
Abstract
Abstract
Background:
Despite several interventions having been adopted to reduce the incidence of incisional surgical site infection (SSI), it still remains a challenge for surgeons, because incisional SSI is a common cause of health-care–associated infection, leading to increased morbidity, prolonged hospital stay, patient discomfort, and increased sanitary costs. The aim of this study was to evaluate the effect on incisional SSI of vitamin E ointment in the subcutaneous tissue of patients undergoing a laparoscopic colorectal surgical procedure.
Patients and Methods:
A randomized study was performed. Patients with colorectal neoplasms undergoing an elective laparoscopic surgical procedure were included. The patients were randomized into two groups: Those patients undergoing a subcutaneous vitamin E ointment application (Group 1) and those patients who did not receive it (Group 2). Incisional SSI, post-operative pain, and analytical acute phase reactants were analyzed.
Results:
There were 108 patients who were assessed for eligibility, and 101 patients were analyzed. The incisional SSI rate was 4% in Group 1 and 17.6% in Group 2 (p = 0.03). Mean post-operative pain, 24 hours after operation, was 17.3 ± 10.5 mm in Group 1 and 31.9 ± 18.9 mm in Group 2 (p < 0.001). Median hospital stay was six days in Group 1 and eight days in Group 2 (p < 0.001). White blood cell count was significantly lower in Group 1 (p < 0.001).
Conclusion:
The subcutaneous application of sterile vitamin E acetate ointment leads to a reduction in the incisional SSI rate, lower post-operative pain, and decrease in C-reactive protein and white blood cell count.
D
Several interventions have been adopted to reduce the incidence of incisional SSI, including peri-operative antibiotic systemic prophylaxis, skin cleansing with antiseptic agents, adequate surgical technique, thermoregulation, or glycemic control, among other measures [4,5]. Laparoscopic approaches are generally associated with lower rates of incisional SSI than open procedures. This is especially relevant for clean-contaminated procedures, such as colon operations, where the SSI rate has been observed to be significantly lower with laparoscopy within each risk category, independent of the presence of other risk factors for SSI [6,7]. Even after minimally invasive approaches, however, incisional SSI rates can be more than 10% [8].
Local delivery of antibiotic agents to the surgical site as a means of reducing the incidence of incisional SSI has been also essayed, but with controversial results [9]. Recent articles also defend the use of triclosan-coated sutures to reduce incisional SSI [8,10]. Even local irrigation with different antibiotic agents has been investigated [11], but to date few have found their way into routine clinical practice.
Vitamin E has an immunomodulating effect on diverse pathologies, reducing the inflammatory-mediated tissue damage. Topical application of vitamin E has been proven to be effective in dermatologic diseases, demonstrating a local effectiveness [12,13]. Thus, the aim of this study was to evaluate the effect on incisional SSI of sterile vitamin E acetate ointment in the subcutaneous tissue of patients undergoing laparoscopic colorectal surgical procedures.
Patients and Methods
A randomized study was performed at the Coloproctology Unit of the University Hospital Rey Juan Carlos between January 2015 and March 2016. Inclusion criteria were a diagnosis of colorectal neoplasms and plans to undergo elective laparoscopic surgery with curative aims. Exclusion criteria were open surgical approach or conversion to laparotomy, performance of a stoma, immunodepression status (human immunodeficiency virus [HIV] or congenital immunodeficiencies, and pharmacologically induced immunodeficiencies by chemotherapeutic agents or corticoids), and anastomotic leak in the post-operative course, confirmed by computed tomography scan with rectal contrast enema.
Patients with rectal cancer receiving neoadjuvant treatment were operated on six weeks after finishing the therapy. The administration of pre-operative neoadjuvant chemoradiotherapy is not an unappealable condition for performing a stoma at our institution. The decision for performing a stoma is individualized in each patient, according to the patient's features and the surgical conditions.
The sample size calculation was based on historic data for our center's incisional SSI rate in elective colorectal surgery (18%) and an expected incisional SSI rate of 6% in the experimental group (Vitamin E ointment) dressing), based on the best data reported in the literature referring to incisional SSI after elective colorectal surgery [14]. At 80% power and a significance level of 0.05, it was calculated that 45 patients were required in each arm of the study. The number of patients was increased by 20%, in anticipation of loss at follow-up.
