
Abstract
Abstract
Background:
C-reactive protein (CRP) has been assessed to detect organ-space surgical site infection (OSI). Nevertheless, data about peri-operative oxygen debt and surgical stress-elicited biologic markers to explain and allow for the early detection of OSI are lacking. We analyzed immediate post-operative venous lactate, early CRP levels, and intra-operative hemodynamic values on the capacity to predict OSI after elective colorectal operation.
Patients and Methods:
Patients undergoing an elective colorectal surgical procedure with anastomosis between March 2013 and August 2014 were included and assessed prospectively. Post-operative lactate values at L-0, L-6, and L-24 hours, CRP (basal and 48 h), and the percentage of operative time (POT) with systolic blood pressure below 100 mm Hg and heart rate above 90 beats per minute in patients with and without OSI were compared. Binary logistic regression was constructed for L-0 and CRP-48, and receiver-operating characteristic (ROC) was analyzed for sensitivity (S), specificity (Sp), positive (PPV) and negative (NPV) predictive values.
Results:
Patients with OSI (11 of 100) showed higher L-0 and L-24 (3.2 ± 2.5 vs. 1.6 ± 0.8; p = 0.025 and 1.9 ± 1.2 vs. 1.2 ± 0.4 mmol/L; p = 0.025) and CRP-48 (188 ± 80 vs. 74 ± 52 mg/L; p = 0.001). The ROC from logistic regression showed area under the curve of 0.899 (95% confidence interval [CI] 0.805–0.992), S of 72% (95% CI 43.2%–90.5%), Sp of 95% (95% CI 88.6%–98.4%), PPV of 66% (95% CI 38.9%–86.4%) and NPV of 0.96 (95% CI 90%–99%). L-0 was higher in those patients with hypotension during more than 60% of the POT (2.4 ± 2.1 vs. 1.6 ± 0.8; p = 0.038). Patients with OSI had a higher POT with hypotension (50 ± 28% vs. 30 ± 28%; p = 0.032) and tachycardia (18 ± 27% vs. 5 ± 16%; p = 0,024).
Conclusions:
The combination of immediate post-operative lactate and CRP at 48 hours proved to be useful in predicting OSI after elective colorectal operation. Assessment of peri-operative lactate is a potential target for intra-operative goal-oriented management aimed at improving post-operative outcomes.
A
Patients and Methods
Study subjects
Patients aged 18 years and over undergoing elective colorectal surgical procedures with intestinal anastomosis at the Colorectal Surgical Unit (five full-time colorectal surgeons) of the University Hospital of Granollers were prospectively and consecutively included. Mechanical bowel preparation with oral antibiotic agents and intravenous antibiotic prophylaxis (single dose of metronidazole, 1,500 mg and gentamicin, 5 mg/kg, within the 60 min before surgical incision) were used as the main preventive measures of surgical site infection (SSI).
Study design
Demographic, clinical, and biologic data from patients undergoing colorectal surgical procedures were gathered as part of a prospective and observation study. We assessed the capacity of a binary logistic regression model that included venous lactate and post-operative CRP levels in predicting the appearance of organ-space surgical site infection (OSI). Venous lactate was assessed both immediately (L-0), six (L-6), and 24 hours after operation (L-24) and assayed using an enzyme colorimetric test (Cobas Integra® 400, Roche Diagnostics, Indianapolis, IN; LACT2 reactants from Roche Diagnostics). Normal lactate values were defined as 0.7–1 mmol/L. Lactate clearance was also calculated using the following formula:
Lactate levels were determined in venous samples because, in previous studies, its values have been equivalent to arterial ones [5]. The CRP concentration was determined pre-operatively (along with pre-operative laboratory test assessment) and at 48 (CRP-48) hours after operation by immunoturbimetric assay (Cobas Integra 400; reactants Tina-quant CRP N° 1 859, Boehringher Mannheim, Ridgefield, CT). Normal values were defined as less than 5 mg/L. Data from the anesthesiologist's operative notebook, such as the percentage of the overall intra-operative time (POT) with hypotension (systolic blood pressure less than 100 mm Hg) and tachycardia (cardiac frequency more than 90 beats per minute), were recorded to establish the correlation between intra-operative hemodynamic pattern and OSI. Total intra-operative infused volume was also determined.
