
Abstract
Abstract
Background:
Intra-operative surgical site irrigation (lavage) is common practice in surgical procedures in general, with all disciplines advocating some form of irrigation before incision closure. This practice, however, has been neither standardized nor is there compelling evidence that it effectively reduces the risk of surgical site infection (SSI). This narrative review addresses the laboratory and clinical evidence that is available to support the practice of irrigation of the abdominal cavity and superficial/deep incisional tissues, using specific irrigation solutions at the end of an operative procedure to reduce the microbial burden at wound closure.
Methods:
Review of PubMed and OVID for pertinent, scientific, and clinical publications in the English language was performed.
Results:
Incision irrigation was found to afford a three-fold benefit: First, to hydrate the bed; second, to assist in allowing better examination of the area immediately before closure; and finally, by removing superficial and deep incisional contamination and lowering the bioburden, expedite the healing process. The clinical practice of intra-operative peritoneal lavage is highly variable and is dependent solely on surgeon preference. By contrast, intra-operative irrigation after device-related procedures has become a standard of care for the prophylaxis of acute peri-prosthetic infection. The clinical evidence that supports the use of antibiotic irrigation is limited and based on retrospective analysis and few acceptable randomized controlled trials. The results of laboratory and animal studies using aqueous 0.05% chlorhexidine gluconate are favorable, suggesting that further studies are justified to determine its clinical efficacy.
Conclusion:
The adoption of appropriate and standardized intra-operative irrigation practices into peri-operative care bundles, which include other evidence-based strategies (weight-based antimicrobial prophylaxis, antimicrobial sutures, maintenance of normothermia, and glycemic control), offers an inexpensive and effective method to reduce the risk of post-operative SSI and deserves further evaluation.
I
Intra-operative lavage, particularly peritoneal lavage, has been performed during surgical procedures for more than 100 years. The traditional view has been that, after contaminated operation, peritoneal lavage reduces residual bioburden and endotoxin levels in peritoneal fluid and effectively reduces the risk of established bacterial foci by the physiologic debridement of fibrin, blood, bacteria, and other debris within the abdominal cavity [2].
The argument that peritoneal contamination should be diluted by using liters of irrigation fluid was succinctly expressed by Robert E. Condon, former Chairman of Surgery at the Medical College of Wisconsin: “The modern concept of peritoneal lavage views the contaminated peritoneum in the same way as a contaminated dermal wound; copious irrigation is a major component of therapy and involves the use of large volumes of saline (up to 10 L and occasionally more) solution with the objective of diluting and removing all of the contaminated peritoneal contents” [3]. Similarly, fascial and superficial irrigation before skin closure is another common practice, but involving less than 1–2 L of solution. The combination of irrigation and debridement is a hallmark in the management of device-related infections [1,4].
Irrigation affords a three-fold benefit: First, it serves to hydrate the bed; second, to assist in better examination of the area immediately before closure; and finally, removing superficial and deep incisional contamination and lowering the bioburden, to expedite the healing process, and in theory reduce the risk of infection [5,6]. The normal process of healing involves three distinct but interrelated phases: Inflammatory, proliferative, and maturational (or re-modeling). Contamination, bacteria, foreign debris, or necrotic tissues need to be removed before the inflammatory phase because contamination can promote an excessive inflammatory response with delayed or inappropriate angiogenesis, excessive tissue granulation, and increase of the risk of SSI and sepsis. The presence of microbial contamination at closure can also alter collagen synthesis and cause tissue anoxia, which can diminish phagocytic cell function. Therefore, irrigation has a clear potential benefit in facilitating the normal progression of the inflammatory to the proliferative and maturational phases of healing [6].
This narrative review addresses the laboratory and clinical evidence for the practice of irrigation of the abdominal cavity and superficial/deep incisional tissues after surgical procedures, using various irrigation solutions to reduce the microbial burden. The discussion has also considered whether antibiotic or biocide irrigation fluids pose any risk for the development of microbial resistance. All surgical incisions are contaminated at operative closure to some extent, and the determinant of this bioburden progressing to SSI is based on: Microbial numbers, microbial virulence, and the status of host defense [7]. Intra-operative irrigation (lavage) should logically play an adjunctive role in improving patient outcome but does published data support that perspective, or even worsen outcome?
Intraoperative Peritoneal Lavage (IOPL) and Wound Irrigation
The rate of SSI after abdominal surgery ranges from 15%–25% with significant post-operative morbidity and mortality, increased length of stay, and substantial health-care costs [8–11]. The actual clinical practice of IOPL is variable and dependent on surgeon preference. The practice was first performed in 1905 by a gynecologist, who advocated sterile water as a lavage fluid before incision closure [12]. This was followed in 1911 by a general surgeon who discovered that physiologic saline, when used as a lavage fluid, reduced patient death from 100% to 55% [13]. Many surgeons, both in the United Kingdom and the United States, have questioned the wisdom of using lavage fluid within the confines of the peritoneum, because retained fluid could in theory spread contamination within the whole peritoneal cavity [14,15].
The concept of using an antiseptic solution was suggested by Behan et al. [16], who advocated irrigation with an alcohol solution in patients with intra-abdominal infection, reducing mortality rates from 100% to 4%. Antibiotics were considered soon after when Dees [17] proposed the addition of an antibiotic to IOPL. Whereas the use of antibiotics in intra-operative irrigation may be viewed as being intrinsically beneficial, the practice has been controversial because of the potential development of bacterial resistance and a question of whether the antibiotic concentration in the irrigant fluid actually achieves a therapeutic level in the area [18].
