
Abstract
Abstract
Background:
The Gatti score is a weighted scoring system based on risk factors for deep sternal wound infection (DSWI) that was created in an Italian center to predict DSWI risk after bilateral internal thoracic artery (BITA) grafting. No external evaluation based on validation samples derived from other surgical centers has been performed. The aim of this study is to perform this validation.
Patients and Methods:
During 2015, BITA grafts were used as skeletonized conduits in all 255 consecutive patients with multi-vessel coronary disease who underwent isolated coronary bypass surgery at the Department of Thoracic and Cardio-Vascular Surgery, University Hospital Jean Minjoz, Besançon, France. Baseline characteristics, operative data, and immediate outcomes of every patient were collected prospectively. A DSWI risk score was assigned to each patient pre-operatively. The discrimination power of both models, pre-operative and combined, of the Gatti score was assessed with the calculation of the area under the receiver operating characteristic curve.
Results:
Fourteen (5.5%) patients had DSWI. Major differences both as the baseline characteristics of patients and surgical techniques were found between this series and the original series from which the Gatti score was derived. The area under the receiver operating characteristic curve was 0.78 (95% confidence interval: 0.64–0.92) for the pre-operative model and 0.84 (95% confidence interval: 0.69–0.98) for the combined model.
Conclusions:
The Gatti score has proven to be effective even in a cohort of French patients despite major differences from the original Italian series. Multi-center validation studies must be performed before introducing the score into clinical practice
D
To date, there has been no evaluation of the precision of performance estimates of the Gatti score in independent validation samples derived from other surgical centers. The aim of the present study was to perform this second external validation by testing the score in a new prospective series of CABG patients operated on in a French cardiac surgical unit with great experience in the use of BITA grafting (the French series).
Patients and Methods
Between January 1 and December 31, 2015, 255 consecutive patients with multi-vessel coronary disease underwent isolated CABG at the Department of Thoracic and Cardio-Vascular Surgery of the University Hospital Jean Minjoz of Besançon, France. Bilateral internal thoracic artery grafts alone were used to perform myocardial re-vascularization in all patients (Table 1).
Gatti et al. [5].
Defined as basal serum glucose >200 mg/dL at three consecutive measurements.
Defined as glycated hemoglobin ≥6.5%.
Nashef et al. [9].
The creatinine clearance rate, calculated according to the Cockcroft-Gault formula, was used for approximating the GFR.
BMI = body mass index; EuroSCORE = European System for Cardiac Operative Risk Evaluation; GFR = glomerular filtration rate; LVEF = left ventricular ejection fraction.
Unless otherwise stated, definitions of pre-operative clinical variables were those used for the European System for Cardiac Operative Risk Evaluation II (EuroSCORE II) [9]. Poor pre-operative glycemic control was defined as glycated hemoglobin 6.5% or greater [8]. The risk profile for each patient was calculated according to EuroSCORE II [9]. Post-operative myocardial infarction was defined according to the definition criteria for type V myocardial infarction by Moussa et al. [10]. Acute kidney injury was defined according to the Kidney Disease: Improving Global Outcomes (KIDGO) criteria [11]. The U.S. Centers for Disease Control and Prevention classification of the surgical site infections was adopted to define sternal wound infection [12]. For the purposes of this study, deep incisional infection and mediastinitis were considered to be DSWI.
All peri-operative data were recorded prospectively for every patient in a computerized data registry. For each patient, the score of the pre-operative and the combined model of the Gatti score [5] were calculated immediately before operation and recorded in a dedicated file; the score of the combined model was completed at hospital discharge. Post-discharge surveillance of the surgical sites was performed in a dedicated surgical outpatient unit. All patients with a surgical site complication were referred to this outpatient unit, at any time after hospital discharge. Approval to conduct the study was obtained from the Hospital Ethics Committee; the need for patients to provide their individual written consent was waived.
Surgery
Surgery was carried out via a median sternotomy either with cardiopulmonary bypass, with or without cross-clamping the aorta or off-pump technique. When a period of myocardial ischemia was used, myocardial protection was usually achieved with multi-dose tepid (28°C) blood cardioplegia delivered in antegrade mode (Tables 2 and 3) [13–17].
Gatti et al. [5].
Calculated in the patients who underwent aortic cross-clamping.
Calculated in the patients who underwent CPB.