The American Society of Anesthesiologists (ASA) score, Charlson Comorbidity Index, length of operation, main diagnosis, and surgical access were also evaluated. For patients with colorectal cancer, the Tumor-Nodes-Metastasis (TNM) stage was recorded.
The primary outcome of interest was OSI within 30 days of the operation. The attending surgical team was not blinded either for the research process or for the gathering of biologic data. Post-operative infections were recorded in the manner defined by the US Centers for Disease Control and Prevention. The research team recorded the day of OSI diagnosis and, eventually, the day of re-operation. Prospective biologic data collection ended when treatment of the post-operative complication was initiated or when the patient was discharged after an uneventful course.
Sample size calculation
Sample size was calculated with a power of 0.8 and a type I error rate of 0.05 (two tail distribution). Given an expected OSI rate of 8%–10%, the differences between OSI and non-OSI groups regarding the immediately post-operative venous lactate (L-0) value would be 0.5 times the standard deviation (SD) of the L-0 determinations (assuming a standard deviation of 1.7). The study had a minimum overall sample of 91 patients.
Data analysis
Data were summarized as a mean ± SD or 95% confidence interval (CI). Comparison of means was performed using the Student t-test or non-parametric analysis, where appropriate. Contingency tables and chi-square and Fisher tests were used for the analysis of qualitative variables. A binary logistic regression model was constructed using the best lactate and the CRP value at the post-operative 48 hours predictor time point (L-0 and CRP-48). The collinearity of included independent variables was ruled out by performing linear regression analysis. The OSI predictive capacity of this model was assessed by R2 Nagelkerke and goodness of fit by Hosmer-Lemeshow test. A logistic regression equation was derived as follows:
