
Abstract
Abstract
Background:
The aim of the study was to investigate the concentration and diagnostic significance of soluble triggering receptor expressed on myeloid cells-1 (sTREM-1) in acute abdominal conditions.
Methods:
Plasma specimens were obtained from 68 patients with abdominal sepsis, 60 patients with systemic inflammatory response syndrome (SIRS), and 60 healthy individuals. The sepsis group was divided into the survival and death groups according to the 28-d outcome. Plasma sTREM-1, procalcitonin (PCT), C-reactive protein (CRP), and white blood cell (WBC) count were measured. A receiver operating characteristic curve (ROC) was used to compare the diagnostic values of sTREM-1, PCT, CRP, and WBC count. In addition, the correlation between plasma sTREM-1 and the Acute Physiology and Chronic Health Evaluation (APACHE) II score in the sepsis group was assessed by Spearman correlation analysis.
Results:
The plasma concentration of sTREM-1 in the sepsis group was significantly higher than that in the SIRS and healthy groups (both p < 0.001). Also, the plasma concentration of sTREM-1 in the death group was markedly higher than that in the survival group. The ROC for the diagnosis of sepsis vs. SIRS showed that the area under the curve of sTREM-1 (0.82) was greater than that of PCT (0.77), CRP (0.72), and WBC count (0.70). Additionally, in the sepsis group, the plasma sTREM-1 concentration correlated positively with the APACHE II score (r = 0.41; p < 0.05).
Conclusions:
The plasma concentration of sTREM-1 may be a significantly sensitive and useful indicator for the rapid diagnosis of abdominal sepsis.
S
A recently discovered inflammatory marker is soluble triggering receptor expressed on myeloid cells-1 (sTREM-1), which is shed from the membranes of activated phagocytic cells and can be quantified in human body fluids [6]. STREM-1 plays a considerable role in the innate immune response to invading microorganisms, is selectively expressed in neutrophils and macrophages, and is upregulated by lipopolysaccharide (LPS), bacteria, and fungi [7,8]. Su et al. recently reported that urine sTREM-1 has a high positive predictive value in the early diagnosis of acute nephritis [9]; and previous studies have suggested sTREM-1 as a marker for various infectious diseases, such as septic arthritis, acute nephritis, and pneumonia [10,11]. However, plasma sTREM-1 has not been studied in acute abdominal inflammation.
In this study, we evaluated the value of plasma sTREM-1 in acute abdominal conditions and investigated the diagnostic accuracy of plasma sTREM-1 in patients with abdominal sepsis.
Patients and Methods
Patients
The study was performed in the Department of Gastrointestinal Surgery, Zheng Zhou University Affiliated People's Hospital, from October 2014 to October 2015. The protocol was approved by the Ethics Committee of Zheng Zhou University in accordance with the Helsinki Declaration of 1975 (as revised in 2008). All individuals provided informed consent before participating in the study. All patients underwent surgery with the diagnosis of an acute abdomen. The exclusion criteria included pregnancy, a progressive fatal disease or immunosuppressive therapy, malignancy, and other extra-abdominal infections. Patients exhibiting two or more of the following signs during their first 24 h without severe sepsis were said to have SIRS: (1) temperature >38°C or <36°C; (2) pulse rate >90/min; (3) respiratory rate >20/min or hyperventilation with a partial pressure of arterial carbon dioxide (PaCO2) <32 mm Hg; or (4) white blood cell (WBC) count >0.012 × 10
Methods
Blood was drawn with heparin as an anticoagulant using a conventional blood collection tube. Samples of blood for measurement of markers were collected within 24 h after hospitalization. The WBC count, CRP, and PCT values were determined in the clinical laboratory of our hospital using commercial methods following the manufacturer's instructions. STREM-1 was measured with a double-antibody sandwich enzyme-linked immunosorbent assay (ELISA) (Quantikine Human TREM-1 Immunoassay ELISA Kit, R & D, Minneapolis, MN USA).
Statistical analysis
Measurement data were expressed as the median (interquartile range [IQR]). The Mann-Whitney U test and Kruskal-Wallis test were performed to compare means in the two groups. Receiver operating characteristic curves were drawn to illustrate various cut-off values of sTREM-1, WBC count, CRP, and PCT in patients with abdominal conditions. Spearman correlation analysis was used to assess the correlation of plasma sTREM-1 concentration and the Acute Physiology and Chronic Health Evaluation (APACHE) II score in the sepsis group. The SPSS statistical software v16.0 (SPSS, a Division of IBM; Armonk, NY USA) was used for the data analysis, and p < 0.05 was considered statistically significant.