In a study involving hospitalized patients, Pissiotis et al [19] reported that after intra-peritoneal administration of kanamycin, serum and urine levels of the drug were detected that were similar after intramuscular injection. The question of whether these levels have a therapeutic benefit is the subject of much debate. Although selective investigations have in some cases documented a clinical benefit of peritoneal lavage, the scientific quality and statistical power of some of these studies is questionable.
A laboratory study conducted in the Surgical Microbiology Research Laboratory at the Medical College of Wisconsin in Milwaukee investigated the role of antibiotic-fluid irrigation in a Sprague-Dawley rat model of fecal peritonitis using the cecal-ligation and puncture technique (CLP). The investigators found that gram negative Enterobacteriaceae rapidly colonized the serosal mesothelium and were the predominant flora harvested 4 h post-CLP (3.8 log10 colony forming units [cfu]/mg tissue). After 8 h, anaerobes, specifically Bacteroides fragilis, represented the predominant microbial population adherent to the serosal mesothelium (5.6 log10 cfu/mg tissue).
At 24 h, the aerobic and anaerobic microbial populations, adherent to the serosal mesothelium surface, were 7.1 and 9.1 log10 cfu/mg tissue, respectively. Extended peritoneal saline lavage (100 mL × 10) was effective in significantly reducing the aerobic and anaerobic populations in the lavage fluid (p < 0.001). The mesothelial microbial populations, however, remained relatively stable over the course of multiple lavages (p > 0.05).
This study clearly documented the recalcitrant nature of mesothelial adherence microbial populations after multiple lavages (total lavage volume was greater than 10 × the intra-operative volume given to human beings). The addition of cefazolin, kanamycin, or metronidazole alone or in combination to the lavage fluid failed to significantly reduce the microbial burden on the serosal mesothelium at 48 h post-lavage (p > 0.05). The study found that after injury (leakage) to rat colon, microbial colonization of the peritoneal mesothelial surface is a rapid, stable event, and the mesothelial adherent microbial populations were resistant to intra-peritoneal lavage with or without antibiotics, therefore suggesting a mechanistic basis for therapeutic failure [20].
In a randomized trial [3], the value of IOPL in the management of peritoneal contamination was investigated. This clinical study was performed in 87 patients who underwent emergency laparotomies for peritonitis. They were randomized to three groups: (1) no IOPL; (2) IOPL with saline; and (3) IOPL with saline plus 2 g chloramphenicol succinate. The mortality rate in groups 1, 2, and 3 was 21%, 21%, and 10%, respectively (p > 0.05). The incidence of SSI was 20%, 17%, and 17%, respectively (p > 0.05). The authors concluded that IOPL with saline or antibiotics did not influence the outcome after laparotomies for peritonitis.
Although intra-operative peritoneal lavage is often performed routinely with the aim of reducing peritoneal contamination, there is little evidence of benefit found in patients undergoing elective liver resection without bile duct resection. Investigators in Japan [21] conducted a clinical trial to analyze the benefit of IOPL after elective liver resection. Patients were randomized to no lavage or peritoneal lavage, which was performed at the end of operation with a primary end point of SSI. No significant difference in the SSI rate was observed between lavage (21.9%) and non-lavage groups (13.4%, p = 0.135) when superficial/deep and organ space SSIs were considered together. Organ/space infections, however, were observed significantly more often in the lavage group (16.7%) than the non-lavage group (7.2%, p < 0.05).
Peritoneal lavage was also identified as an independent risk factor for organ/space infection using multi-variable analysis (relative risk, 2.977; confidence interval [CI], 1.094–8.100; p < 0.05). The findings of this study underscore the historically held concern that IOPL may actually function as a vehicle for disseminating peritoneal contamination and subsequent infection.
A systematic review and meta-analysis [22], conducted according to Cochrane Collaboration criteria, analyzed the existing evidence for the effect of intra-operative surgical site irrigation with topical antibiotics, povidone-iodine (PVP-I) solutions, or saline on the incidence of SSI after open abdominal surgery. There were 41 randomized controlled trials reporting primary data of more than 9000 patients considered. Meta-analysis of the effect of intra-operative irrigation with any solution, compared with no irrigation, revealed a significant benefit in the reduction of SSI rates (odds ratio [OR] = 0.54, 95% CI 0.42; 0.69, p < 0.0001). Subgroup analyses documented that the positive effect of irrigation was strongest after colorectal surgery and that irrigation with antibiotic solutions had an even stronger effect than irrigation with PVP-I or saline.
Although the meta-analysis showed an advantage to the addition of antibiotics in lavage fluid, all of the included trials were flawed by having a considerable risk for bias, however. Mechanistically, it is difficult to understand how the addition of antibiotics to a lavage fluid could provide a significant benefit over saline alone, but as the authors pointed out, “given the many methodological flaws and large heterogeneity of the analyzed trials, the clinical relevance [of this finding] has to be balanced against the risk of impaired wound healing and the potential of antimicrobial resistance.”
The practice of intra-operative irrigation has not been limited to colorectal surgery. Two studies of peritoneal cavity irrigation after cesarean section have questioned its value. In one study [23], investigators conducted a randomized trial to investigate the effect of saline irrigation of the peritoneal cavity after cesarean section on gastrointestinal disturbance and post-operative infectious morbidity. Four-hundred and thirty participants were randomized to irrigation of the abdominal cavity or a non-irrigation control group with similar demographics in each group. The rate of intra-operative nausea and emesis (p ≤ 0.001) and the rate of post-operative nausea and emesis (p ≤ 0.001 and p = 0.018, respectively) were significantly higher in the irrigation group compared with control groups. In addition, irrigation with saline at the time of cesarean section provided no beneficial effect on the incidence of post-operative infectious complications.