Receiver operating characteristic (ROC) analysis was performed using logistic model-derived probabilities, defining the optimal cutoff from the highest sensitivity/1-specificity value. Contingency tables were constructed to obtain sensitivity (S), specificity (Sp), and positive (PPV) and negative (NPV) predictive values. Statistical analysis was performed using SPSS statistical package v21 (IBM Corp. Released 2012. IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp).
Results
Demographic data
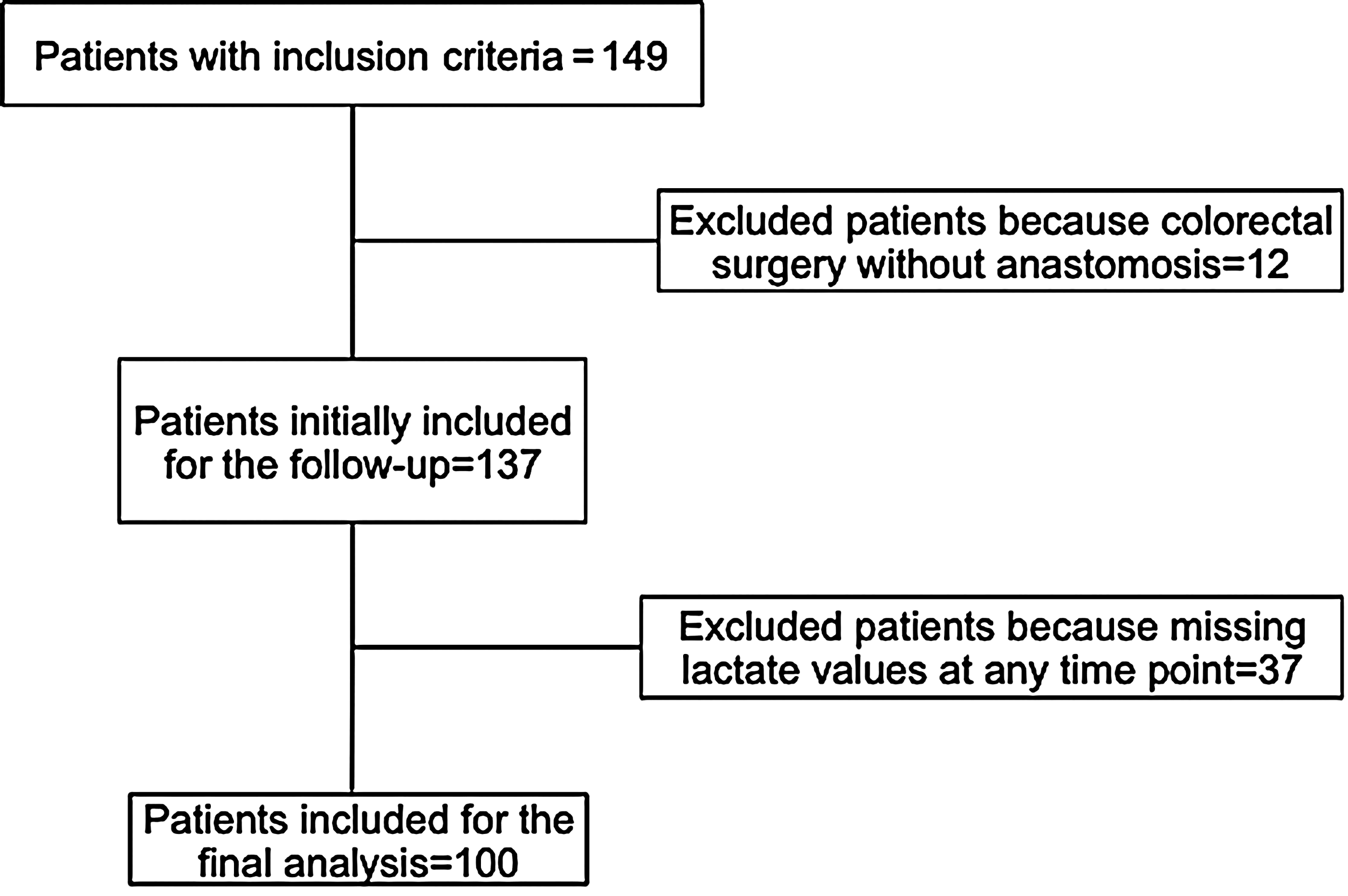
Figure 1 shows the flowchart for the final population of the study. Non-statistical differences regarding the rate of OSI were found when comparing excluded and included patients for the final analysis (5% vs. 11% of OSI, respectively; p = 0.42). The main diagnosis was colorectal cancer in 94 patients, with the remaining six patients being operated on for a benign condition (Table 1).
Totally included and excluded patients.
BMI = body mass index; ASA = American Society of Anesthesiologists; NNIS = National Nosocomial Infections Surveillance.
TNM (Tumor, Node, Metastasis) stage was assessed only in 94 patients operated on for colorectal cancer (six patients operated on for benign condition). In four patients, TNM was not possible to be evaluated; N was not computable because of insufficient number of nodes in the surgical specimen.
Post-operative complications
A total of 50 post-operative complications were recorded in 40 patients (Table 2). Eleven of 100 patients presented OSI that was diagnosed between the second and the 13th post-operative day. Seven patients with OSI underwent re-operation, and four were treated conservatively. Comparative data about complicated and non-complicated patients are represented in Table 3.
Other complications included: three ischemic heart diseases; one cardiac arrythmia; one stroke; one hematoma of surgical wound.
OSI = organ-space surgical site infection; BMI = body mass index; ASA = American Society of Anesthesiologists.
Values are mean ± standard deviation.