BITA = bilateral internal thoracic artery; CPB = cardiopulmonary bypass.
Gatti et al. [5].
Zingone et al. [13].
Erdinc et al. [14].
Neither platelet gel nor topical antibiotics were used.
Sutherland et al. [15].
Furnary et al. [16].
Gatti et al. [17].
BITA = bilateral internal thoracic artery; CPB = cardiopulmonary bypass; EAS = epiaortic ultrasonography scan; ICU = intensive care unit; ITA = internal thoracic artery
Statistical methods
The data were expressed as the number of patients with the percentage in brackets, or the mean ± standard deviation. Pre-operative clinical patient characteristics, operative data, and post-operative complications were compared using the χ2 or the Fisher exact test for dichotomous variables and the Student t test or the Mann-Whitney U test for continuous variables, as appropriate. For both models of the Gatti score, the goodness-of-fit was assessed with the Hosmer-Lemeshow test; the discrimination power was assessed with the receiver operating characteristic (ROC) curve and the calculation of the area under the receiver operating characteristic curve (AUCROC). According to arbitrary guidelines, the accuracy of prediction was defined as low (AUCROC: 0.5–0.7), moderate (AUC: 0.7–0.9), and high (AUCROC: 0.9–1) [18]. The pre-operative and the combined model were compared using the method of DeLong et al. [19]. A p value <0.05 was considered significant. For both models of the Gatti score, the Youden index was measured and a list of threshold values (criteria) corresponding with the coordinates of the ROC curves, with associated sensitivity and specificity was created. For equal sensitivity/specificity the threshold values with the highest specificity/sensibility were given. Finally, the data of the sample were used to create a large set (1,000 iterations) of new bootstrap samples, and the bias-corrected and accelerated bootstrap adjusted for possible bias and skewness in the bootstrap distribution [20]. The expected risk of DSWI according to the Gatti score (low: <10%; moderate: 10%–20%; high: >20%) was compared with the actual rate of DSWI in the French series. Analyses were performed with the SPSS program for Windows, version 13.0 (SPSS, Inc., Chicago, IL).
Results
The French series: Immediate outcomes
There were no hospital deaths. The peri-operative complications that occurred are listed in Table 4. Fourteen (5.5%) patients had DSWI.
Most myocardial infarctions were defined only according to cardiac troponin I elevation to ≥70 × the local laboratory ULN (Moussa et al. [10]).
Acute Kidney Injury Work Group: Kidney Disease: Improving Global Outcomes (KDIGO) [11].
Mangram et al. [12].
DSWI = deep sternal wound infection; RBCs = packed red blood cells; SSWI = superficial sternal wound infection; ULN = upper limits of normal.
The original versus the French series
During the corresponding study periods, the rate of BITA use in the French series was greater than in the original series (100% versus 70.6%; p < 0.0001) [5]. Major differences were found between the original and the French series as the pre-operative characteristics of patients. Overall, the patients' risk profiles were higher in the original series (mean EuroSCORE II: 3.6% ± 5.1% versus 2.6% ± 3%, p = 0.0021; Table 1). In the French series, there was a lower number of coronary anastomoses and both the aortic cross-clamp and cardiopulmonary bypass times were shorter (p < 0.0001). Between the two series, there were also major differences as the rates of use of different surgical techniques and the measures that had been taken to reduce the risk of sternal wound infection (Tables 2 and 3). On the basis of the Gatti score estimates [5], there was no difference as the DSWI risk between the two series of patients (p = 0.64 for the pre-operative model and p = 0.85 for the combined model; Table 4). The actual rates of DSWI in the French and in the original series were 5.5% and 4.4% [5], respectively (p = 0.42).
The French validation of the Gatti score
The corresponding rates of the Gatti score risk factors for DSWI in the original and in the French series are reported in Table 5 [5]. The Gatti score goodness-of-fit was satisfactory both for the pre-operative (p = 0.59) and the combined model (p = 0.82). The AUCROC was 0.78 (95% confidence interval: 0.64–0.92) for the pre-operative model and 0.84 (95% confidence interval: 0.69–0.98) for the combined model (Fig. 1). The Youden index was 0.51 (associated criterion: >148 points) for the pre-operative model and 0.69 (associated criterion: >101 points) for the combined model. The sensibility and the specificity for different threshold values were calculated (Table 6). There was a good correspondence between the expected risk of DSWI according to the Gatti score and the actual rate of DSWI in the French series both for low and high DSWI risk; for middle risk, the Gatti score underestimated the actual risk (Fig. 2).