In the second study [24], investigators conducted a systematic review and meta-analysis to examine the evidence available for the use of intra-operative saline irrigation at cesarean section. The authors found, after analyzing three randomized controlled trials involving 862 females, that there was no statistically significant difference in the SSI rate between patients treated with intra-abdominal saline irrigation compared with control groups (relative risk [RR] = 0.51, 95% CI 0.09–2.73). They concluded that routine use of saline irrigation in the abdominal cavity is not warranted.
In general surgical procedures, the use of antimicrobial solutions for irrigation after appendectomy is controversial. Numerous antiseptic and antibiotic solutions have been suggested for use as irrigation fluids. In a retrospective analysis of 1063 appendectomies [25], investigators sought to determine whether there was a difference in the SSI rate after surgical site lavage with physiologic saline (0.9%), antiseptic solution (Dakin, 0.25%), or an antibiotic solution (imipenem 1 mg/mL).
For saline lavage (n = 661), there was an SSI rate of 7.3% (48/661) and an abdominal abscess rate of 4.2% (28/661). For Dakin solution (n = 208), there was an SSI rate of 15.9% (33/208) and an abdominal abscess rate of 9.1% (19/208). Imipenem (n = 194) irrigation had a SSI rate of 0.5% (1/194) and an abdominal abscess rate of 0.5% (1/194). The authors concluded that abdominal irrigation using the antibiotic solution (imipenem 1 mg/mL) was superior to physiologic saline and Dakin solution. It is important to note that the decision on choice of antibiotic prophylaxis, type of operation (open vs. laparoscopic), irrigation type, irrigation fluid volume, and method of incision closure was based on selective surgeon preference and was not standardized, suggesting a large possible bias with confounding variables.
Intra-operative Irrigation in the Presence of a Biomedical Device: Is There a Role for Antibiotic Irrigation?
Intra-operative irrigation during device-related procedures has become the standard of care after device insertion as well as for the management of acute peri-prosthetic infection [26]. Several studies have explored the addition of antibiotic agents to lavage fluid to reduce the risk of SSI. In a single physician practice [27], the efficacy of antibiotic irrigation for the prevention of early SSI after total joint surgical procedures was evaluated retrospectively in 2293 arthroplasties (1990 patients) between January 2004 and December 2013. The mean follow-up time was 73 months (20–139).
The intra-operative protocol called for an irrigation solution of physiologic saline with vancomycin 1000 mg/L and polymyxin 250,000 units/L, delivered at the rate of 2 L/h. All patients received a cephalosporin (2 g) intravenously before surgery if they were not allergic to penicillin. Those who were allergic to penicillin received vancomycin (2 g IV). A further dose of the antibiotic agent was given 3 h later if the operation was still in progress. No patient was re-admitted for primary infection or additiona antibiotic treatment. The use of antibiotic irrigation during arthroplasty surgery was viewed as being highly effective for the prevention of SSI.
In another retrospective review of 110 posterior lumbar fusions for trauma [28], a rate of infection of 13% in patients who underwent saline irrigation was documented, whereas in patients who had received vancomycin irrigation, no infections were observed during a 2-year follow-up period. Neither of these studies, however, can be viewed as high quality, and the author of the latter study acknowledged that the lumbar fusion analysis was retrospective and likely underpowered.
Several studies have since combined the use of vancomycin powder in addition to intra-operative wound irrigation as an SSI risk reduction tactic. In one such study [29], a retrospective analysis, data on 454 patients who had undergone open aorto-femoral or infra-inguinal vascular procedures between 2006 and 2011 was reviewed. One group of patients received pre-operative systemic antibiotic agents alone and the comparator group received intra-operative surgical site application of vancomycin powder plus irrigation. Both groups had similar demographics and operative characteristics.
A small but statistically significant decrease in the 30-day incidence of SSI was found (25.1% vs. 17.2%; p = 0.049) in the vancomycin plus irrigation group. This was related to a decreased rate in superficial SSIs (18.9% vs. 11.5%; p = 0.033); no significant difference was found between the incidence of deep SSIs (6.1% vs. 5.7%; p = 0.69) or overall surgical site dehiscence rates (22.2% vs. 17.7%; p = 0.24). The authors concluded that the addition of intra-operative local vancomycin plus irrigation did not improve the rates of inguinal surgical site dehiscence or deep infections but appeared to have a positive impact on superficial SSIs.
The evidence that suggests there is a benefit to having antibiotic irrigation as an effective risk reduction tactic is based primarily on retrospective analysis. To be effective, an antibiotic agent must have a sustained exposure to a bacterial cell, which is measured in several minutes rather than seconds. In most irrigation techniques, the fluid is flushed on or within the surgical site but is then rapidly dissipated or evacuated using suction. Further, there have been documented cases of severe anaphylaxis after exposure to antibiotic irrigation fluids.
In three reported cases [30], bacitracin irrigation, at a concentration of 50,000 units per 10 mL, was applied directly to a pacemaker pocket. In each case the patient experienced diffuse erythema, hypotension, and a decreased pulse within 8–15 minutes of bacitracin administration. Two of the patients lost consciousness, and erythema or a rash developed in all three patients. Development of hypotension within 15 minutes of bacitracin administration was the first sign of an adverse reaction, as in other published reports of anaphylactic reactions associated with bacitracin irrigation.
Optimizing Antimicrobial Activity within the Surgical Wound: Are Antiseptics the Answer?
