
Abstract
Abstract
Necrotizing soft tissue infections (NSTI) have been recognized for millennia and continue to impose considerable burden on both patient and society in terms of morbidity, death, and the allocation of resources. With improvements in the delivery of critical care, outcomes have improved, although disease-specific therapies are lacking. The basic principles of early diagnosis, of prompt and broad antimicrobial therapy, and of aggressive debridement have remained unchanged. Clearly novel and new therapeutics are needed to combat this persistently lethal disease. This review emphasizes the pillars of NSTI management and then summarizes the contemporary evidence supporting the incorporation of novel adjuncts to the pharmacologic and operative foundations of managing this disease.
N
Numerous terms have been used to describe NSTIs, including hospital gangrene, necrotizing erysipelas, suppurative fasciitis, clostridial gangrene, and gas gangrene. Wilson introduced the term necrotizing fasciitis in 1952 to refer to both gas-forming and non–gas-forming necrotizing infections [7]. Because diagnosis and management requires a similar approach regardless of the anatomic location or depth of involvement, necrotizing soft tissue infection has now supplanted necrotizing fasciitis as the preferred term, because it encompasses all forms of this potentially devastating infection.
The NSTIs are characterized as a collection of rapidly advancing, often fatal, infections of the soft tissue compartment (dermis, subcutaneous tissue, superficial fascia, deep fascia, or muscle). Typically, they are not associated with an abscess, but if an abscess is left untreated or is inadequately drained, it may transition to a rapidly progressive, necrotizing infection. Although a recent query of the Nationwide Inpatient Sample (1998–2010) reported a reduced incidence, there are still approximately 3,800–5,800 cases annually in the United States, with a case complication rate of nearly 50% and a case fatality rate of 5%–10% [8].
The basic principles of early diagnosis, prompt and broad antimicrobial therapy, and aggressive, serial, surgical debridement remain the pillars of therapy aimed at reducing morbidity and death [9–12]. Indeed these are the only factors that we, the clinicians, can modify to optimize outcome, and the data are nearly incontrovertible that delay, particularly in operative debridement, is associated with an increased risk of death [13–16]. Unfortunately, these basic principles have remained unchanged for decades, which likely underlies the relatively stagnant and still high and unacceptable mortality rates. Clearly novel and new therapeutics are needed to combat this persistently lethal disease.
In this study, we review the epidemiology, classification, and microbiology of NSTIs and subsequently provide a contemporary perspective of diagnosis and management. We conclude by conducting a systematic review to summarize the contemporary evidence supporting the incorporation of novel adjuncts to the pharmacologic and operative foundations of managing this disease: Hyperbaric oxygen therapy, intravenous immunoglobulin (IVIG), and blood purification.
Methods
We performed a systematic review of the MEDLINE and the Cochrane Database of Systematic Reviews from 2005 to 2015 using specific search strategies. We provide search strings and Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram as Appendix A (see online supplementary material at ftp.liebertpub.com). We restricted articles to adult (age ≥18 years) human data reported in the English language only. We screened articles published between January 1, 1995 and December 31, 2015. We focused on randomized clinical trials (RCTs), meta-analyses, systematic reviews, and clinical practice guidelines. We excluded opinion articles, commentaries, and case series, although we did incorporate observational trials.