The patients were randomized by means of an Internet randomization module into two groups: Those patients undergoing a subcutaneous sterile vitamin E acetate ointment application (Filme Oft, Hulka SRL, Rovigo, Italy) (Group 1) and those patients who did not receive this vitamin E ointment application (Group 2) (Fig. 1). Peri-operative systemic antibiotic agents (cefazoline 2 g and metronidazole 1,500 mg; single dose pre-operatively, within 30 min of incision, and re-dosed after 4 h when the operation is prolonged over that time) were used in both groups. No mechanical bowel preparation took place in any patient.
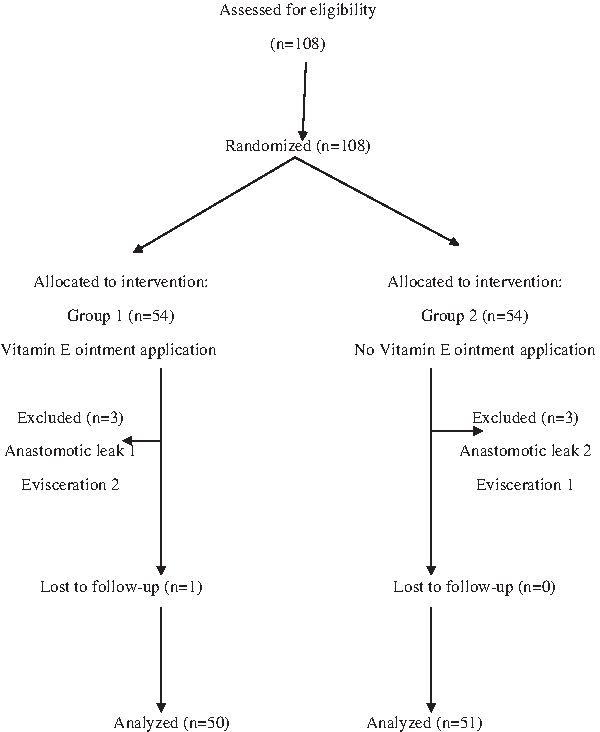
Cohort flow diagram.
Methodology
Specimen extraction and abdominal wall closure
The specimen was extracted through a supra-pubic 6 cm-Pfannenstiel incision, enlarging the port placed at this level. The incision was protected with an Alexis® device (Applied, Rancho Santa Margarita, CA), to avoid the contact of the specimen with the abdominal wall. The aponeurotical layer was sutured with polydioxanone loop number 1 (Ethicon, Johnson & Johnson, Somerville, NJ). The fascial layer of the rest of the port sites was not closed. The skin was closed with staples.
Before the skin closure, the subcutaneous tissue was irrigated with 50 mL of physiologic saline to eliminate secretions and cell detritus. After placing the staples, povidone-iodine solution was applied to the incisions, and they were covered with gauzes and a plastic adhesive tape. The dressing was maintained for 72 hours, excepting for those patients with accumulation of secretions in the gauzes or with signs of incisional SSI. In such cases, the dressing was removed and changed with a similar one, following an aseptic technique.
Vitamin E application in the subcutaneous tissue
Before the skin stapling and after the subcutaneous irrigation with physiologic saline, sterile Vitamin E acetate ointment was applied in the subcutaneous tissue; 2 mL were applied in the supra-pubic incision and 0.5 mL in each of the rest of the port sites.
Analgesia regimen
Post-operative analgesia included metamizole 2 g/8 h and acetaminophen 1 g/8 h, alternating every four hours. When post-operative pain, as measured by the visual analogue scale (VAS), overcame 50 mm at any moment in the post-operative course, 5 mg of subcutaneous morphine was administrated.
Variables
The investigated clinical variables were age, gender, co-morbidities, location of the neoplasm, complications (anastomotic leak, evisceration, organ-space SSI, and incisional SSI), death, and hospital stay. Technical variables evaluated were surgical technique and performance of a stoma. Micro-biologic cultures were obtained from the infected surgical incisions. Post-operative pain was evaluated 24 hours after surgery by means of a VAS, ranging from 0 mm (complete absence of pain) to 100 mm (unbearable pain). Acute phase reactants (white blood cell count [WBC], fibrinogen, and C-reactive protein [CRP]) 48 hours after surgery were also investigated.