Using an antiseptic for intra-operative irrigation is certainly not a new concept and can be traced back to Listerian antiseptic surgical practice. The selection of an appropriate antiseptic agent for intra-operative surgical site irrigation is problematic, however, because of the wide variety of antiseptic agents that are available currently. A classic experimental study [31], published in 1984, offered some insight into the potential agents of choice based on an experimental in vivo wound model using female albino guinea pigs. Surgical site irrigation with saline or noxythiolin at 15 minutes after Staphylococcus aureus contamination failed to reduce either the incidence or degree of infection. The use of benzalkonium chloride and povidone iodine (PVI) to a lesser degree reduced the SSI rate. They were inferior, however, to chlorhexidine gluconate (CHG); this agent eliminated all overt signs of infection. The healing rate of SSI when chlorhexidine was used was no different from control non-infected surgical sites. When irrigation was performed at 45 minutes before surgical site contamination, only chlorhexidine reduced the infection rate (p < 0.001). The authors concluded that the superior activity of CHG in this animal model was a good indication that it would be an effective biocide to prevent staphylococcal SSI, in part because of combined bactericidal activity and persistence within the wound and low tissue toxicity.
These findings, however, while impressive, do not represent a universal consensus. A meta-analysis published in 2010 [32] included 24 randomized controlled trials (totaling 5,004 patients; 2,465 patients with PVI and 2,539 patients without) that compared intra-operative PVI lavage with no PVI in patients who were undergoing surgery and had SSI as the primary outcome. The SSI rate was 8.0% in the PVI group and 13.4% in the control group. The use of intra-operative PVI significantly decreased the SSI rate (RR 0.58, 95% CI 0.40–0.83; p = 0.003). It was concluded that intra-operative PVI lavage is an effective tactic for reducing the rates of SSI.
Validating Aqueous 0.05% CHG for Intra-operative Irrigation
In 2012, the Food and Drug Administration of the United States approved the use of aqueous CHG 0.05% for cleaning and irrigating various wounds [33]. Aqueous CHG is a cationic-chlorinated biguanide with broad-spectrum activity that is effective against gram positive and gram negative bacteria, selective fungi, and disrupts bacterial cell membranes within 20–30 seconds. Unlike PVI, CHG is not inactivated by blood or tissue protein [1,34,36].
In a series of studies conducted (unpublished data) in the Surgical Microbiology Research Laboratory at the Medical College of Wisconsin in Milwaukee, aqueous 0.05% CHG was found to rapidly reduce the microbial burden under in vitro and in vivo conditions. In vitro, time-kill, kinetics studies documented a more than six-log reduction for most health-care–associated pathogens including multiple drug resistant (MDRO) gram positive and gram negative bacteria (Figs. 1 and 2). To assess the impact of 0.05% CHG on in-vitro microbial adherence to synthetic surgical mesh, three MDRO surgical isolates recovered from post-operative SSIs were selected for study: two methicillin-resistant S. aureus (MRSA) (one biofilm +/ one biofilm −) and Escherichia coli (extended spectrum beta-lactamase +). A concentration of 0.05% CHG was effective (more than five-log reduction, p < 0.001) in resolving selective gram positive and gram negative MDR pathogens from the surface of four distinct synthetic mesh segments (Figs. 3 and 4).

Time-kill log-reduction of selective gram positive multi-drug resistant surgical pathogens. CFU = colony-forming units.
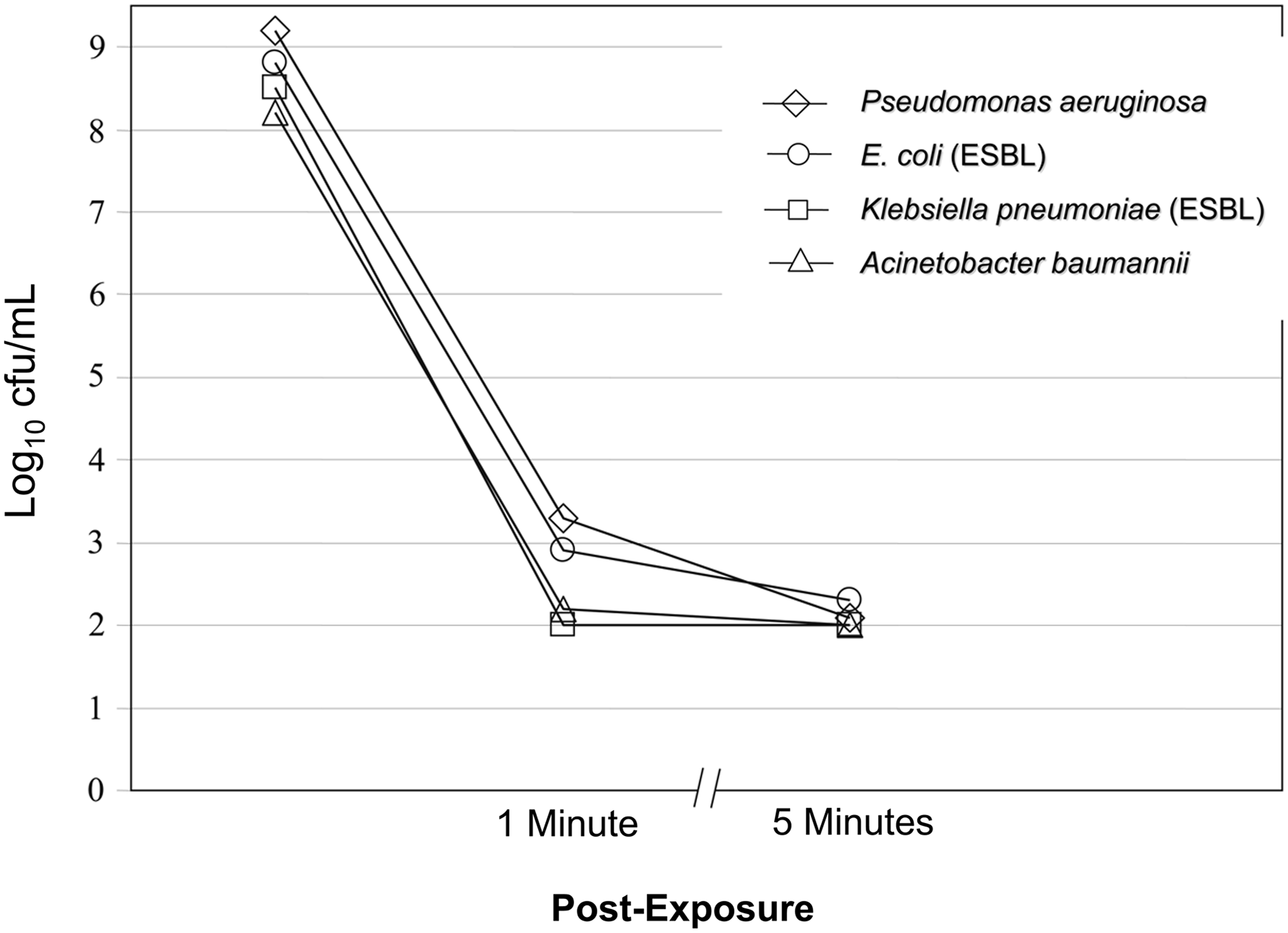
Time kill log-reduction of selective gram negative multi-drug resistant surgical pathogens. CFU = colony-forming units.