After screening 2,773 titles and abstracts, more articles were identified for full-text review, after which manual review of bibliographies generated 25 additional references. A total of 86 articles were reviewed manually, of which 64 were selected with relevant content (Fig. 1). We selected only articles deemed to provide major advances in the treatment of patients with NSTI. We considered sources of bias in these articles and defined areas of uncertainty as those in which the evidence conflicted. We used a systematic weighting of strength of recommendation and quality of evidence using the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) system [17–20].
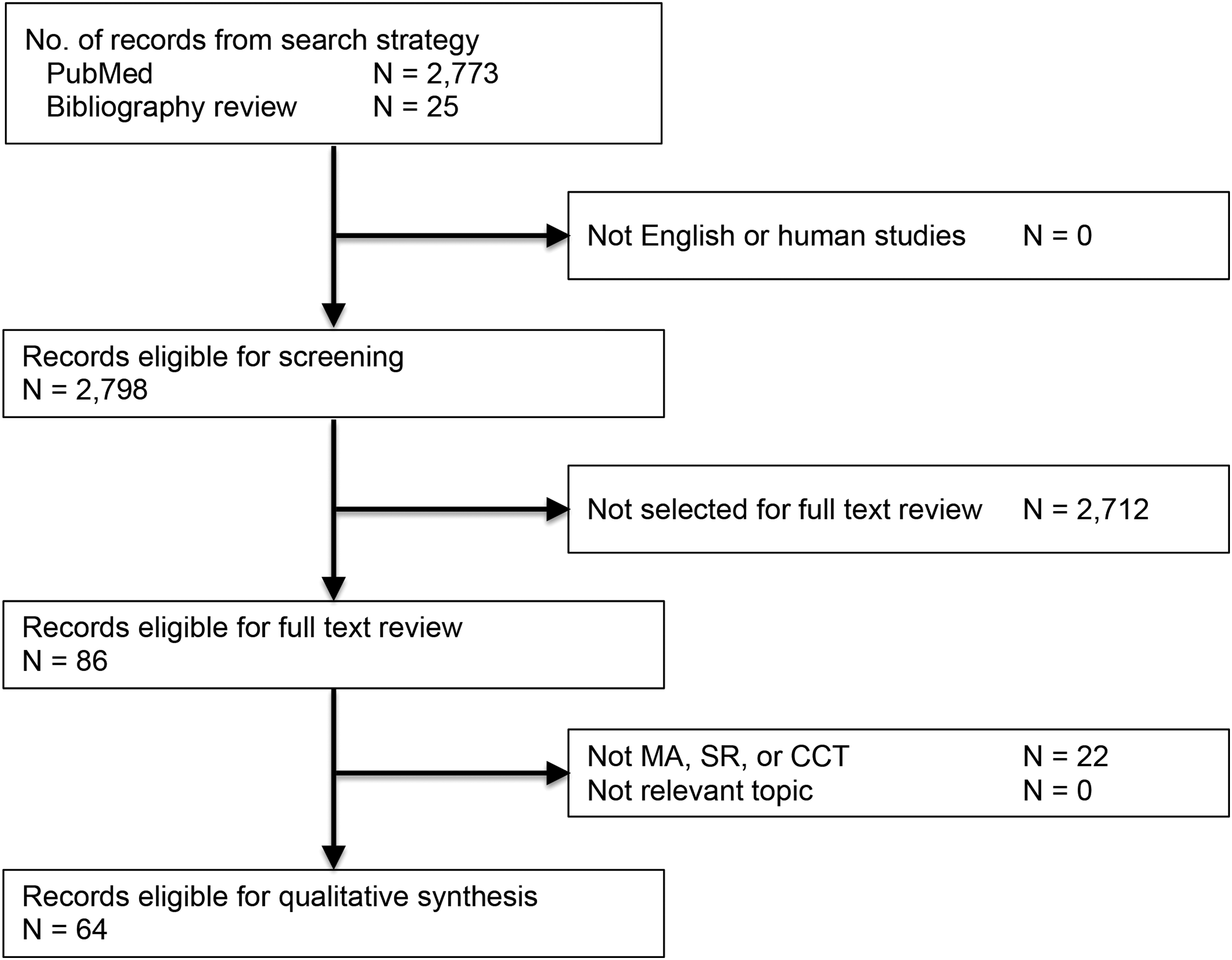
PRISMA flow diagram. MA = 8; SR = 3; CCT (not observational) = 21. Observational trials with controls = 32.
NSTIs
Epidemiology
The NSTIs are rare, with an estimated incidence in the United States to be between 500 and 1,500 cases per year [21]. Using insurance databases, Ellis Simonsen et al. [22] determined the incidence of NSTI to be 0.04 cases per 1,000 person years. Using the Nationwide Inpatient Sample from 2001 and 2004, Endorf et al. [23] found 10,940 patients (0.04%) with NSTI. Males were significantly more likely to have a NSTI (66.3% vs. 63.5%, p < 0.001).
The NSTI patients require extensive intensive care unit (ICU) and hospital resources. In the United Kingdom (UK) between 1995 and 2006, 0.24% of ICU admissions were because of necrotizing fasciitis [24]. In a study of patients admitted to burn centers versus non-burn centers, the average length of stay was 22.1 days for burn centers and 16.0 days for non-burn centers [23]. The cost of care is significant and ranges from $71,000 to $83,000 [23]. The majority of patients with NSTI are treated by surgeons in the community, but increasingly, these patients are being referred to tertiary care hospitals and burn centers for specialized wound and critical care management.
Death from NSTI has decreased over the past 30 years. In the UK between 1995 and 2006, patients with NSTI had a mortality rate of 41.6%. A review of 27 case series between 1980 and 1998 reported an estimated mortality rate of 32% [25]. In 67 studies that included 3,302 patients from 1980–2008, the overall mortality rate was 23.5% [26]. There was only a slight downward trend of 27.8% to 21.7% between those studies published from 1980 to 1999 and the studies from 1999–2008 [26]. A review of NSTI from the National Surgical Quality Improvement Program database found a mortality rate of only 12% [27]. In a study of NSTI at six academic hospitals in Texas between 2004 and 2007, mortality rates varied between 9% and 25% [28].
Comparison between studies is difficult because of the rarity and the heterogeneity of disease presentation. Improvements in outcome continue to require early diagnosis, early and aggressive surgical debridement, early administration of appropriate empiric antibiotic agents that are then tailored to microbiologic identification and antimicrobial susceptibility, and optimization of underlying medical co-morbidities.
Classification
Skin and soft tissue infections are classified in numerous ways and often for specific reasons. For purposes of evaluating new therapeutics for the management of soft tissue infections, the Food and Drug Administration classifies soft tissue infections into two broad categories: Uncomplicated and complicated. Uncomplicated soft tissue infections include superficial infections such as cellulitis, impetiginous lesions, furuncles, and simple abscesses that can be managed with surgical incision alone. Complicated soft tissue infections such as infected ulcers, infected burns, and major abscesses require significant surgical interventions. For clinical therapeutic trials, NSTI is generally an exclusion criterion.
A more useful classification divides soft tissue infections into either non-necrotizing or necrotizing infections. It is important to differentiate necrotizing infections from non-necrotizing infections, because necrotizing infections require aggressive surgical management. Necrotizing infections can be divided further into specific types based on anatomy (e.g., Fournier, Ludwig angina), depth of involvement (e.g., necrotizing adipositis, fasciitis, or myositis), microbial source of infection (types 1, 2, 3), or even a combination of microbial source and depth (i.e., clostridial cellulitis, non-clostridial anaerobic cellulitis).
