycosis is a multi-system illness caused by endemic fungi. The non-specific signs and symptoms of early infection and the protean manifestations of disseminated disease can make the diagnosis challenging, particularly in patients who have traveled to or moved away from endemic areas. Although most disease is self-limited, persistent pulmonary and disseminated disease can be amenable to surgical intervention in some cases. Any operation should be performed in close collaboration with infectious disease specialists to ensure an appropriate trial of anti-fungal therapy pre-operatively and optimize the anti-fungal regimen post-operatively. Finally, surgery can palliate debilitating symptoms that would otherwise be untreatable.
Footnotes
Author Disclosure Statement
No conflicts of interest are reported for any author.