Results
Patient characteristics
In the healthy group, 30 patients were male, and 30 patients were female, with an average age of 64 ± 11.2 years. In the SIRS group, 29 patients were male, and 31 patients were female, and their average age was 65.7 ± 14.8 years. In the sepsis group, 36 patients were male, and 32 patients were female, with an average age of 66 ± 15.2 years. Intestinal fistula (pancreatitis acuta), gastric fistula (cholecystitis acuta), acute appendicitis, ileus, and perforation of the intestine accounted for 16, 13, 12, 15, and 12 of the problems in the sepsis group, respectively. There was no significant difference in sex or age among the three groups (p = 0.09 and p = 0.07, respectively). Patients with sepsis were confirmed to have suspected or documented sepsis by microbiological tests.
Plasma concentration of sTREM-1
As shown in Table 1, the median plasma sTREM-1 values in the three groups were healthy 35.3 ng/L, SIRS 87.6 ng/L, and sepsis 169.3 ng/L. Thus, sTREM-1 was significantly increased in patients with sepsis compared with the healthy and SIRS groups (both p < 0.001; Kruskal-Wallis test). Moreover, the PCT concentrations in the healthy, SIRS, and sepsis groups were 0.2 ng/mL, 0.4 ng/mL, and 7.2 ng/mL, respectively. Therefore, the sepsis group had a significantly higher concentration of PCT than the healthy group (p < 0.001; Mann-Whitney U test), but there was no significant difference between the SIRS and sepsis groups. Similar to PCT, the concentration of CRP, the WBC count, and the temperature in the sepsis group showed significantly higher values than those in the healthy group (all p < 0.001) but not in the SIRS group. As shown in Table 2, there were significant differences between the survival and death groups in both sTREM-1 (p = 0.007) and APACHE II score (p = 0.01).
Statistically significant difference compared with health group: p < 0.001.
Statistically significant difference compared with SIRS group: p < 0.001.
For abbreviations, see text.
Correlation between plasma sTREM-1 and APACHE II score in the sepsis group
The APACHE II score was used as an index of disease severity. Spearman's rank-order correlation coefficient analysis was applied to assess the correlation between sTREM-1 and APACHE II score of patients with sepsis and acute abdominal conditions. The plasma sTREM-1 concentration correlated significantly with the APACHE II score (r = 0.41; p = 0.006) (Fig. 1).

Correlation of sTREM-1 concentration with Acute Physiology and Chronic Health Evaluation II score in the sepsis group.
Diagnostic values of sTREM-1, PCT, CRP, and WBC in patients with sepsis
The sensitivity and specificity of plasma sTREM-1 concentrations for predicting the occurrence of sepsis in patients with acute abdominal conditions were determined; for comparison purposes, we determined the concentrations of PCT and CRP and the WBC count in the same plasma samples. The ROC curves were generated for sTREM-1, PCT, CRP, and WBC of the healthy group and the sepsis group having acute abdominal conditions (Fig. 2). The AUC of sTREM-1 was 0.98, which was higher than that of PCT (0.94), CRP (0.89), and WBC (0.81). When the cut-off value of 216.33 ng/L was used, according to the Youden index, plasma sTREM-1 showed a sensitivity of 94.1% and a specificity of 96.7%. The ROC analysis revealed that sTREM-1 predicted sepsis significantly with acute abdominal conditions vs. healthy control patients compared with the other markers measured.

Receiver operating characteristic analysis of sTREM-1, procalcitonin, C-reactive protein, and white blood cell count for the diagnosis of sepsis and the healthy group.
Diagnostic values of sTREM-1, PCT, CRP, and WBC in patients with sepsis and SIRS
To explore better the availability of sTREM-1 as a potential biomarker for the diagnosis of sepsis in patients with acute abdominal conditions, a ROC analysis was used to discriminate the SIRS group from the sepsis group using the four sepsis diagnostic markers (Fig. 3). The AUC of sTREM-1 was 0.82, which was higher than that of PCT (0.77), CRP (0.72), WBC count (0.70), and APACHE II score (0.77). When the cut-off value for sTREM-1 was set to 113.06 ng/L, sTREM-1 had the optimal sensitivity (80%) and specificity (76%) for discriminating SIRS from sepsis. Altogether, these data strongly support the potential of sTREM-1 as a novel biomarker for abdominal sepsis.