Microbiology
Three basic microbial sub-types have been described. Type 1 infections are poly-microbial in nature and are the most prevalent form of NSTI, occurring in 55%–75% of NSTIs [16]. Type 2 infections are mono-microbial and are caused by Group A Streptococcus (GAS). Some authors also consider mono-microbial infections from community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA) as Type 2 [29]. Type 3 infections are also mono-microbial and are attributed to Clostridium species or rare virulent microbes such as Vibrio vulnificus or Aeromonas species [29,30].
Type 1 infections are a mix of aerobic and anaerobic bacteria and average 4.4 isolates per specimen [31]. The predominant aerobic isolates are Streptococcus species, Staphylococcus species, Enterococcus species, Enterobacteriaceae family (Escherichia coli, Klebsiella species), Pseudomonas species, and Acinetobacter species. Bacteroides species are the most common anaerobic organisms. Clostridium species are common participants in poly-microbial infections but are not necessarily causative of myonecrosis. Fungal species are occasional pathogens [14,31].
Poly-microbial NSTIs tend to occur on the perineum and trunks of immunocompromised patients. Fournier gangrene is a classic example of poly-microbial NSTI. Diabetes mellitus and peripheral vascular disease are common predisposing factors in poly-microbial NSTI [32]. Other predisposing factors include obesity, chronic renal failure, human immunodeficiency virus (HIV) infection, alcohol abuse, abscess, intravenous (IV) drug use, insect bites, recent surgical incisions, and perforation of the gastrointestinal tract [29,33,34]. Interestingly, an inciting event is never identified in 20%–50% of the patients [14,15,35].
Another example of Type 1 NSTI is cervical necrotizing fasciitis. Bacterial penetration into the fascial compartments of the head and neck results in a rapidly progressive gangrenous cellulitis with life-threatening airway obstruction. It is most often associated with an odontogenic infection (78%–90%), but other causes include trauma, tongue piercing, neoplasm, and other parapharyngeal infections [36–39]. Both Ludwig angina (submandibular space infection) and cervical necrotizing fasciitis are usually caused by mouth anaerobes such as Fusobacterium species, anaerobic Streptococcus species, Peptostreptococcus species, Bacteroides species, and spirochetes.
Type 2 NSTIs are caused by GAS (S. pyogenes) either alone or in association with S. aureus. In up to half of patients, Type 2 infections may be accompanied by toxic shock syndrome [40,41]. In contrast to Type 1 NSTI, Type 2 NSTI can occur in any age group and without predisposing medical conditions [14]. Predisposing factors include a history of trauma, IV drug use, surgical procedures, childbirth, burns, exposure to a case, and potentially non-steroidal anti-inflammatory drugs (NSAIDS) [42,43].
Over the past 10 years, MRSA has been seen increasingly as a mono-microbial cause of NSTI. The CA-MRSA that is overwhelmingly associated with NSTI is clone USA300 containing the Panton-Valentine leukocidin cytotoxin [44]. In some communities, this CA-MRSA is responsible for more than 15% of NSTI [43]. Although CA-MRSA most commonly causes necrotizing infection of the subcutaneous tissue and skin, more severe invasive disease such as necrotizing fasciitis and pyomyositis are being reported increasingly [44,45].
Clostridial infections have been classified by some as Type 3 NSTI [30]. Clostridium species are gram-positive, spore-forming, anaerobic rods normally found in soil and the gastrointestinal tract. Clostridial infections are associated classically with trauma or surgery. As surgical technique and wound care have improved, clostridial infections have decreased and are more likely now to be associated with wounds from IV drug abuse [15,46,47]. Clostridium perfringens is the etiology of 70%–80% of clostridial infections [48]. Its local and systemic manifestations are because of the production of potent extracellular toxins. Alpha toxin (a phospholipase C) and theta toxin (perfringolysin) are the two most potent proteins causing hemolysis, microvascular thrombosis, and myonecrosis [48]. Alpha toxin directly inhibits myocardial contractility and indirectly induces systemic cytokine expression, which may contribute to the circulatory collapse commonly seen with this infection [48]. Spontaneous gas gangrene is a rare clostridial infection caused by the hematogenous spread of C. septicum from the gastrointestinal tract in patients with a perforation from colon cancer or diverticulitis [49].
Members of the Vibrionaceae family (V. vulnificus and others) and Aeromonas species, are rare but potentially lethal causes of NSTI. Vibrio vulnificus is endemic to warm coastal waters and raw seafood while Aeromonas species are found in fresh or brackish water, soil, or wood [50–52]. Patients at greatest risk appear to be those with underlying hepatic dysfunction, diabetes mellitus, and other immunocompromised conditions [51,53–55].
The clinical signs and symptoms of V. vulnificus and Aeromonas NSTI are similar. Patients with hemorrhagic bullae, subcutaneous bleeding, purpura, necrosis, and gangrene who present with a fulminating course should raise suspicion of these entities. Clinical history should help differentiate the potential source, because exposure to seawater or shellfish would suggest Vibrio species, while exposure to fresh or brackish water, soil, or wood would point to Aeromonas species. Treatment usually necessitates aggressive debridement, especially in those patients with shock, leukopenia, severe hypoalbuminemia, and underlying chronic illness, especially a combination of hepatic dysfunction and diabetes mellitus [52]. These infections are aggressive, resulting in a high rate of amputation and death.