Incisional SSI was defined following CDC criteria [15]. When a purulent discharge from the surgical incision was present, a sample was obtained for micro-biologic confirmation. Incisional SSI was determined by an epidemiology nurse blinded to the treatment groups. Infection surveillance was extended for 30 days after discharge; all patients were evaluated 30 days after operation in the outpatient clinic. If the patients presented symptoms suggestive of SSI before the 30-days visit, they were advised to go to the emergency department. Once the incisional SSI was diagnosed, the incision was opened and the purulent discharge drained.
Statistics
Statistical analysis was performed with the statistical software SPSS 19.0 for Windows. Quantitative variables that followed a normal distribution were defined by the mean and standard deviation. For non-Gaussian variables, the median and range were used. Qualitative variables were defined by number and percentage of cases.
Comparison of variables was performed with a Student t-test and the Pearson correlation method for quantitative variables following a Gaussian distribution. Non-parametric tests (Mann-Whitney and Spearman correlation) were used for non-Gaussian variables. Comparison of qualitative variables was performed with the chi-square test; in those cases with fewer than five observations in the cell, the Fisher exact probability method was used (p < 0.05 was regarded as significant).
The study was approved by the local ethics committee. Informed consent was obtained from all participants included in the study.
Results
There were 108 patients assessed for eligibility. Six patients were excluded from the analysis, because they presented an anastomotic leak or were re-operated on because of evisceration. One patient in Group 1 was lost to follow-up before the 30th day of the post-operative course. In total, 50 patients were analyzed in Group 1 and 51 in Group 2. The patient sample consisted of 59.4% males and 40.6% females, with a mean age of 69.1 + 11.4 years. Co-morbidities included diabetes mellitus (26.7%), high blood pressure (45.5%), dyslipidemia (30.7%), cardiopathies (20.8%; 15.6% atrial fibrillation and 5.2% ischemic cardiopathy), chronic obstructive pulmonary diseases (9.9%), chronic renal failure (2%), and non-decompensated cirrhosis (2%). The pre-operative diagnosis was adenocarcinoma in all the patients. There were no differences in co-morbidities between groups, and their distribution is summarized in Table 1.
NS = non-significant.
The tumors were located in the right colon (27.7%), the transverse colon (3%), the left colon (32.7%), and the rectum (32.7%). In four patients, two synchronic neoplasms were detected in different locations of the colon. The surgical techniques are described in Table 2. There were no significant differences in the surgical techniques between groups. All the anastomoses were stapled: In the left colon and rectum, a circular stapler was used (EEA 31 mm, Covidien, Minneapolis, MN); in the transverse and ileocolic anastomoses, a lineal stapler was used. Transverse and ileocolic anastomoses were performed extracorporeally through the Pfannenstiel incision. The rest of the anastomoses were performed intra-corporeally. The specimen was extracted in all cases through the Pfannenstiel incision.
NS = non-significant.
Anastomotic leaks appeared in three patients (3%), including one patient in Group 1 and two patients in Group 2 (non-significant: NS). All the anastomotic leaks appeared in colorectal anastomoses. Global organ/space SSI was 5%, 6% in Group 1 and 4% in Group 2 (NS). Evisceration appeared in two patients in Group 1 and one patient in Group 2 (NS); all these patients were re-operated on for abdominal wall closure, but were excluded from the statistical analysis. Evisceration occurred the first, second, and fourth day after operation, and none of the patients presented SSI criteria at the moment of the diagnosis of evisceration. The mortality rate was 1%, affecting one patient in Group 2 (NS). The cause of peri-operative death (extended for 30 days after operation) was an anastomotic leak and sepsis. Median hospital stay was six days (range 5–40 d) in Group 1 and eight days (range 6–42 d) in Group 2 (p < 0.001).