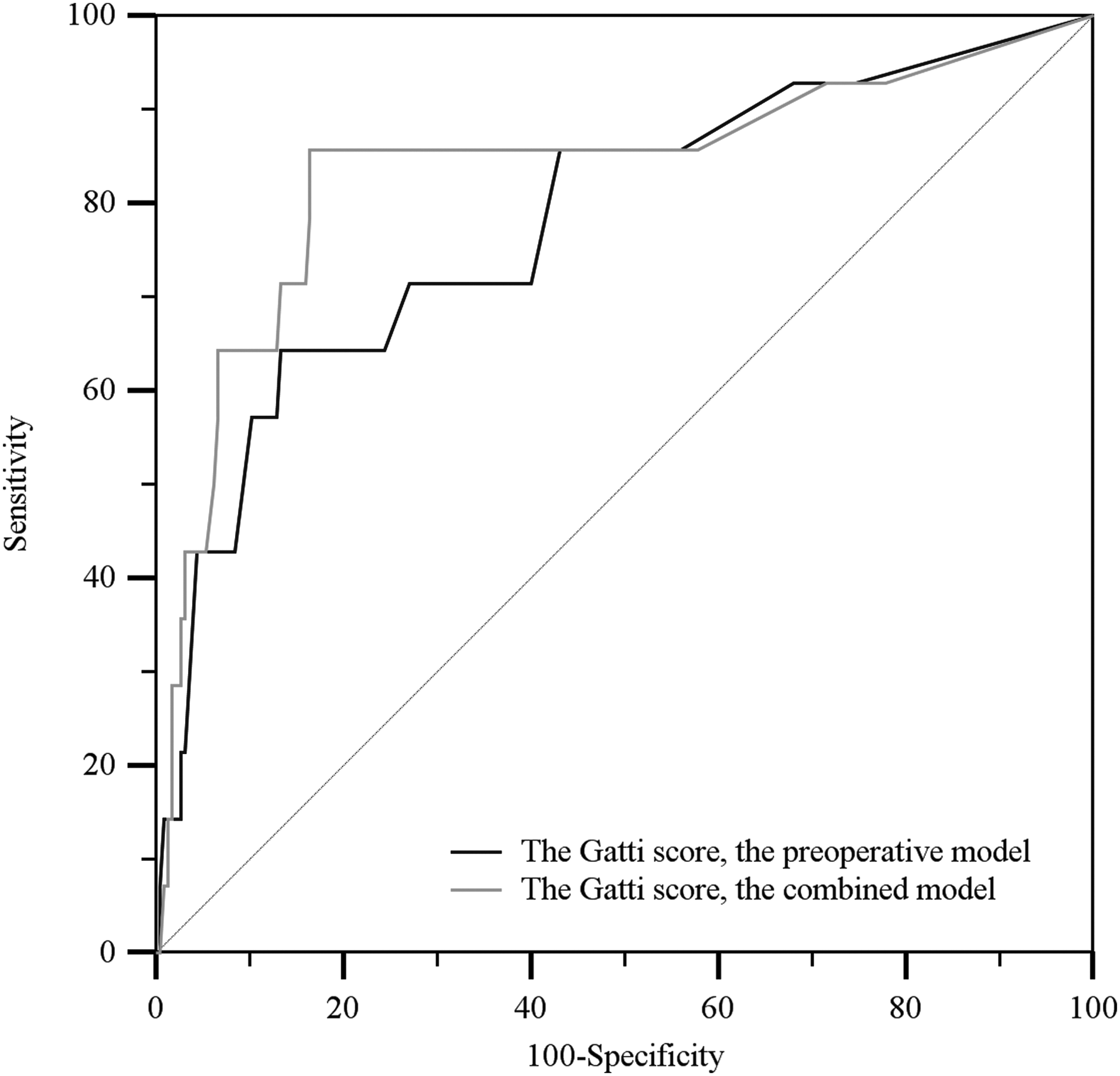
The Gatti score. The pre-operative and the combined model in the French series (AUCROC = 0.78, 95% CI: 0.64–0.92 versus AUCROC = 0.84, 95% CI: 0.69–0.98; p = 0.057). AUC = area under the receiver operating characteristics curve; CI = confidence interval.