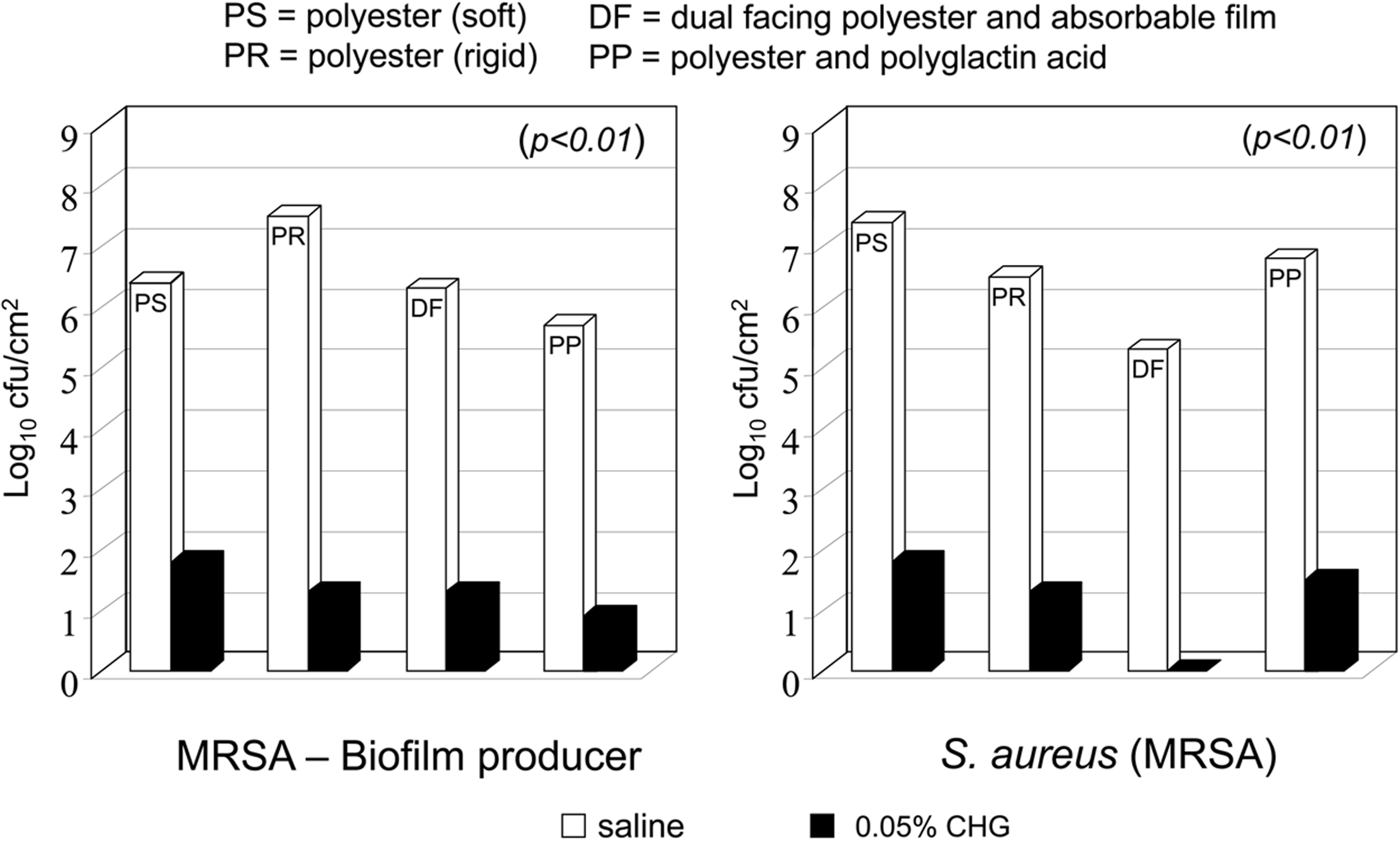
Time-kill log-reduction of two methicillin-resistant Staphylococcus aureus (MRSA) strains (biofilm producer/non-biofilm producing MRSA on four different synthetic mesh following 1-min exposure to 0.05% chlorhexidine gluconate (CHG). CFU = colony-forming units.