Mucormycosis (most familiar as zygomycosis) is an uncommon but potentially devastating cause of NSTI. These fungi are ubiquitous and found in soil, manure, plants, and decaying material [56]. Agents most commonly found in human infections are Mucor, Rhizopus, Rhizomucor, Lichtheimia, and Cunninghanmella [57]. Cutaneous mucormycosis is associated with trauma and burn wounds and has mortality rates ranging 38%–80% [58,59]. Patients in whom cutaneous mucormycosis develops from minor breaks in the skin almost always have an underlying disease causing immunosuppression [56,60,61]. Treatment of patients with cutaneous mucormycosis requires aggressive debridement, antifungal therapy, and elimination of predisposing factors for infection such as hyperglycemia, metabolic acidosis, deferoxamine administration, and neutropenia. Deferoxamine, which chelates both iron and aluminum, has been associated with promoting tissue invasion by behaving as a siderophore and supplying the organisms with iron [62,63].
Clinical presentation
The presentation of NSTI varies widely, ranging from skin and subcutaneous necrosis to life-threatening sepsis with muscle and fascial involvement. Although necrotizing infection leads to massive destruction of tissues, the initial presentation is not always obvious, because it may involve only the deep tissues in the early phases, leaving the overlying skin appearing normal. This makes the diagnosis of NSTI very difficult. It is important to recognize NSTI early, because delay in the diagnosis and treatment is associated with extensive tissue destruction, limb loss, and death [41,64–67].
Localized pain may be the earliest symptom of NSTI [66, 67]. Pain out of proportion to the physical appearance should raise the suspicion of NSTI. Other clinical manifestations may be edema beyond the area of erythema, skin anesthesia, epidermolysis, and bronzing of the skin (Table 1). Hemorrhagic bullae, crepitus, foul odor, “dishwater” drainage, and dermal gangrene are late manifestations and are usually associated with systemic sepsis and organ dysfunction [68]. An apparent superficial cellulitis that progresses rapidly, fails to respond to standard therapy, or is associated with evolving systemic signs of sepsis must raise the suspicion of a more extensive underlying infection.
There are multiple risk factors associated with NSTI (Table 2). These include advanced age (>60 years), IV drug use, diabetes mellitus, obesity, malnutrition, congestive heart disease, chronic pulmonary disease, peripheral vascular disease, chronic alcoholism, and immunocompromised states such as malignancy, steroid use, transplantation, and HIV infection [68–70]. Several studies have demonstrated that IV and subcutaneous injection of illicit drugs is the greatest risk factor for NSTI in the urban setting [69,71,72]. Thus, a soft tissue infection in a patient with a recent history of injection should raise the suspicion of more extensive underlying necrotizing infection. It is also important to note that NSTIs do occur in healthy persons as much as 30% of the time [73].
HIV = human immunodeficiency virus; AIDS = acquired immunodeficiency syndrome.
The reported sites of soft tissue infections vary depending on the series [68,69,73]. The most common site of infection is the extremity, followed by perineum and buttocks, trunk, and head and neck. The cause of NSTI is not always obvious and usually involves tissue damage. The reported etiologies are injection of illicit substances, cutaneous infection or ulceration, post-operative infection, peri-rectal abscesses, soft tissue trauma, strangulated hernias, perforated viscus, colostomy site infection, and idiopathic causes [69,74,75]. The association between NSAIDS and NSTI has also been shown [76–78]. It is unclear, however, whether this association is attributable to the immunomodulatory effect of NSAIDS or to the fact that patients with NSTI use NSAIDS to suppress fever and pain. Nevertheless, NSAIDS may mask the usual signs of inflammation and thereby delay the diagnosis.
Diagnosis
Early diagnosis of NSTI is difficult, because early clinical cutaneous manifestations may not be distinguishable from simple superficial infection. There are several methods proposed for the early diagnosis of NSTI. One such method is the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score by Wong et al. [79]. The score was devised retrospectively, based on six common clinical parameters: Serum C-reactive protein (CRP), white blood cell count, hemoglobin concentration, serum sodium, serum creatinine level, and serum glucose level (Table 3). According to the authors, a minimum score of 6 is associated with necrotizing fasciitis, with a positive predictive value of 92% and negative predictive value of 96%. Since the development of the LRINEC score, a few cohort studies attempted to validate its clinical use for the diagnosis of NSTI. In one study, Su et al. [80] reviewed retrospectively 209 patients with a confirmed diagnosis of necrotizing fasciitis and showed that only 100 of 209 (48%) had a LRINEC score ≥6. These authors also demonstrated, however, that the group of patients with LRINEC scores ≥6 had a higher rate of amputation and death compared with the group with LRINEC scores <6. This study suggests that the LRINEC score may be more helpful in prognosticating than in diagnosing NSTI.
In a more recent cohort study of a much smaller scale (N = 28 patients), the LRINEC score was found to have a sensitivity of 80%, a specificity of 67%, a positive predictive value of 57%, and a negative predictive value of 86% [81]. The sensitivity and specificity reported here are much smaller than those proposed by Wong et al. [79]. Mills et al. [27] reported that leukocytosis and hyponatremia occur simultaneously in only 22% of patients with NSTI, suggesting that the sensitivity of these parameters for the detection of NSTI is low. The major drawback of the LRINEC scoring system is that it is derived from retrospective data and is therefore predisposed to selection bias.
Imaging studies such as conventional radiography and computed tomography (CT) are only helpful if there is gas in the tissue. The presence of gas in the tissue together with a suspicious clinical presentation is pathognomonic of NSTI. Radiographic detection of sub-cutaneous emphysema, however, is seen in only 39% of patients with NSTI [82]. In detecting inflammatory changes, CT is very sensitive but is not necessarily specific for necrotizing infection. In the diagnosis of deep abscesses, however, CT is helpful, especially intra-muscular abscesses that otherwise cannot be diagnosed with physical examination. Magnetic resonance imaging (MRI) with gadolinium contrast enhancement can accurately differentiate between necrotizing infection from non-necrotizing infection [83]. Unfortunately, the time it takes to obtain an MRI scan, especially in an unstable patient with sepsis, who may be undergoing aggressive resuscitation, is difficult to justify. The MRI scan is not always accessible readily in many facilities. Further, an MRI scan requires patient compliance, and any movement by the patient during the study may render a very time-consuming study non-interpretable, thus further delaying diagnosis and treatment.