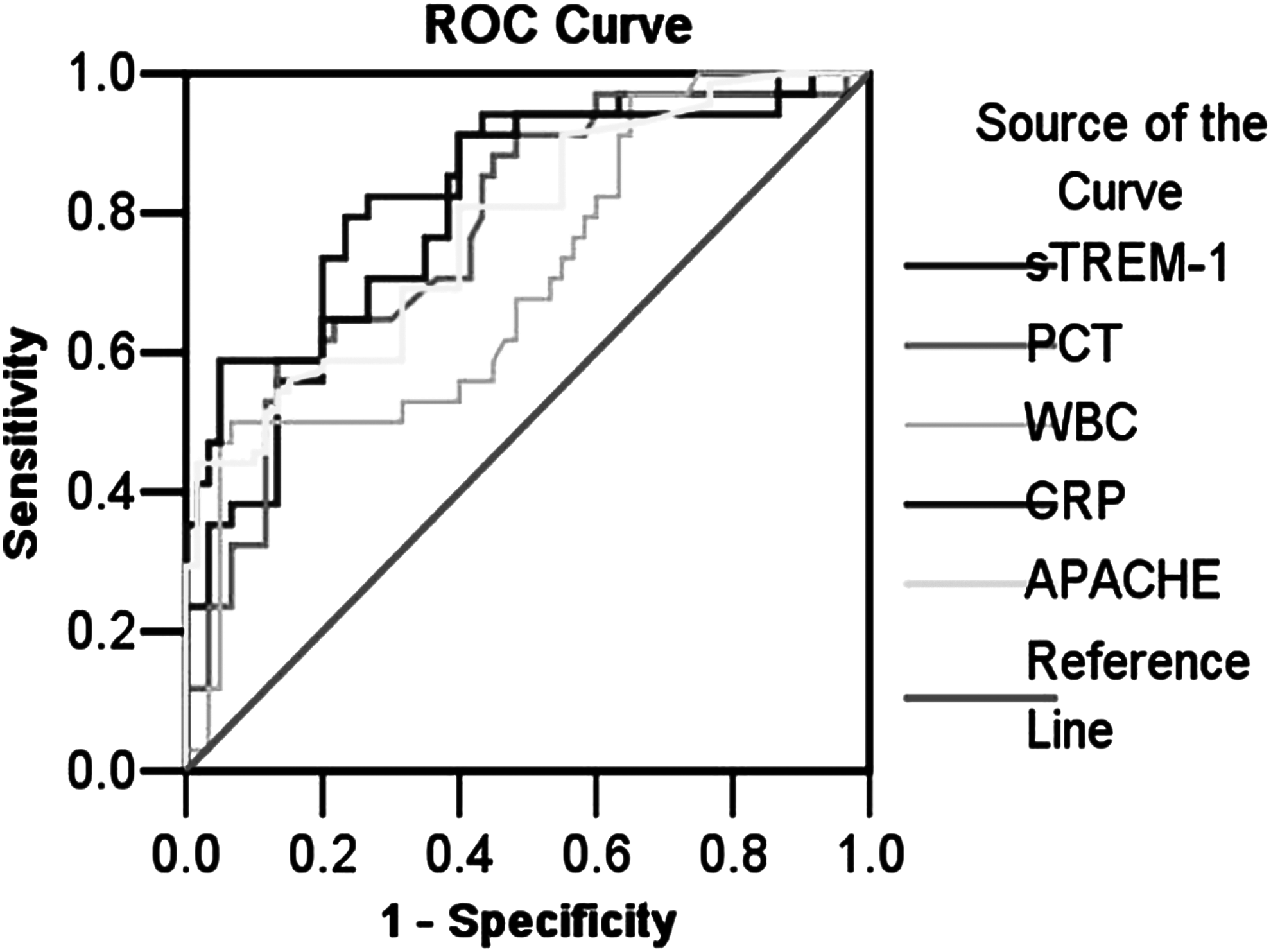
Receiver operating characteristic analysis of sTREM-1, procalcitonin, C-reactive protein, white blood cell count, and Acute Physiology and Chronic Health Evaluation II score for the diagnosis of sepsis and SIRS.
Discussion
A prompt diagnosis of abdominal sepsis is indispensable, and failure to intervene early results in morbidity and, possibly, death [13,14]. Clinical and laboratory signs of systemic inflammation are neither sensitive nor specific enough for the diagnosis of abdominal sepsis [15]. In particular, SIRS is difficult to differentiate from sepsis in acute abdominal conditions; thus, it becomes critical to identify any biomarker that can distinguish sepsis from SIRS accurately in patients with acute abdominal conditions and diagnose quickly bacteremia and predict its prognosis [16].