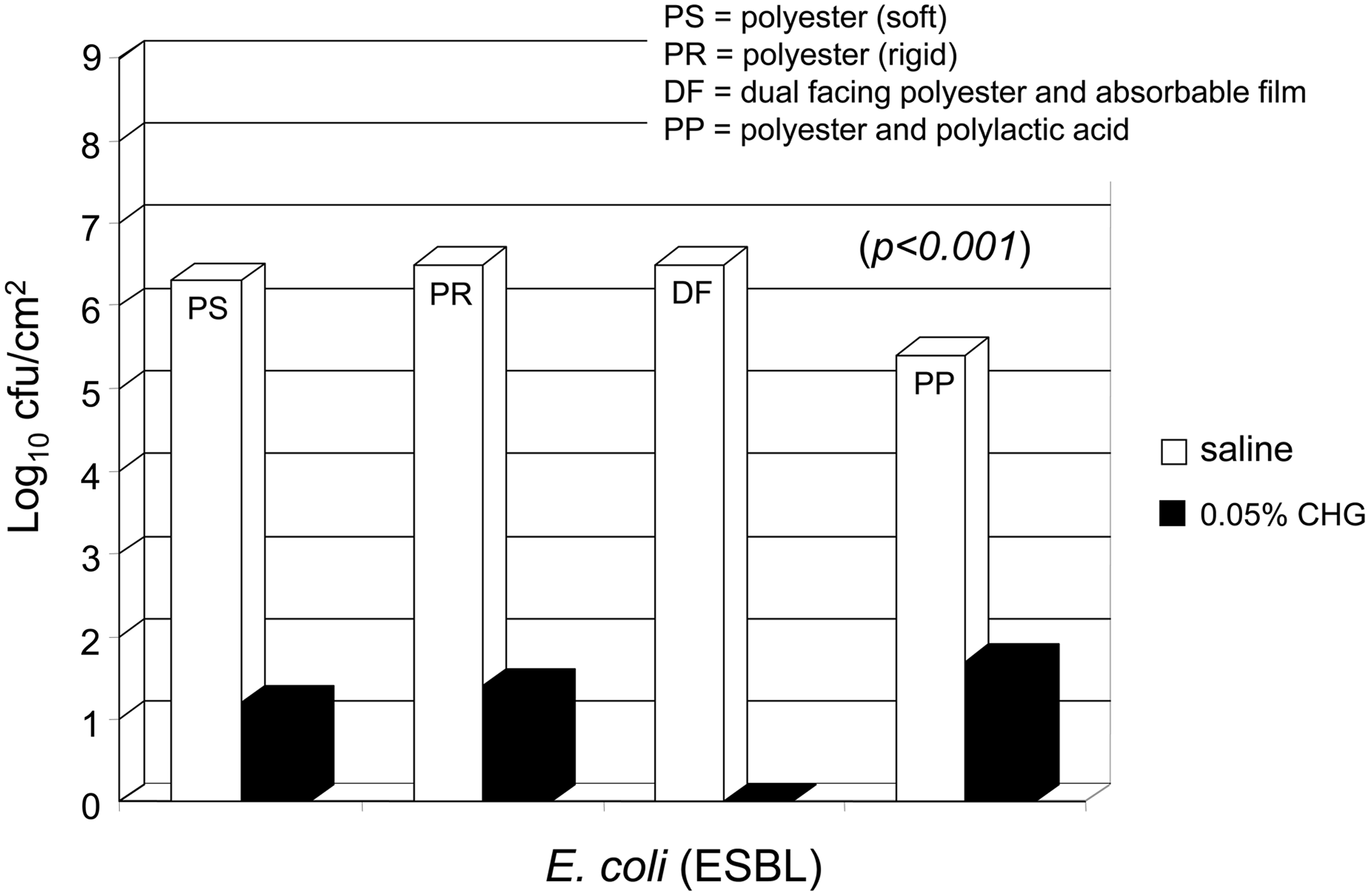
Time-kill log-reduction of Escherichia coli, extended spectrum beta-lactamase (ESBL) drug resistant strain on four different synthetic mesh following 1-minute exposure to 0.05% chlorhexidine gluconate (CHG). CFU = colony-forming units.
In an approved protocol, a pilot study was conducted to compare the effect of intra-operative saline to aqueous 0.05% CHG irrigation on the resolution of MRSA from the surface of implanted (infected) polypropylene surgical mesh. Briefly, a 1 × 2 cm abdominal (ventral midline) defect was created in 16 anesthetized Sprague-Dawley rats followed by aseptic repair with a polypropylene mesh secured with four interrupted sutures. Mesh segments were contaminated (15 minutes) with 3.0 log10 cfu/mL of MRSA recovered from a previous ventral hernia mesh infection. Eight mesh segments were irrigated twice for 60 seconds with physiologic saline (control) while eight mesh segments were irrigated for 60 seconds with aqueous 0.05% CHG followed by a 60 seconds saline rinse (total volume 200 mL for both control and CHG groups). The incision was closed with Prolene and the wound protected with a coflex wrap.
Animals were sacrificed at 7 days, the meshes aseptically removed, sonicated in 5 mL of Trypticase Soy Agar (TSA) for 10 minutes at 10 KHz, and serially plated to tryptone soya agar and incubated for 48 h at 35°C. Microbial recovery was expressed as log10 cfu/cm mesh surface. All eight mesh segments in the saline irrigation group contained a luxurious microbial biofilm (6.3 log10 cfu/cm2 mesh segment), while 1/8 mesh segments in the aqueous 0.05% CHG irrigated group was culture positive (2.6 log10 cfu/cm2 mesh segment, Fig. 5). A concentration of aqueous 0.05% CHG was effective (82.5% reduction, p < 0.001) in reducing the risk of MRSA biofilm-mediated mesh infection in this in-vivo animal model.