Bedside tissue biopsy with frozen section has been suggested for the diagnosis of NSTI [84]. The diagnosis is made based on histologic changes that include tissue necrosis, poly-morphonuclear infiltration, fibrinous vascular thrombosis, and sometimes micro-organisms within the destroyed tissue. Although the reported series shows this method to be reliable, the experience is limited. Further, a pathologist is not always available readily at night for frozen section interpretation, and waiting until the next day is not a viable option.
Aspiration of the fluid for the detection of organisms by Gram stain and cultures has also been suggested [85]. The presence of organisms, however, does not necessarily equate to a necrotizing infection and is not as reliable as taking deep tissue samples at the time of surgical exploration. Likewise, failure to obtain fluid is non-diagnostic and does not rule out necrotizing infection. Cultures take too long to make a timely diagnosis of NSTI.
The diagnosis of NSTI, therefore, must be made clinically and surgically. The clinical history and a meticulous physical examination are essential to establish an early suspicion of the disease. Clinical history and physical features that raise the suspicion of NSTI should prompt surgical exploration for a more definitive diagnosis and treatment. Indeed, the data support that a low threshold for operative diagnosis and acceptance of a high incidence of non-therapeutic operative intervention is necessary to optimize sensitivity and ensure that all patients received expeditious care.
Management
The management of NSTI requires aggressive resuscitation, IV antibiotic agents, complete surgical debridement, and supportive care. All aspects of treatment should be started promptly and simultaneously. The single most important aspect of managing NSTI is complete debridement of necrotic and infected tissues. Early operative debridement is the major determinant of outcome [64, 65]. Surgical debridement should never be delayed in the hope of restoring hemodynamic stability before anesthesia induction, because correction of the septic state will not occur until all of the infected and necrotic tissues have been removed.
Surgical management
When NSTI is suspected, surgical exploration is indicated. This involves making an incision over the inflamed and tender area and dissecting down to the fascia. A change in the fascia from a tough and shiny white appearance to a dull gray fascia that can be easily separated from the fat with blunt dissection is indicative of necrotizing infection: “The finger test.” The classically described brownish-tan “dishwater” fluid weeping from the tissues, if present, is also highly suggestive of NSTI. The underlying muscles should also be examined closely by making an incision in the fascia, whether or not the fascia appears normal. All necrotic fascia and muscles, as well as the overlying skin, should be excised. The excision margin should be healthy bleeding tissue.
The patient's ultimate outcome depends on the completeness of surgical debridement. This sometimes means amputation of the affected limb if there is extensive soft tissue loss preventing any reasonable functional recovery or if there is destruction of the major nerves and blood vessels. Under no circumstance should the wounds be closed at the time of surgical debridement, but rather packed for open drainage and re-exploration. Perineal gangrene often involves the scrotum and peri-anal skin. Surgical debridement usually involves excision of the scrotal skin and perineal skin extending to the gluteal region. The testicles are usually spared, and orchiectomy is required rarely.
After adequate surgical debridement, the patient's hemodynamic status should improve significantly. The patient's wound should be re-explored in the operating room within 24 hours to evaluate whether the spread of infection has been stopped and if further debridement is required. All newly identified necrotic tissue should be aggressively debrided. In patients whose clinical condition continues to deteriorate, re-exploration should be considered sooner, because there is a very high likelihood that the initial debridement is inadequate or the infection has spread even further. The goal of surgical therapy is complete debridement with the initial operation. It is not at all uncommon, however, that multiple debridements are required. In one study, 64% of the patients required at least one other debridement [69].
Surgical debridement is usually extensive and involves significant blood loss. Therefore, part of the pre-operative workup should include type and cross match for red blood cells. Many of these patients are coagulopathic, and efforts should be made to correct the coagulopathy to minimize blood loss. Patients are at risk for hypothermia, because a large surface area is often exposed and large areas of skin are excised.
Critical care management
As soon as the diagnosis of NSTI is suspected, immediate fluid resuscitation should begin. Many of these patients are hypovolemic and often have acute kidney injury. Aggressive initial fluid resuscitation will help restore intravascular volume, maintain adequate end-organ perfusion and tissue oxygenation, and limit the adverse effects of end-organ failure. The magnitude of resuscitation is dependent on the individual patient's physiologic status and should be targeted to provide adequate perfusion to the organs. For patients who are in shock or who have underlying cardiac or pulmonary disease, intravascular volume status requires monitoring.
Initial IV antibiotic therapy should be broad enough to cover the diverse and various causative agents (Table 4). High dose penicillin G or ampicillin should be used to cover for potential Clostridium, Streptococcus, and Peptostreptococcus infections. Penicillin G, if chosen, should be given as 18–24 million units per day for an adult. Anaerobes such as Bacteroides, Fusobacterium, and Peptostreptococcus should also be covered with clindamycin or metronidazole. Clindamycin is also effective in treating patients with group A β-hemolytic Streptococcus by suppressing the production of exotoxins [86]. Clindamycin is also the drug of choice for patients allergic to penicillin. Gram-negative coverage can be achieved by adding an aminoglycoside, a third or fourth generation cephalosporin, a fluoroquinolone, aztreonam, or a carbapenem. Alternatively, penicillin or ampicillin can be replaced by piperacillin-tazobactam to include gram-negative coverage.