Analysis of peri-operative venous lactate
Venous lactate levels at time points L-0 and L-24 were significantly higher in patients with OSI. Nevertheless, lactate clearance from L-0 to L-6 was significantly higher in patients with OSI (44.2% ± 96.5% vs. −9.6% ± 40.2% in non-OSI and OSI groups, respectively; p = 0.013). Further, the percentage of patients with L-0 ≥ 2.5 mmol/L was higher in those with OSI (Table 4). Taking into account L-0 levels, we found no significant differences in the total intra-operative Ringer lactate infusion (1618 ± 760 vs. 1815 ± 1297 mL in L-0 < 2.5 and ≥2.5 mmol/L, respectively; p = 0.874). The area under the curve (AUC) values and the predictive capacity of OSI of L-0 are shown in Table 5.
Values are means ± standard deviation or counts as %. L-preoperative = lactate levels before surgery; L-0 = at the end of surgical procedure; L-6 and L-24 = after 6 and 24 hours.
L-0 = lactate at the end of surgery; CRP-48: = C-reactive protein at post-operative 48 hours; AUC = area under the curve; PPV = positive predictive value; NPV = negative predictive value.
Analysis of peri-operative C-reactive protein
Pre-operative CRP was higher, although not significant, in the OSI group (9,7 ± 21.7 vs. 36 ± 65 mg/L; p = 0.110). CRP-48 was significantly higher in patients with OSI (74.3 ± 51.82 vs. 188.8 ± 80 mg/L; p < 0.001). The AUC values and the predictive capacity of OSI of CRP-48 are shown in Table 5.
Predictive capacity of the binary logistic regression model including L-0 and CRP-48
A binary logistic regression model was constructed using the best post-operative lactate value (L-0) and the CRP-48 time point. The model shows that L-0 and CRP-48 significantly increased the odds of OS developing (Table 6). Figure 2 shows the ROC curve from the binary logistic regression, while a contingency table was used to analyze the main predicted values (Table 5).
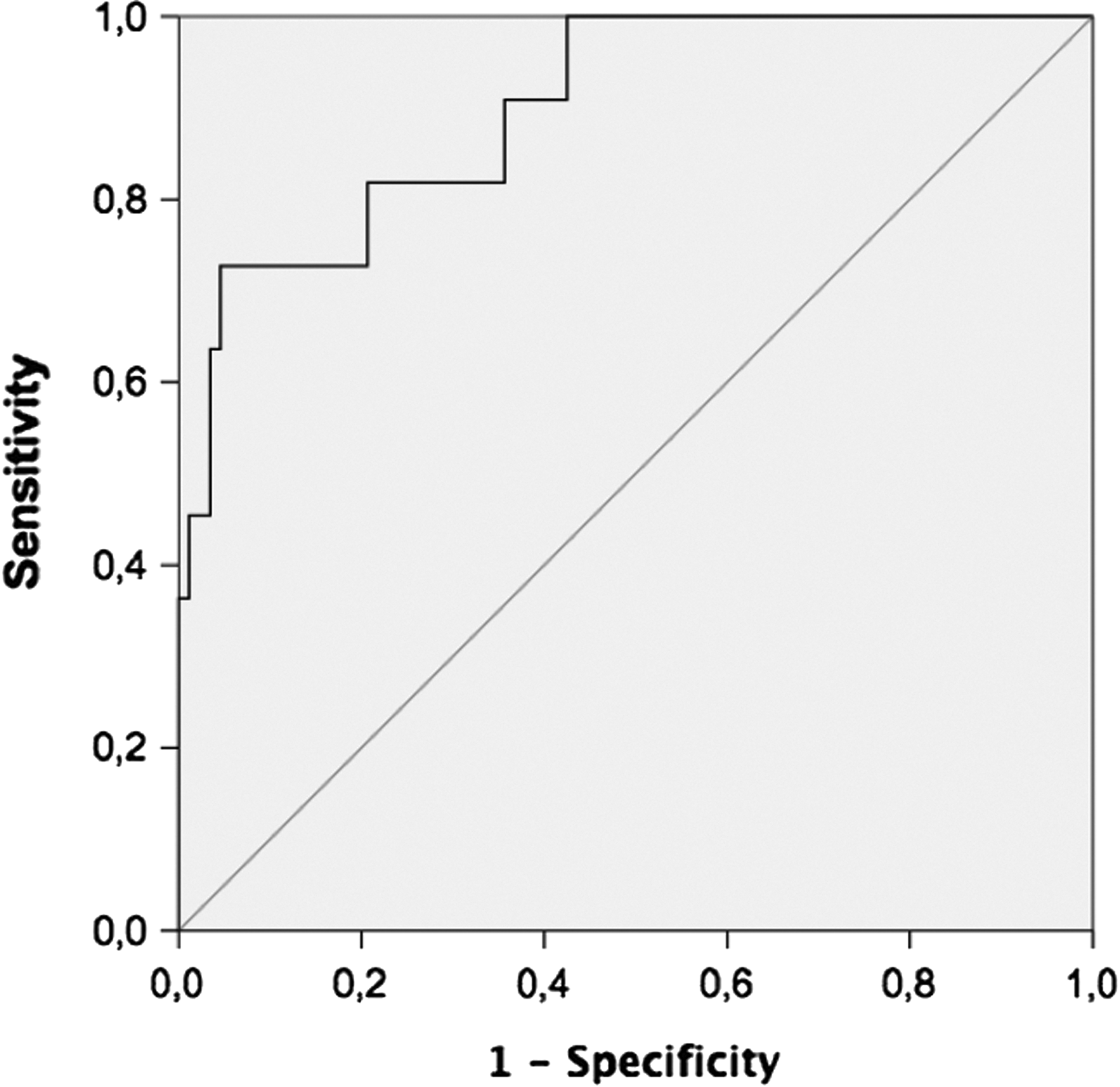
The receiver operating characteristic curve constructed with the saved probabilities derived from the binary logistic regression model.