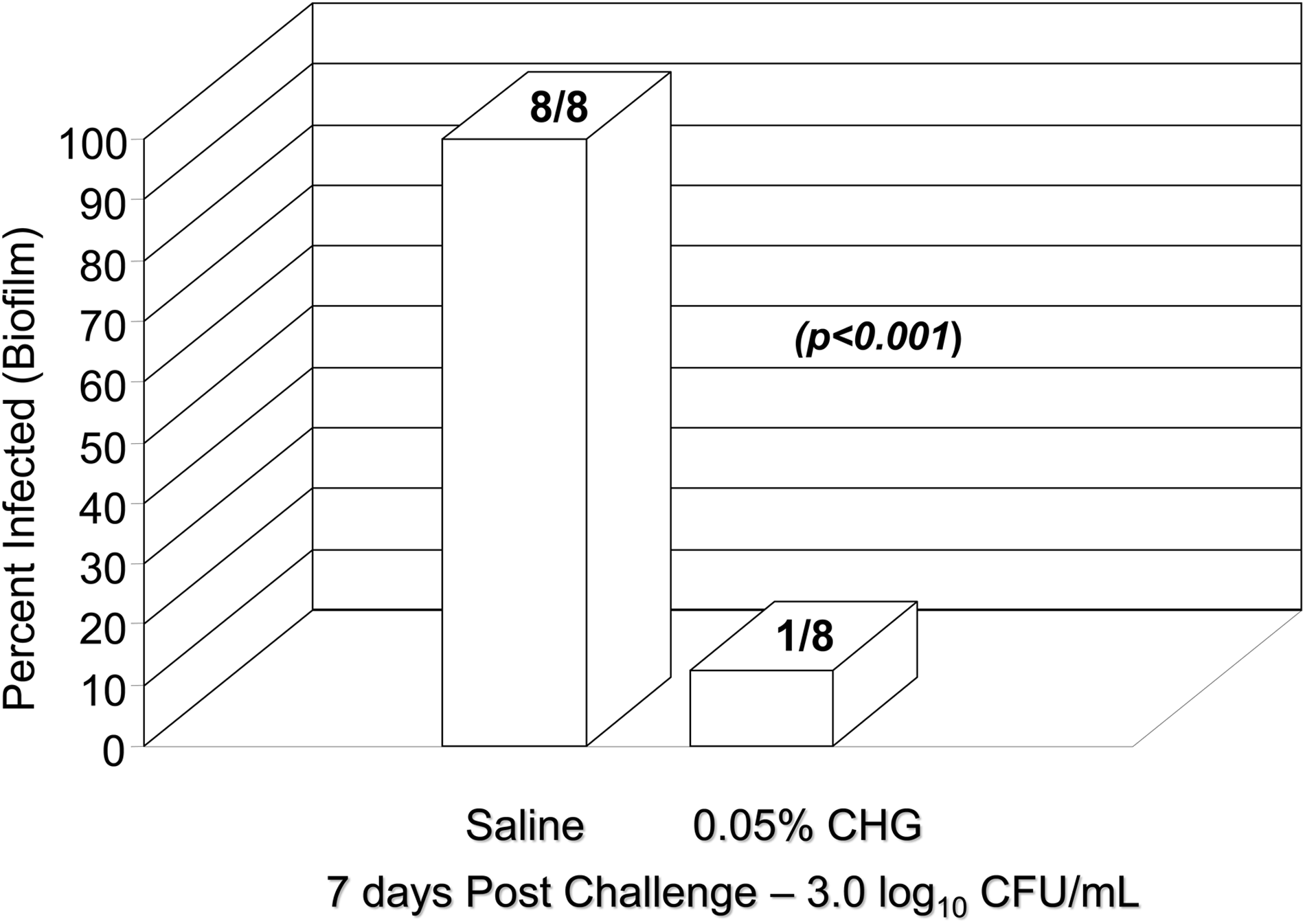
Impact of Intraoperative saline and 0.05% chlorhexidine gluconate (CHG) irrigation on resolution of methicillin-resistant Staphylococcus aureus (MRSA) contaminated polypropylene mesh in Sprague-Dawley animal model at 7 day post-infection (p < 0.001). Total lavage volume, 200 mL, microbial counts expressed as log10 cfu/cm2 surgical mesh, initial MRSA inoculum challenge, 3.0 log10 cfu/mL. CFU = colony-forming units.