Do not delay antibiotic administration if 1st priority drug not available; instead, begin with next highest priority drug and then give 1st priority drug as soon as possible.
IV = intravenous.
Selection of antimicrobials that inhibit toxin production should be considered in patients with streptococcal, Clostridium spp., and staphylococcal infections, especially those with evidence of rapidly progressive or severe infections. Clindamycin, erythromycin, or linezolid are potential inhibitory agents, provided that the pathogen is sensitive to the antibiotic. Protein cytotoxins play a significant role in the pathogenesis of staphylococcal infections [87]. Phenol-soluble modulin peptides are staphylococcal-secreted peptides that recruit, activate, and lyse human neutrophils, thereby eliminating a main cellular defense against staphylococcal infection [78]. The β-lactams actually enhance toxin production, while both clindamycin and linezolid inhibit toxin production by suppressing translation, but not transcription of S. aureus toxin genes and directly inhibiting synthesis of group A streptococcal toxins [87]. When patients exhibit signs and symptoms of shock, coagulopathy, and organ failure, antitoxin antimicrobials should be initiated promptly.
Because CA-MRSA necrotizing infections are more prevalent, parenteral anti-MRSA agents should be considered for use in the initial antibiotic regimen in suspected cases. Clinicians should also be aware that not only is there an increase in frequency of MRSA isolates but there is also a shift of the vancomycin minimum inhibitory concentration (MIC). In a study from Houston over a 7-year period, more than a third of MRSA isolates had a MIC greater than or equal to 1 mcg/mL, and nearly a third of isolates had a MIC of 2 mcg/mL [88]. Treatment failure rates for MRSA infections with increased MIC are reported [89, 90].
The antibiotic recommendation for Vibrio and Aeromonas infections is high dose combination therapy that includes a cell wall-active agent (third generation cephalosporins, carbapenems), plus doxycycline (protein synthesis inhibitor) [9].
When invasive mucormycos has been demonstrated, a lipid-based formulation of amphotericin B should be started (less nephrotoxicity than the conventional deoxycholate formulation, but invariably this still occurs especially those with risk factors). Echinocandins have no in vitro activity against the agents of mucormycosis; however certain species do express the target 1,3 beta-D-glucan synthase complex, and there is an in-vitro and observational data supporting the use of echinocandins in combination with amphotericin B for the treatment of these infections [91–93]. Posaconazole, which is a broad-spectrum azole agent with in vitro activity against the zygomycetes, may be considered for combination therapy with amphotericin B, or can be used as step-down therapy for patients who have responded to amphotericin B. It is rarely used as salvage therapy for those who do not respond to or cannot tolerate amphotericin B [94–96].
Antibiotic agents should be adjusted as early as possible to only cover the causative agents once they have been identified. The identification of causative agents and their antibiotic susceptibilities are key information obtained at the time of surgical debridement that will guide antimicrobial therapy.
Supportive care of the patient is extremely important. Nutrition support should be started as soon as the patient can tolerate it. If the patient can take food by mouth, it is the preferred route. If the patient is intubated or is unable to obtain adequate caloric intake orally, enteral feedings via nasogastric or nasoduodenal feeding tube is preferred over parenteral nutrition. When calculating total caloric requirement, a consideration should be given to the fact that these patients will have an increase in caloric and protein demands because of the large protein loss through the open wounds and the hypermetabolic state. Appropriate vitamins such as vitamins A and C and minerals such as zinc should be given to patients with large open wounds to facilitate wound healing. Rehabilitation should be started as soon as the patient is stable and able to participate. Early mobilization will help minimize pulmonary complications and de-conditioning.
Wound management
Once surgical debridement is no longer required, wound care can be performed at the bedside. Because these wounds are so extensive, patients usually require large doses of narcotics for dressing changes. Topical antimicrobial therapy is not necessary and is never a substitute for adequate surgical debridement. Agents such as silver nitrate and silver sulfadiazine will alter the appearance of the wound, making it difficult to be examined. Betadine should not be used on an open wound, because it will cause cell damage and inhibit wound healing. Perineal wounds are especially difficult to manage, because soilage of the wound is frequent. Stool diversion by colostomy is rarely required, however. Meticulous wound care is all that is required even with the most difficult wounds. When the wound is clean, use of a vacuum wound dressing is an option to facilitate wound granulation.
For the majority of the wounds, closure is achieved with simple split thickness skin grafts. More complex wounds should be managed in conjunction with the plastic surgery team. Wound coverage should be performed when the patient is medically stable and the wound is free from infection. It is not necessary to wait for granulation tissue to fill the entire wound bed for split thickness skin grafts, because the grafts will take as long as there is a clean and vascularized bed that is free from infection. Early coverage of the wound is advantageous in that it will help decrease pain associated with dressing changes and decrease metabolic demands.
For perineal wounds that involve the scrotum, the best cosmetic result can be achieved by delayed primary closure of the wound, if it is small. If the wound is too large for primary closure, it should not be allowed to heal by secondary intention because this will lead to contracture deformity of the scrotum. Several scrotal reconstruction methods have been described, including musculocutaneous flap and fasciocutaneous flaps from the thigh and the abdomen [97–99]. Direct split thickness skin grafts over the denuded testicles have also been described to provide good cosmetic and functional outcome, with the additional advantage of being a single stage operation [100,101]. A simple and widely used method is placement of the testicles in subcutaneous pockets in the thigh. It is functionally acceptable, but cosmetically sub-optimal. Many surgeons use this technique for temporary coverage, which can be revised later with other reconstructive methods [100].
