
Abstract
Abstract
Background:
Diarrhea is a common condition after solid organ transplant (SOT); Clostridium difficile-associated colitis (CDAC) is one of the most common infections after SOT. We documented previously that some types of enteritis are associated with an elevation of tacrolimus (TAC) trough concentrations by interfering with the drug's complex metabolism.
Patients and Methods:
Tacrolimus concentrations of 25 SOT recipients including 12 renal and 13 liver recipients before, during, and after CDAC were analyzed retrospectively.
Results:
Median age of the 25 patients was 54 y (range, 36–71), there were 15 males and 10 females. Clostridium difficile-associated colitis developed at a median of 55 d (range 2–4551) post-SOT. Median TAC concentrations prior to the outbreak of CDAC were 6.9 ng/mL (range, <1.5–17.2), 5.6 ng/mL (range, <1.5–13.2) during diarrhea, and 7.4 ng/mL (range, <1.5–24.3) after resolution of diarrhea (p > 0.05, NS). Treatment of CDAC consisted of metronidazole for 14 d in all cases. All patients recovered from CDAC but seven patients had CDAC relapse.
Conclusions:
In contrast to other types of infectious diarrhea such as rotavirus enteritis and cryptosporidiosis, CDAC is not associated with an increase in TAC concentrations. This is because C. difficile causes primarily colitis as opposed to other organisms, which are associated with enteritis.
D
Clostridium difficile-ssociated colitis (CDAC) has emerged as a common infection after SOT [1,7–9,11–17]. The course of the disease may be more severe than in the normal host with an increased risk for recurrent disease [1,7,12,13]. This high risk of developing CDAC is based on the excessive overall risk for infectious complications caused by multiple factors, including end-stage organ failure, major surgical intervention, and immunosuppressive therapy, which all cause disturbances in the colonic microbioma [18,19]. Repeated exposure to antimicrobial agents, frequent exposure to the hospital environment, and maintenance therapy with acid-blocking medication are additional contributors to developing CDAC [20,21].
During infectious diarrhea, SOT recipients may experience an increase in tacrolimus (TAC) trough concentrations, which has been reported in patients with rotavirus enteritis and cryptosporidiosis [2,5,22,23] but this has not been studied specifically in patients with CDAC [7]. The exact mechanism of how TAC concentrations are elevated has not been elucidated completely; interference with cytochromes (CYP3A4) within the intestinal mucosa is believed to be the main reason [24]. The increase in TAC concentrations may aggravate diarrhea, exacerbate the concentration of immunosuppression, and cause nephrotoxicity and neurotoxicity [25]. The aim of this study was to analyze TAC trough concentrations retrospectively in a cohort of 25 SOT recipients with CDAC.
Patients and Methods
The institutional surgical infection database was searched for CDAC. For the time period December 1996 to September 2007, a total of 58 SOT recipients experiencing 67 episodes of CDAC were identified including one cardiac, 19 renal, two pancreas, five renal/pancreas, and 31 liver recipients. Twenty-five patients with TAC-based immunosuppression were studied with regard to their TAC trough concentrations in association with CDAC (Table 1). Only the first episode of CDAC was considered in patients with relapsing disease. The final study group included 12 renal and 13 liver recipients with a median age of 54 y (range, 36–71); there were 15 males and 10 females.
CDAC = Clostridium difficile-associated colitis; WBC = white blood cell count; TAC = tacrolimus.
Surgical technique and peri-operative management were carried out according to standard protocols. Immunosuppression included TAC at trough concentrations of 4–8 ng/mL, mycophenolate-mofetil at 1–2 g/d divided in two doses and a steroid taper with a maintenance dose of 5–10 mg/d. Subsets of patients additionally received induction with antithymocyteglobulin (ATG), muromonab antibody (OKT3), rituximab, or interleukin (IL)-2-receptor antagonists.