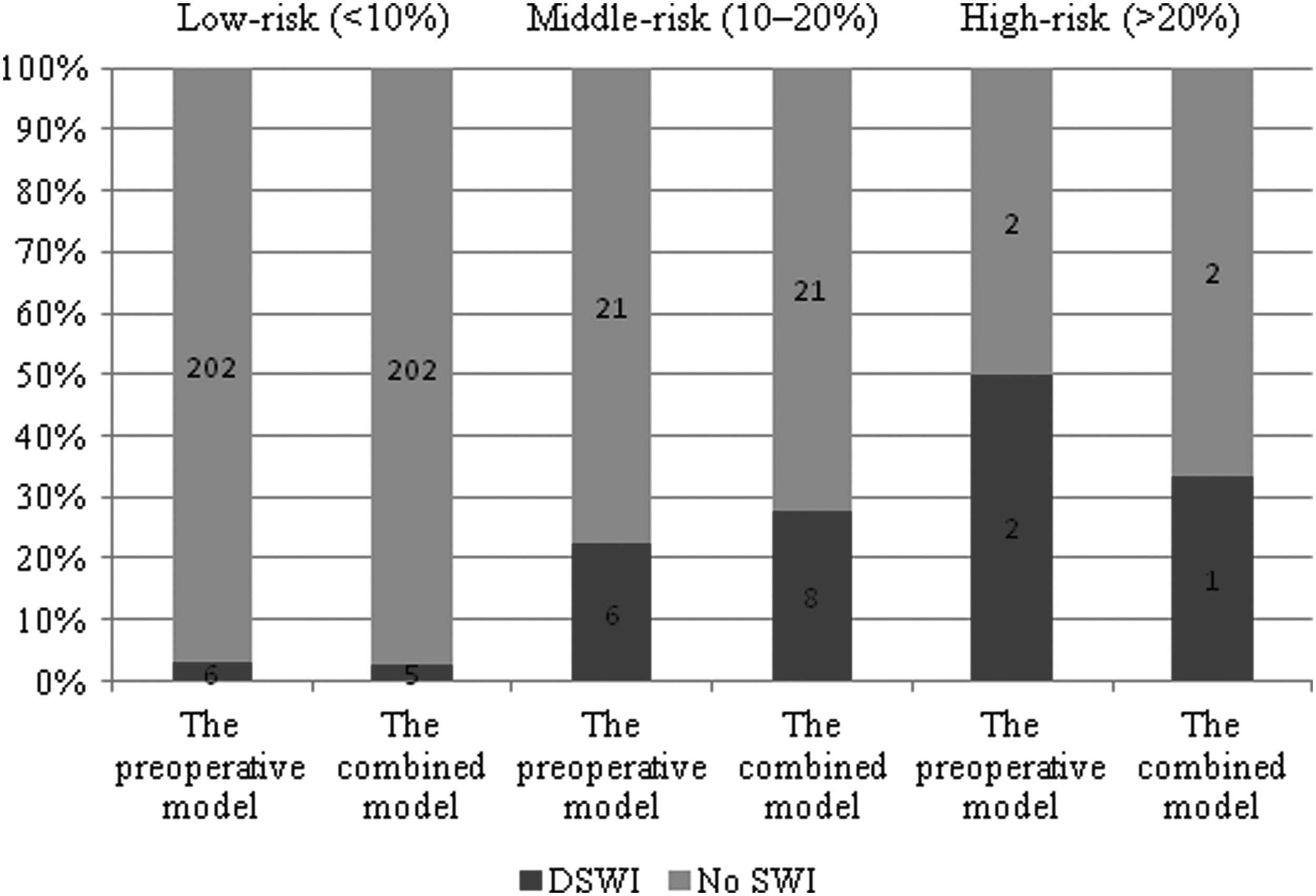
The actual rate of DSWI in the French series and the expected DSWI risk according to the Gatti score. DSWI = deep sternal wound infection; SWI = sternal wound infection.
Gatti et al. [5].
Defined as basal serum glucose >200 mg/dL at three consecutive measurements.
Defined as glycated hemoglobin ≥6.5%.
Moussa et al. [10].
By intra-operative EAS (Zingone et al. [13]).
By intra-operative palpation.