Many markers have been used to identify abdominal sepsis. In particular, PCT has been proposed as the most promising [17], but recently, studies found that PCT might not be useful in the early detection of infections [18–20]. C-Reactive protein has been used as a nonspecific inflammatory indicator but showed low sensitivity and specificity for the diagnosis of sepsis; thus, its role as a singular diagnostic and prognostic biomarker in sepsis remains limited [21]. STREM-1 has been suggested as a potential marker for bacterial infections [22]. The ectodomain of the protein is shed by a metalloprotease and released into the blood [23]. The plasma sTREM-1 concentration is reported to be high in pneumonia [24,25]. In addition, dynamic changes in sTREM-1 concentrations can predict the survival and mortality rates of patients in the early stage of nephritis [26–28]. All the these studies suggested that sTREM-1 has advantages in diagnosing bacterial infections. To our knowledge, there is little information about sTREM-1 in acute abdominal sepsis. In the present study, we examined the concentration of sTREM-1 in acute abdominal conditions and assessed the potential value of sTREM-1 as an accurate marker for the diagnosis of abdominal sepsis.
Our data showed that plasma sTREM-1 concentrations were significantly higher in the sepsis group than in the healthy and SIRS groups (both p < 0.001). The sepsis group had a significantly higher concentration of PCT and CRP and WBC count than did the healthy group, which indicates that sTREM-1 is likely to be a better marker for sepsis in patients with acute abdominal conditions. Moreover, the plasma concentration of sTREM-1 was significantly higher in the patients who died than that in those who survived. This result is consistent with the findings in previous studies, which demonstrated increased plasma sTREM-1 concentrations in acute pancreatitis and chronic obstructive pulmonary disease [29–31]. According to previous studies, we noticed that the plasma sTREM-1 concentrations differed significantly among different types of infections. In inflammatory bowel disease, the mean plasma sTREM-1 was 435 ± 279 ng/L [32]; in the patients with myocarditis, the mean value of sTREM-1 was 100.9 ng/L [33]; whereas in our study, the mean concentration of plasma sTREM-1 was 169.31 ± 79.27 ng/L in acute abdominal sepsis. A possible explanation may be that because various bacterial types infect different parts of the body, different ELISA kits are used for measurement.
A ROC analysis was performed for the four biomarkers and their diagnostic performance in sepsis patients with acute abdominal conditions. We found that the AUC of sTREM-1 was higher than that of PCT, CRP, and the WBC count. When 216.33 ng/L was set as the best threshold for sTREM-1, there was a sensitivity of 94.1% and a specificity of 96.7%. The ROC curve showed that sTREM-1 was a significantly sensitive indicator of sepsis compared with the other markers. These excellent performance characteristics also have been reported in other infections. For example, sTREM-1 accuracy has been demonstrated in pneumonia (98% sensitivity, 90% specificity) [34]. Moreover, to better prove the utility of sTREM-1, we used a ROC analysis to distinguish the SIRS patients from the sepsis group (Fig. 3). Our data showed that sTREM-1 was useful for discriminating these two conditions. When the cut-off value for sTREM-1 was set at 113.06 ng/L, the clinical sensitivity was 80%, and the specificity was 76%, which suggested that sTREM-1 completely separate patients with sepsis from patients with SIRS. In addition, in our study, the plasma sTREM-1 concentration correlated positively with the APACHE II score, suggesting that, to some extent, plasma sTREM-1 can reflect the severity of sepsis in acute abdominal infection. Combined sTREM-1 and APACHE II score might be even more valuable for discerning the prognosis of patients with abdominal sepsis. Moreover, the technique used for plasma sTREM-1 determination is rapid and inexpensive and can be performed on small batches of specimens or individual samples [35]. Altogether, these data strongly suggest the promise of sTREM-1 as a new biomarker for sepsis in patients with acute abdominal infection. Further studies with larger samples and additional prospective studies should define the application of sTREM-1 measurements and targeted therapy in treating sepsis.
This work represents an advance in biomedical science because for the first time, it showed higher plasma concentrations of sTREM-1 in patients with abdominal sepsis and a positive correlation between the plasma concentration and disease severity.
Footnotes
Author Disclosure Statement
None of the authors has a conflict of interest relating to this work.