Peri-operative antibiotic prophylaxis consisted of piperacillin/tazobactam for most liver transplants and cefazolin for the majority of renal transplants. Trimethoprim/sulfamethoxazole (TMPS) was given per protocol from day two post-SOT for one year at a dose of 800 mg/160 mg two times per week.
Clostridium difficile-ssociated colitis was defined as presence abdominal pain, diarrhea, and/or fever with concomitant detection of C. difficile toxin from stool. A second-generation enzyme-linked immunosorbent assay (ELISA) capable of detecting toxin A and B was used.
Data are given as percentage of the entire cohort for discrete parameters and means with standard deviation or median with minimum and maximum ranges for continuous parameters. For statistical analysis, SPSS 16 (SPSS Inc., Chicago, IL) was used including χ2 test for discrete and analysis of variance (ANOVA), Student t-test and/or non-parametric Mann-Whitney U assay/Kruskal-Wallace, and Friedman test for continuous parameters. A p value <0.05 was considered statistically significant. The work was approved by the institutional ethics committee.
Results
Demographic and clinical data are shown in Table 1. Six patients developed CDAC during the first month post-transplant, another eight between one and three months, and another three between 100 and 365 d. The remaining six individuals were diagnosed after one year with a single case observed more than 10 y post-transplant. There were no differences with regard to baseline data such as age, gender distribution, body mass index, APACHE II score, white blood cell (WBC) count, or temperature at onset of CDAC or rate of recurrent CDAC between renal and liver recipients. However, renal recipients developed CDAC later than liver recipients (Fig. 1). The median APACHE II score at onset of CDAC for the entire cohort was 15 (range, 7–25).

Time from transplant to development of Clostridium difficile-ssociated colitis (CDAC) for renal (dotted line) and liver recipients; the difference is statistically significant (p = 0.016)
Eleven patients developed CDAC during hospitalization after their transplant (renal, four; liver, seven). Another five patients had other surgical interventions and seven patients had been hospitalized for medical complications such as graft dysfunction or infections prior to developing CDAC. In two cases CDAC was the admission diagnosis.
Of the 18 patients with CDAC onset more than one month post-transplant, four presented with diarrhea including the two who had CDAC as admitting diagnosis. Five had graft dysfunction (three renal graft rejections, two elevated liver enzymes), one had a peri-hepatic hematoma, and one a small bowel obstruction. Seven had infections (pneumonia, two; urinary tract infection, two; necrotizing pancreatitis, one; intra-abdominal abscess, one; and blood stream infection, one) and received antibiotics immediately prior to developing CDAC. All patients were exposed to trimethoprim/sulfamethoxazole for Pneumocystis jiroveci prophylaxis for one year.
Median onset of CDAC after hospital admission was five (range, 1–62) days. All patients received metronidazole as first-line therapy for 14 d. Seven patients had recurrent CDAC but no patient died because as a result of CDAC. During a median follow-up of 1,110 days (range, 70–4,892) post-transplant and median 1,055 days (range, 29–2,285) post-CDAC, four patients lost their renal allografts (no liver allograft was lost) and three patients died (two liver, one renal recipient). Eight patients (three liver, five renal recipients) transferred their care or were lost to follow-up including one renal recipient who had lost the graft.