CI = conficence interval; CRP = C-reactive protein.
Interpretation of the equation of the logistic regression model
An equation derived from the binary logistic regression model was obtained as follows:
Because the best cut-off from the ROC analysis was 0.2613, any probability above this value encompasses the predicted model and values.
Relationship between intra-operative blood pressure and heart rate and OSI
We assessed hemodynamic pattern data by recording the proportion of time that patients presented intra-operative hypotension and tachycardia. In five patients, hemodynamic data were not able to be retrieved. Patients in whom OSI developed presented a significantly higher POT with documented hypotension (50 ± 28% vs. 30 ± 28%; p = 0.032) and tachycardia (18 ± 27% vs. 5 ± 16%; p = 0.024).
Relationship between intra-operative hypotension and immediate post-operative lactate (L-0)
We compared L-0 values for patients with and without intra-operative hypotension. Specifically, we were concerned with the different percentiles of hypotension duration. We did not find significant differences in L-0 values when comparing the overall cohort of patients with and without hypotension, considering a cutoff ≥50% of intra-operative time (1.79 ± 1.33 and 1.6 ± 0.68 mmol/L in patients with and without hypotension, respectively; p = 0.926). We found significant differences, however, when assessing the 75th percentile (cutoff ≥60%) duration of intra-operative hypotension (2.4 ± 2.0 vs. 1.6 ± 0.8 mmol/L in ≥60% and <60%, respectively; p = 0.038). We did not find volume infusion differences in these post-hoc defined groups (1763 ± 637 vs. 1858 ± 211 mL in ≥60% and <60%, respectively; p = 0.761).
Relationship between variables related to immediate lactate production, intra-operative hypotension and the post -operative inflammatory response
Over the full range of patients, those with L-0 of ≥2.5 mmol/L presented significantly higher values at CRP-48 (137 ± 83 vs. 78 ± 58 mg/L; p = < 0.001). The group of patients with ≥60% hypotension developed higher values at CRP-48 (110 ± 61 vs. 78 ± 66 mg/L; p = 0.031).