Novel adjuncts
Hyperbaric oxygen therapy
Hyperbaric oxygen (HBO) therapy has also been proposed as an adjunctive therapy for NSTI. The HBO therapy involves the administration of oxygen (F
Should HBO be used in NSTI?
In patients with Type I NSTI, HBO may offer survival benefit (Table 5). Two systematic reviews were identified, both of which were unable to conduct summary estimates because of the poor quality of the studies, and thus could not provide generalized conclusions or recommendations [103, 104]. We identified a total of 12 (n = 12) contemporary observational trials, of which nine (n = 9)[105–113] studies were characterized as incorporating substantial, or being comprised completely of, cases of Type I NSTI [105–116]. Three of these trials [107–109] performed an analysis adjusted for differences in severity of illness and case mix, of which two [107,108] reported improved survival with the use of HBO; the third trial did not observe benefit [109]. Of the unadjusted trials, four reported survival benefit with HBO in uni-variable analysis. A total of 11 additional trials were identified, although not included because of either being of a case series study design (Table 4).
HBO = hyperbaric oxygen; NA = not available; ATM = atmospheres; UHC = __________; FG = Fournier gangrene; NF = necrotizing fasciitis; aOR = adjusted odds ratio; CI = confidence interval.
We did not identify any contemporary trials that focused on Type II NSTI. Three retrospective trials incorporated an identifiable population that was diagnosed with streptococcal infections, although significant differences in deaths were not observed [109,113,116]. We did not identify any contemporary trials that focused on Type III (clostridial) NSTI, although a single trial incorporated a small cohort (n = 5) with clostridial infections [109].
Recommendation:
Hyperbaric oxygen may be considered as an adjunct (i.e., secondary treatment) to therapy in cases of Type I (poly-microbial) NSTI, but should not delay the administration of antibiotic agents or expeditious operative debridement (weak, low).
Recommendation:
Hyperbaric oxygen is not recommended as an adjunct (i.e., secondary treatment) to therapy in cases of Type II (streptococcal) NSTI (weak, very low).
Recommendation:
Hyperbaric oxygen is not recommended as an adjunct (i.e., secondary treatment) to therapy in cases of Type III (clostridial) NSTI (weak, very low).
When should HBO be used?
There are little data to guide the timing of or criteria to institute HBO therapy. No identified contemporary study reported clinical indications, aside from a diagnosis of NTSI. Similarly, no study detailed or defined physiologic indications for instituting HBO therapy. One study reported that the greatest benefit was observed in patients with the highest degree of organ injury [107].
Recommendation:
The use of HBO should occur after the administration of antibiotic agents and operative intervention (weak, very low).
How should HBO be administered?
The reported protocols for the administration of HBO therapy varied considerably in administration regimen: Atmospheric pressure (range): 2.0–2.8 atmospheres (ATM); session duration (range): 30–90 minutes per session; number of sessions (range): 2–3 sessions per day; and duration of therapy (range): 1–26 treatments, 3–10 days, until infection resolved [103–116].
There are no data regarding a standardized duration of HBO therapy. Retrospective studies continued HBO therapy for a wide range of sessions/days, reporting in most circumstances that therapy was continued until “the infection resolved.”
Recommendation:
Hyperbaric oxygen should be instituted at approximately 2.5 ATM for 30–90 minutes per session, 2–3 sessions per day as tolerated (strong, low).
Recommendation:
Hyperbaric oxygen should be continued until source control is achieved and physiologic abnormalities are resolving (weak, low).
Are there risks of HBO?
HBO may cause acute brain oxygen toxicity, which presents with seizures. In large prospective trials of the application of HBO to a wide variety of medical conditions, the incidence of this complication was low, 0.03% [117]. A systematic review of HBO use, however, specifically in the context of wounds, reported an incidence of grand mal seizures of 0.7% (23/322) [103].
Pressure-induced (barotraumas) to the middle ear trauma is a recognized complication of HBO, particularly in the intubated patient [118]. In the vast majority of the cases, this barotrauma is self-limiting. Pressure-induced trauma to the inner ears, lungs, sinuses, and teeth has also been reported, although exceedingly rare [118].
Recommendation:
Standardized seizure management should be incorporated into the institutional HBO treatment protocol (strong, low).
Recommendation:
A myringostomy tube should be placed before HBO therapy for all patients receiving mechanical ventilation (strong, low)
IVIG
The use of IVIG for the management of NSTI has been advocated by some authors. The rationale for the use of IVIG is that IVIG provides antibodies that can neutralize the circulating streptococcal exotoxins, thus reducing the toxin-induced tissue necrosis [119,120]. In addition, IVIG may also have an effect on the circulating cytokines, thereby controlling the systemic inflammatory response. There are risks associated with the use of IVIG, including allergic reactions and acute kidney injury, although contemporary studies suggest these events are rare [121,122]. Although there are some retrospective as well as prospective studies showing a potential benefit in the use of IVIG in NSTI, additional studies are required before it can be recommended for routine use in NSTI [123–125].
Should IVIG be used in Type I (poly-microbial) or Type III (clostridial) NSTI?
There were no identified studies of the use of IVIG for Type I NSTI. In our expanded search that included all causes of sepsis, we identified six systematic reviews and meta-analyses of the use of IVIG (Table 5) [126–131]. A reduced risk of death was reported in each study; however, sensitivity analyses restricted to studies of low bias rendered estimates not statistically significant [126,127,129,131].