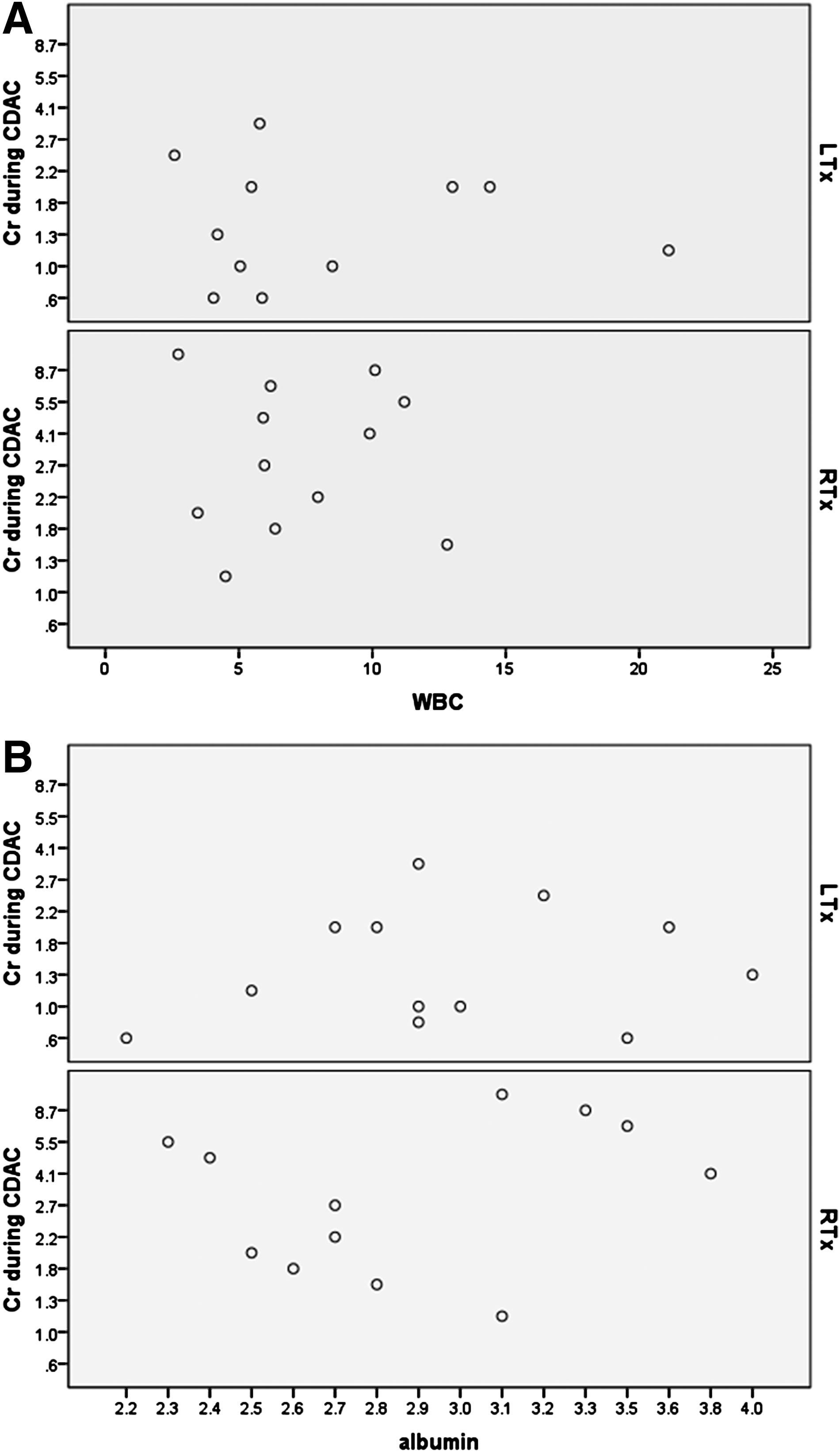
Figure 2 shows TAC concentrations at baseline, peak, and convalescence and Figure 3 shows corresponding serum creatinine concentrations for renal and liver recipients. Baseline creatinine of renal recipients was higher than in liver recipients. Neither TAC concentrations (p = 0.409) nor creatinine concentrations (p = 0.228) increased substantially in association with CDAC. At the time of CDAC, median WBC was 6 k/mL (range, 2.6–53.1) and medium serum albumin was 2.9 mg/dL (range, 2.2–4). Neither WBC nor serum albumin values differed between liver and renal transplant recipients. No correlation between serum creatinine and serum albumin values (p = 0.49 Pearson correlation) and WBC (p = 0.388 Pearson correlation) was found (Fig. 4A and 4B).