Discussion
The conundrum of predicting OSI after colorectal surgery by assessing CRP
Because CRP is an acute phase response protein that also may be elicited after a non-infectious injury, the predictive capacity of CRP (immediately measured after a major surgical procedure) is relatively low for OSI detection; as CRP values can also be affected by peri-operative related trauma. Despite such drawbacks, patients with a diagnosis of OSI show significantly higher CRP values at 48 hours [6–8]. Accordingly, at post-operative 48 hours, for a cutoff of 130 mg/L, we found an AUC of 0.888, with a sensitivity of 0.454 and a PPV of 0.5 for OSI prediction.
The relatively modest predictive capacity of the present model is slightly improved from those of previous studies where the AUC for a given 48-hour CRP ranged from 0.560 to 0.766 [6,7,9–11], with these figures also worse compared with 72- or 96-hour post-operative time points (AUC ranging from 0.738 to 0.823 and 0.716 to 0.996 at 72 hours [7,8,12,13] and 96 hours [9,11,14–16], respectively). While later assessment of CRP results in a better predicted capacity, however, the real usefulness of CRP is doubtful, because the diagnosis of OSI may be obvious clinically at later time points [3].
The effect of post-operative immediate venous lactate in a CRP-based early predictive formula of OSI
We have observed that the binary logistic model-derived formula constructed with L-0 and CRP-48 shows improved predictive values when compared with both isolated L-0 and CRP-48 values. Such a formula may potentially be useful not only for predicting a relevant infectious post-operative adverse event but also for classifying at-risk patients who require a higher level of peri-operative management.
Excessive lactate production has been observed after several derangements precluding an oxygen debt and/or as a result of insufficient liver clearance [17]. Although the initial lactate values [18] predict an adverse outcome, sustained hyperlactemia [19] has been correlated with a poor outcome [17] in patients with severe sepsis and trauma [20,21]. Given the mounting evidence in favor of lactate monitoring in different acute diseases, several studies have used lactate as a metabolite biomarker used to classify operative risk after major surgery.
Very high lactate levels (>8 mmol/L) [22] have been correlated with major adverse events after pediatric cardiac surgery [22–26] and liver surgery [27,28] and in high-risk abdominal surgery [29–31]. Compared with liver operations, cutoff levels of lactate when assessing for post-operative complications after gastrointestinal surgery are lower, ranging from 1.5 [29] to 2.5–3 mmol/L [31,32]. These values are within the range of our observations. Although significant differences in peri-operative lactate were found in patients in whom post-operative complications developed, the sensitivity and PPVs of the preferred cutoff were relatively low.
Accordingly, we found modest sensitivity figures (0.640). We hypothesize that while local or systemic hypoperfusion and/or ischemia-reperfusion injury [33] (and elicited lactate production) might induce anastomosis insufficiency, other relevant co-adjuvant factors (mainly technically derived gaps) might also play a part in finally inducing an anastomosis dehiscence. Accordingly, the PPV of venous lactate for post-operative complication is low. A previously healthy patient undergoing a straightforward operation with hemodynamic stability and post-operative low lactate values might therefore circumvent moderate surgical technical deficits (high NPVs).
We found that patients with OSI showed a significantly increased lactate clearance (from L-0 to L-6), compared with patients without complications. Because a decreased lactate clearance has been strongly correlated with patient death from sepsis [19], such findings may be disturbing. Nevertheless, the correlation between lactate clearance and poor outcome has been substantiated in patients with multiple organ failure who are unable to metabolize the produced lactate, signaling an ominous outcome. We would like to reinforce the idea that lactate production is a potential biologic marker of peri-operative stress that might eventually contribute to anastomosis failure in a patient with a preserved capacity to adequately eliminate such lactate excess.