Defined as three consecutive cardiac index measurements <2 L/min/m2 despite adequate pre-load, afterload, and inotropic support or IABP (Gatti et al. [5]).
Defined according to clinical evaluation.
BMI = body mass index; DSWI = deep sternal wound infection; EAS = epiaortic ultrasonography scan; IABP = intra-aortic balloon pumping; RBCs = packed red blood cells.
Efron [20].
CI = confidence interval.
Discussion
Several models have been devised to predict the risk of developing sternal complications after median sternotomy [6,7]. However, the predictive power of these models are low when they are tested in BITA patients [5]. Actually, these predictive models arose from cohorts of patients undergoing various surgical procedures or pre-selected series of CABG patients in which most of the patients have received single internal thoracic artery (and saphenous vein) grafts [6,7].
In 2015, the Gatti score was created specifically to predict DSWI risk after BITA grafting to reduce the rate of DSWI after CABG without giving up too much in terms of long-term survival benefits derived from the use of BITA grafts [1,2,5]. The score has proven to work well even when it has been tested on an independent validation sample of prospectively enrolled patients derived from the institution where it had been created [8]. In the present study, the Gatti score was tested in a prospective series of 255 patients operated on at the Department of Thoracic and Cardio-Vascular Surgery of the University Hospital of Besançon, France.
There were major differences between the original and the French series in terms of baseline characteristics of patients, the surgical techniques that were adopted, operative data, and post-operative complications. Overall, the French patients were older and had more frequent comorbidities (diabetes mellitus, impairment of mobility secondary to neurologic dysfunction, renal failure, and extracardiac arteriopathy) whereas in the original series there was a stronger ischemic heart disease (higher rates of recent myocardial infarction, left main and three-vessel coronary disease, moderate left ventricular dysfunction, critical state, and urgent surgical priority). In the original series, BITA grafts were used (preferably as in situ conduits) to obtain a left-sided myocardial re-vascularization; the off-pump technique was adopted infrequently and only in the presence of a diffusely atherosclerotic ascending aorta [5,13]. In the French series, the BITA grafting alone with Y-graft was used; in the absence of a diffusely atherosclerotic ascending aorta, either the off- or on-pump technique was adopted according to the surgeon's preference. In both series, prophylactic antibiotics were used and special attention was placed on the skin preparation, internal thoracic artery harvesting technique (both internal thoracic arteries were harvested as skeletonized conduits with low-intensity cautery), sternal reconstruction [14,15], and peri-operative management of hyperglycemia in patients with diabetes mellitus [16]. The longer mean aortic cross-clamp and cardiopulmonary bypass times of the original series were partially due to a higher mean number of coronary anastomoses.
In both series, DSWI was a frequent post-operative complication. It was much more frequent than reported in cohorts of patients who have received single ITA (and saphenous vein) grafts. It was more frequent than reported in BITA patients by other authors [1–4]. In our opinion, the high rate of sternal wound infections of the two series was caused by the use of BITA grafting without any pre-operative selection of candidates. Conversely, this proves that no substantial reduction of the DSWI risk can be achieved without performing a pre-operative selection of patients. The Gatti score could be a reasonable way to perform this selection [5]. The expected risk of DSWI according to the Gatti score was the same in both series (for both models of the score) despite there were in the original series higher rates of urgent surgical priority, multiple blood transfusions, and mediastinal re-exploration. In fact, both the prevalence of female gender and the rate of diabetes mellitus on oral hypoglycemic agents were greater in the French series, even though the differences were not quite significant. In addition, among the French patients, there was also a superior rate of poor pre-operative glycemic control with respect to the original series, however, the definition of poor glycemic control that was adopted was not the same in both groups.
The goodness-of-fit and the discrimination power of both models of the Gatti score were satisfactory and there was a good correspondence between the expected DSWI risk (by the Gatti score) and the actual rate of DSWI, at least for the low- and high-risk patients. Despite the major differences between the two series including pre-operative characteristics, surgical techniques, and post-operative complications, the Gatti score has proven to be effective in predicting DSWI after routine BITA grafting also in a French validation sample. This could mean that the score works well even in populations of patients with different rates of comorbidities from other institutions. This hypothesis has to be verified by new larger multi-center studies before introducing the Gatti score into clinical practice.
Footnotes
Author Disclosure Statement
No competing financial interests exist.