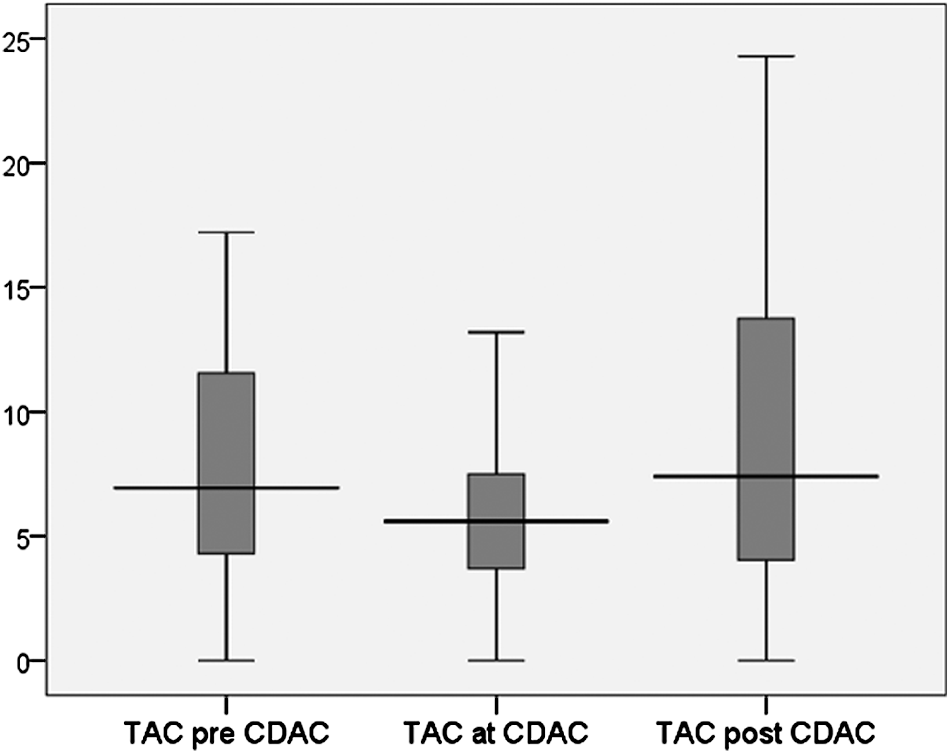
Tacrolimus (TAC) trough concentrations (ng/mL) prior, during, and after Clostridium difficile-ssociated colitis (CDAC) (p > 0.05, NS)
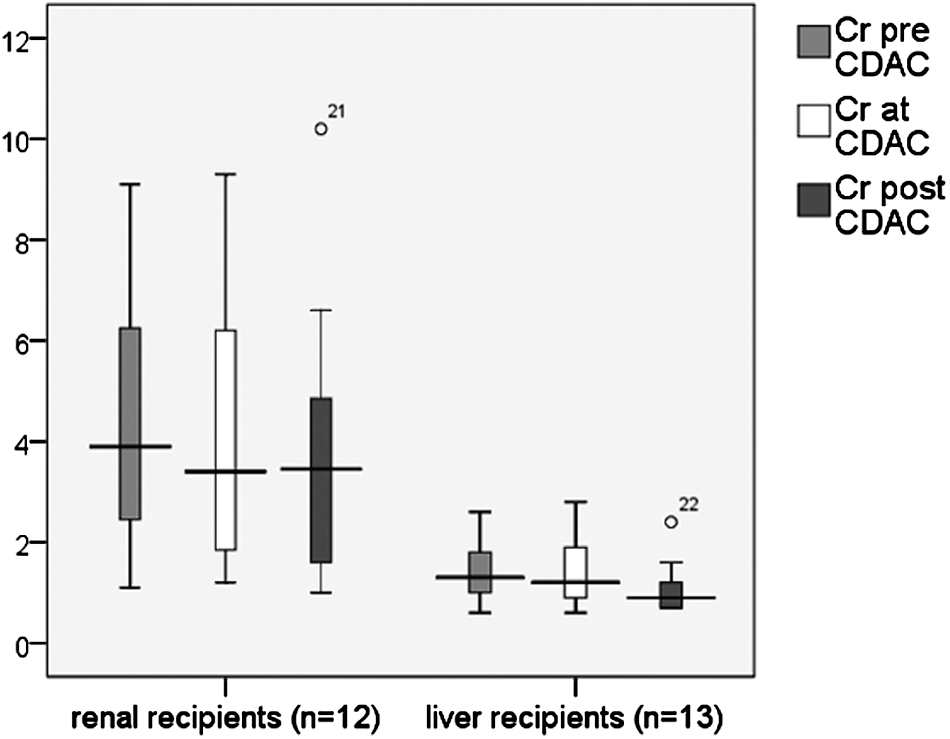
Serum creatinine values prior, during, and after Clostridium difficile-ssociated colitis (CDAC) according to the transplanted organ (p > 0.05, NS for each group)
(
Discussion
We herein report a series of 25 SOT recipients with CDAC and conclude that this colonic infection is not associated with an increase in the TAC concentrations. With that, no worsening of renal function during CDAC was observed even when correcting for severity of disease (WBC, serum albumin). Solid organ transplant recipients are a high-risk group for CDAC [26]. Rates of CDAC can be reduced using a “bundled” preventative approach focused on education, isolation precautions, and antimicrobial management [27]. To prevent CDAC in transplant recipients, baseline immunosuppression should be kept as low as possible, antibiotics should be used cautiously, and transplant patients should be kept isolated from patients with known C. difficile colonization or infection. Avoidance of acid-blocking medication may also be helpful, however, patients require these agents during the most vulnerable time period to prevent stress/steroid induced ulcers as high-dose steroids are part of most immunosuppressive protocols [21]. Clostridium difficile-ssociated colitis is a rapidly emerging global health threat carrying significant mortality and chronic carriers such as SOT recipients may serve as reservoirs for ongoing outbreaks [28]. In our own population, the prevalence for CDAC in liver transplant recipients was almost 10%, which is consistent with publications from other centers, however, there seems to be variation on the prevalence of CDAC depending on the transplanted allograft and multiple other factors [1,7,26,29].