Intra-operative hemodynamic pattern and peri-operative lactate production
We hypothesize that intra-operative oxygen debt-related factors might enhance venous lactate production, signaling serious adverse events. Accordingly, we have shown that patients with more sustained intra-operative hypotension showed a significantly higher rate of post-operative OSI, and that such derangements are associated with higher levels of immediate post-operative lactate. Observational studies have demonstrated a direct relationship between decreased central venous O2 saturation [34] and microvascular flow [35] and post-operative complications after major surgery. Interestingly, such derangements may be overcome via the use of goal-oriented intra-operative hemodynamic management [32,36,37].
The relationship between peri-operative lactate production and the inflammatory response
The CRP levels at 48 hours are significantly higher in patients undergoing colorectal surgical procedures who ultimately present post-operative OSI [6,7,9–11,14,15]. Although this inadequate post-operative inflammatory response may be because of an ongoing infectious complication, a plausible alternative hypothesis is that this excess at CRP-48 might be related to the intra-operative derived stress molecules that are able to elicit the inflammatory response, indicating that the patient is at risk of post-operative complications. Accordingly, we have shown that those patients with higher immediate post-operative lactate levels and those with sustained intra-operative hypotension display a significant increased CRP response.
Previous studies support these observations. Experimental data have demonstrated that hypoxia may induce the production of pro-inflammatory cytokines [38,39]. Further, increased oxidative stress assessed by skin autofluorescence in patients undergoing colorectal procedures is correlated with both IL-6 and CRP production and post-operative complications [40].
Limitations of the present study
Of the patients screen initially, 37 were excluded because of the lack of lactate values at any time point. Although such post hoc exclusion may introduce a relevant bias, we did not find significant differences between included and excluded patients regarding post-operative OSI. Although there are some data supporting the theory that venous lactate levels may overestimate lactate production [41], this observation is far from being universal [27,28], because the correlation between arterial and venous blood lactate has been found to be acceptable [5].
Whether patients infused with Ringer lactate solution might induce increased post-operative venous lactate values is an additional source of potential concern [42]. We did not find significant differences regarding the level of L-0 and the amount of Ringer solution infused, however. Finally, we were not able to dissect the influence of different host- and procedural-related variables that may influence peri-operative lactate and CRP production.
Conclusions
We observed that immediate venous lactate values, in combination with CRP values in a binary logistic based predictive model, improve the predictive capacity of post-operative OSI. Moreover, we found a correlation between lactate production and hemodynamic imbalances, with these derangements able to elicit a post-operative inflammatory response and indicate those patients at risk of post-operative organ-space infection. Goal-directed therapy guided by venous lactate and hemodynamics should be considered in patients undergoing elective colorectal surgery (especially high-risk patients) to minimize the risk of presenting OSI. Under these circumstances, the surgical team may potentially reinforce peri-operative homeostatic goals, with the final objective of both containing an initial anastomosis deficit and closely assessing potential intra-abdominal post-operative infections.
Further cost-benefit analysis of biomarkers-elicited abdominal computed tomography scans (or other potential diagnostic tools to rule out post-operative intra-abdominal infection) made during the early post-operative period are required—both for the current predictive biologic model containing post-operative venous lactate and CRP at 48 hours. Because this predictive formula displays a high negative predictive capacity, those patients deemed not “at risk” may be included in fast track or enhanced recovery surgical programs.
Footnotes
Acknowledgments
The authors thank the members of the colorectal surgery unit of the Hospital General de Granollers, Doctor A. Ibáñez, J. Montero, A. Gaspar, D. Ribé, and R. Hernando, the nurses L. Molero and O. Silva, and the assistant nurses of the Department of Surgery and the Laboratory Department of Hospital Universitari de Granollers for the lactate and C-reactive protein analysis and the Statistical Department of Universitat Internacional de Catalunya for the statistical analysis support.
Author Disclosure Statement
No competing financial interests exist.