The incisional SSI rate was 4% in Group 1 and 17.6% in Group 2 (odds ratio [OR] 0.199; confidence interval [CI] 95% (0.041–0.973); p = 0.03). The cultures of the incision discharge in patients in Group 1 grew only Bacteroides fragilis. The polymicrobian cultures of the samples obtained from patients in Group 2 grew Escherichia coli, Streptococcus spp., Klebsiella spp., Proteus spp., and B. fragilis (Fig. 2). These micro-organisms were not resistant to the peri-operative systemic antibiotic agents administrated. There was no significant association between any of the co-morbidities and incision infection. The type of operation did not show any impact on SSI.
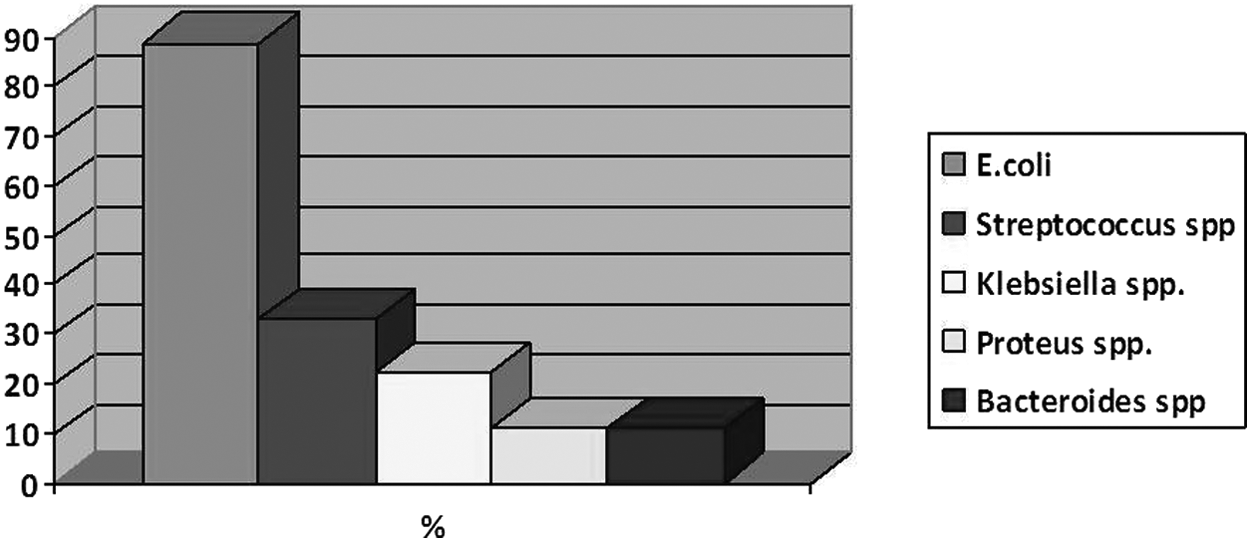
Micro-organisms involved in the incisional surgical site infection in Group 2. E. coli = Escherichia coli. Color images available online at www.liebertpub.com/sur
Mean post-operative pain, as quantified by VAS 24 hours after operation, was 17.3 + 10.5 mm in Group 1 and 31.9 + 18.9 mm in Group 2. The mean difference was 14.6 mm, CI 95% (8.1–21.1); p < 0.001.
Effect on acute phase reactants 48 hours after operation
Mean values of evaluated acute phase reactants are shown in Table 3. The WBC was significantly lower in Group 1 (mean difference 2,082/m3, CI 95% (997.9–3,167.7); p < 0.001). There were no significant differences between groups in fibrinogen values. The CRP levels tend to be lower in Group 1, however (p = 0.059).
NS = non-significant.
The WBC 48 hours after operation was significantly higher in those patients in whom incisional SSI developed later (mean difference 1,360.9/mm3; CI 95% (572.1–2,264.6); p = 0.042). Similarly, CRP levels were greater in the patients presenting incisional SSI (mean difference 8.6 mg/dL; CI 95% (5.5–11.6); p < 0.001).
Discussion
The immunomodulation effect of vitamin E affects humoral and cell-mediated immune responses. Vitamin E has demonstrated modulation of neutrophils recruitment to the damaged tissue [12]. Topical application of vitamin E ointment has demonstrated a certain anti-inflammatory effect in dermatologic diseases. Vitamin E achieves a reduction of edema and moderates the increase of cyclo-oxigenase-2 (COX-2), an enzyme that catalyzes the synthesis of prostaglandin E2, involved in the local inflammatory response against aggression [13]. Vitamin E has been widely used in gynecologic disorders, mainly affecting the vulvar skin [16].