Diarrhea has been shown to influence TAC concentrations but the exact mechanism is not known [2,5,22–24,30–32]. Major inter-individual differences in absorption, bioavailability, and metabolism of TAC should be considered [33]. Absorption of the drug decreases sequentially from the duodenum, jejunum, and ileum [34,35]. Elevated TAC concentrations may be because of increased absorption, decreased metabolism, decreased hepatic first-pass effect, and hemo-concentration. Decreased intestinal metabolism likely is the major contributor to increased TAC concentrations observed during diarrhea. The two intestinal enzymes CYP3A4 and P-gp influence TAC metabolism and absorption [33–38]. Other thus far unknown factors may be involved in the elevation of TAC concentrations during intestinal infection and some individuals may experience only minimal or no elevation [33,39–43].
Clostridium difficile-ssociated colitis usually causes pathology only in the colon and therefore has no impact on TAC trough concentrations. This is in contrast to diarrhea associated with enteritis. Rotavirus in particular has been associated with increased TAC concentrations, although other infectious causes may also function in a similar way [5,22–24,30–32,44–46]. As CDAC seems to have no impact on TAC trough concentrations, one may consider that elevation of TAC trough concentrations in SOT recipients with diarrhea may be because of enteritis and testing for rotavirus, norovirus, and Cryptosporidium should be performed.
Footnotes
Author Disclosure Statement
RGS received consulting fees from Merck, Pfizer, 3M, and GSK.
No competing financial interests exist.