Two published studies have suggested a therapeutic benefit can be gained from the use of aqueous 0.05% CHG as an intra-abdominal lavage fluid. The first study investigated closed postoperative peritoneal lavage (CPPL) with chlorhexidine gluconate as a tactic for reducing the number of intraperitoneal bacteria and improving the outcome of intra-abdominal infection. Intra-abdominal infection was produced in mice by cecal ligation and puncture (CLP) technique (CLP). After 16 to 18 hours, the animals underwent re-laparotomy with placement of an intra-abdominal catheter for CPPL. In the first experiment animals were randomly divided into 4 groups: no lavage (control), CPPL with chlorhexidine, CPPL with cefoxitin, and CPPL with lactated Ringer solution (LR). Lavage was continued intermittently every 8 hours for 24 hours. All animals received systemic cefoxitin every 8 hours for 7 days. Mortality was recorded every 8 hours for 10 days. In the second experiment, animals were divided into 3 groups: no lavage (control), CPPL with chlorhexidine, and CPPL with LR. Lavage was continued intermittently every 8 hours for 24 hours. The animals were killed 48 hours after reoperation. Bacterial counts from peritoneal fluid and biopsy specimens, as well as peritoneal white blood cell counts, were measured before and after lavage. Closed postoperative peritoneal lavage with CHG reduced mortality from 71% in the control group to 37% (p = 0.003). There was no survival benefit in either the CPPL with cefoxitin (91% mortality, p = 0.14) or CPPL with LR groups (90% mortality, p = 0.17). There was a greater reduction in bacterial counts in the chlorhexidine group compared with control group (p < 0.05). The authors observed a 50% reduction in mortality and a significant reduction in bacterial counts in the CPPL-CHG group compared with control groups. The authors concluded that closed postoperative peritoneal lavage with 0.05% chlorhexidine gluconate might be useful in the multimodal treatment of intra-abdominal infection [37].
The second study [38] was conducted to assess the benefit of using 0.05% CHG at the completion of colon surgery to reduce post-operative intra-abdominal infection. The 180 mice (ICR mice) were randomized to six groups: groups A, B, and C received one-time intra-peritoneal injections of physiologic saline, aqueous CHG 0.05%, and aqueous CHG 0.025%, respectively; groups D, E, and F all underwent CLP, then partial cecectomy and peritoneal lavage with physiologic saline alone, aqueous CHG 0.05% followed by physiologic saline, and CHG 0.025% followed by physiologic saline, respectively.
Animals were sacrificed and examined at necropsy for occurrence of intra-abdominal abscesses or adhesions. Postoperative intra-abdominal abscesses developed in 48 mice (26.7%). Group E (aqueous CHG 0.05%) mice had a significantly lower incidence of post-operative intra-abdominal abscesses compared with that of group D (saline lavage) mice (p = 0.011). The use of aqueous CHG 0.05% peritoneal lavage after partial colectomy (cecectomy) resulted in reduced post-operative intra-abdominal infection without significant macroscopic adhesion formation [38]. The results of this animal study using aqueous 0.05% CHG were highly favorable, suggesting that further studies are warranted documenting the efficacy of this innovative intra-operative risk reduction tactic.
Compared with Antibiotic Agents, Does Use of Biocides such as CHG Pose a Risk for the Development of Resistance?
A theoretical risk has been raised that the use of biocides (antiseptic agents), such as CHG, povidone iodine, and triclosan, may increase the emergence of organisms resistant to biocides [34,38,40]. Whereas some bacterial cells can express an intrinsic resistance to selected antiseptic agents, the primary concern among advocates of antibiotic stewardship centers around the possibility that selective biocides may increase the risk of antibiotic resistance, which is then transmitted to other organisms [4].
Extensive experience with current antiseptic agents, however, suggested that the clinical risk appears relatively low [41]. A likely reason why resistance to biocides, cross-resistance with antibiotics, and transmission of resistance has not been recognized in surgical practice relates in part to the multi-factorial action of biocides on microbial cells. Antimicrobial agents such as the beta-lactams, aminoglycosides, quinolones, and other antibiotic agents have a singular mechanism of action (i.e., beta-lactam binding to the penicillin-binding proteins in the bacterial cell membrane), while antiseptic agents such as CHG and triclosan have primary and secondary mechanisms that involve the outer bacterial membrane and other membrane-like structures within the cytoplasm.
Biocidal activity is rapid, often occurring within 30–60 seconds of contact with the bacterial cell; alternatively, antibiotic agents require a longer contact time, often measured in several minutes. It is important, however, that antiseptic agents be used in a prudent manner and at concentrations that exceed the minimal concentration when in contact with the bacterial cell, thereby limiting the potential risk of resistance developing or conferring cross resistance to selective antibiotic agents [42].
The Mechanistic Benefit of Intra-Operative Irrigation—Final Consideration
As discussed earlier, lavage to remove debris and dead tissue has a beneficial impact on post-operative wound healing. Pragmatically, however, irrigation before incision closure probably reduces the risk of not just superficial SSI but also the extension of the infection into deeper tissue planes. A matched case-control study has been conducted to determine risk factors for the development of infection after hip and knee arthroplasty. Multiple logistic regression indicated that a significant risk factor for prosthetic joint infection was the development of a superficial SSI not involving the prosthesis (OR, 35.9; 95% CI, 8.3–154.6) [43].
In a separate analysis of 1181 total knee and 1124 total hip arthroplasties, deep wound infection (DWI) after total knee and total hip replacement was highly correlated with the presence of a superficial SSI (p < 0.0001). The authors projected that 58% of superficial SSIs eventually develop into deep SSIs after prosthetic replacement surgery, and therefore preventing a superficial SSI lowers the probably risk of a DWI developing [44]. Although both of these findings relate specifically to orthopedic practice, it is reasonable to assume that a similar mechanistic process occurs after hernia repair with synthetic mesh or placement of vascular graft prosthesis.
The adoption of an appropriate and standardized intra-operative irrigation tactic along with other evidence-based peri-operative care bundle practices, including weight-based antimicrobial prophylaxis, antimicrobial sutures, maintenance of normothermia, and glycemic control, offers an inexpensive and effective method to reduce the risk of post-operative SSI and deserves further evaluation [45].
Footnotes
Author Disclosure Statement
Dr. Edmiston is currently a member of the Sage Products, Clorox, and IRRIMAX speaker's bureau. Dr. Edmiston is also a consultant to the Wisconsin Division of Public Health. For Dr. Leaper, no competing financial interests exist.