Post-operatively, the vitamin is used with cosmetic effect, because the reduction of the local inflammatory response is associated with a smaller scar [10]. Moreover, vitamin E is also associated with a reduction in post-operative pain of skin wounds [17]. A recent study by our group demonstrated that the topical application of vitamin E ointment on the surgical bed of hemorrhoidectomy achieves a significant reduction of post-operative pain, probably because of a modulation of the inflammatory response to the surgical aggression [18].
We have to accept that an incidence of SSI of 17.6% in the control group is slightly higher than data reported in the literature for laparoscopic elective colorectal surgery [4,10]. This is the “usual” SSI rate for our institution, however, and forces us to develop new strategies searching for an improvement in our clinical results.
As mentioned previously, local drug delivery for prevention of incisional SSI was based on application of antibiotic or antiseptic agents, based on the hypothesis that these agents might reduce the bacterial contamination and consequently reduce the infection rate. It is widely known, however, that the three factors participating in surgical infection are bacterial contamination, the surgical team, and the host. Thus, a different inflammatory response to local aggression might contribute to the development of SSI, with the immunomodulating effect of vitamin E acting as a protective factor against it [4].
Moreover, independent of this immunomodulation, the acetate radical of vitamin E acetate applied in this study might also have a bactericidal effect. Acetate radicals have been shown to be highly effective against gram-negative micro-bacteria [19].
Curiously, in both groups, the prevalence of anaerobic bacteria causing the incisional SSI rate was similar, despite the fact that the global incidence of the incisional SSI rate was significantly lower in the patients receiving vitamin E ointment. A possible explanation for this finding is that vitamin E acts as a co-factor in the hydrogenization of unsaturated fatty acids, induced only by anaerobic micro-organisms (not by aerobic ones), leading to a local reduction of these fatty acids, including omega-3 fatty acids, in the subcutaneous tissue [20]. Omega-3 fatty acids have demonstrated a bacteriostatic and bactericidal effect [21]. This probably justifies the resistance of anaerobic bacteria to the bactericidal and immunomodulating effect of vitamin E.
Acute-phase reactants are produced not only during infection but also in many types of inflammation, including the normal post-operative course after open or laparoscopic abdominal surgical procedures. In patients in whom complications developed, however, this elevation is significantly higher than in patients with an uneventful post-operative course [22]. The different acute phase reactants present different time peaks, and long-term monitoring of their levels would reveal the different dynamics of these molecules in patients presenting post-operative complications, when compared with those uncomplicated ones.
Serum CRP levels show a peak 48–96 hours after surgery. In patients with an uneventful post-operative course, the peak decreased after 2 days, while a prolonged increase in its levels has been described as an indicator of impending complications [23,24]. We have observed in our sample, however, a significant difference in the post-operative CRP levels between patients in whom incisional SSI developed and those with an uneventful post-operative course in the analytical determination 48 hours after operation; CRP levels were significantly higher in the patients in whom complications developed.
Similar to CRP, fibrinogen increases its levels after the operative trauma, but in this case, the peak is obtained later than 48 hours post-operatively. Therefore, we could not observe differences between groups or between the patients in whom SSI developed and those in whom SSI did not develop. The WBC is probably the acute phase reactant with the earliest peak [25]. Thus, in the laboratory data obtained 48 hours after operation, significant differences could be observed; the WBC count was lower in the patients receiving Vitamin E ointment and in those with an uneventful post-operative course.
The association of Vitamin E ointment with a lower CRP level and WBC reflects that apart from a protective effect against incisional SSI, the immunomodulation induced by Vitamin E reduces the surgical aggresion just caused by the surgical procedure, independent of the development of SSI. The clinical translation of this lower inflammatory response induced by vitamin E is lower pain perception, as measured by VAS 24 hours after operation.
Conclusion
The subcutaneous application of sterile vitamin E acetate ointment leads to a reduction in the incisional SSI rate, lower post-operative pain, and a decrease in CRP and the WBC.