Only four contemporary placebo-controlled RCT of IVIG for severe sepsis or septic shock were identified, of which none reported a significant reduction in death [122,132–134]. In one sub-group analysis, patients on appropriate antibiotics and who received IVIG exhibited a reduced risk of death [133]. The study by Werdan et al. [122] reported reduced Acute Physiology and Chronic Health Evaluation II score and duration of mechanical ventilation [122].
Seven contemporary retrospective analyses [135–140] were identified, of which three adjusted for differences in severity of illness [135–137]. Only one reported a reduced risk of death [137], though none of these three studies observed differences in catecholamine use, vasopressor-free, ventilator-free days or hospital length of stay [135–137].
Recommendation:
We do not recommend the use of IVIG in cases of Type I or Type III NSTI even in the setting of severe sepsis or septic shock (strong, moderate).
Should IVIG be used in Type II (streptococcal) NSTI?
IVIG may offer survival benefit in patients with Type II NSTI and streptococcal toxic shock syndrome (Tables 6 and 7). We identified one multi-center, double blind, randomized, placebo-controlled trial of IVIG for streptococcal toxic shock syndrome (STSS) [125]. Although IVIG was associated with a reduced risk of death, this did not attain statistical significance. The IVIG was associated with a more rapid resolution of shock and organ failure, however, as defined by Sequential Organ Failure Assessment (SOFA) score [125]. We identified a total of three contemporary prospective observational or national surveillance trials, which focused on GAS infections or STSS [124,141,142]. Two trials adjusted for differences in severity of illness and case mix, and both reported increased adjusted odds of survival with IVIG [124,142]. All studies are limited by relatively low cohort size (N = 21–67 subjects) (Table 6).
IVIG = intravenous immunoglobulin; RCT = randomized controlled trial; STSS = streptococcal toxic shock syndrome; GAS = group A Streptococcus; OR = odds ratio; aOR = adjusted odds ratio; IgM = immunoglobulin M; IgA = immunoglobulin A.
A “probable” case meets the clinical case definition in the absence of another identified etiology for illness and with isolation of group A Streptococcus from a non-sterile site.
A “confirmed” case meets the clinical case definition and with isolation of group A Streptococcus from a normal sterile site (e.g., blood or cerebrospinal fluid or joint, pleural or pericardial fluid.
SBP = systolic blood pressure.
Recommendation:
We recommend that IVIG be considered as an adjunct to therapy in cases of Type II (streptococcal) NSTI (strong, moderate).
When should IVIG be used?
Three of the four studies specifically focused on GAS incorporated patients meeting criteria for the diagnosis of toxic shock syndrome (Table 7) [143].
Recommendation:
We recommend the use of IVIG for cases of Type II (STSS) that meet TSS criteria (strong, moderate).
How should IVIG should be dosed and administered?
There is considerable batch-to-batch variation of IVIG in terms of the quantity of neutralizing antibodies, and Level I evidence is lacking. Studies of immunoglobulin for the management of GAS and STSS used poly-clonal IVIG. Initial doses ranged from 0.5–1.0 g/kg daily for up to six days [124,125,141,142].
Recommendation:
In cases of GAS and STSS, we recommend a dose of poly-clonal IVIG of 0.5–1.0 g/kg per day for no more than five days (strong, moderate).
Blood purification (plasmapheresis, plasma exchange)
Blood purification incorporates a host of varying interventions aimed at removing a variety of mediators purported as causal in the pathophysiology of NSTI and sepsis.
Should blood purification be used in NSTI?
We did not identify any studies of the use of blood purification for any type of NSTI (Table 8).
RR = relative risk; PMX = polymixin; HP = hemoperfusion; SOFA = Sequential Organ Failure Assessment; RCT = randomized controlled trial; HR = hazard ratio; aHR = adjusted hazard ratio; KM = Kaplan Meier; HF = hemofiltration; CCRT = ________; MRSA = methicillin resistant Staphylococcus aureus; HD = hemodialysis; CVVH = continuous venovenous hemofiltration; CVVHDF = continuous venovenous hemodiafiltration; PE = plasmapheresis; LPS = lipopolysaccharide; CPFA = coupled plasma filtration and adsorption; DHP = direct hemoperfusion; PMX = polymyxin B; PMMA = polymethylmethacrylate; PAN = polyacrylonitrile; CHF = continuous hemofiltration; CHDF = continuous hemodiafiltration.
Three meta-analyses evaluated the use of blood purification in patients with sepsis, severe sepsis, and septic shock [144–146]. Two trials identified a reduced risk of death: 0.69 (0.56–0.84) [144] and 0.63 (0.42–0.96) [145]. The former trial included 16 studies and conducted sensitivity analyses of each distinct mechanism of blood purification [144]. This trial observed a loss of statistical significance with hemoperfusion in the absence of polymixin B (PMX B), endotoxin-adsorbing columns [144]. A summary estimate of the two included trials of plasma exchange remained significant: 0.63 (0.42–0.96) [144]. The remaining meta-analysis (n = 3 studies) of high volume hemofiltration was unable to pool estimates because of study heterogeneity [146].
We identified 15 contemporary RCTs, of which only two reported a significant reduction in death [147–161]. The Use of Polymyxin B Hemoperfusion in Abdominal Sepsis (EUPHAS) trial demonstrated improved 28-day survival using hemoperfusion and PMX B: aHR 0.36 (0.16–0.80) [147], as did the study of Nemoto et al. [148]. The EUPHAS investigators also reported improved SOFA scores [147]. Of the remaining RCTs (n = 13), a variety of blood purification methods were used, yet no study observed a significant reduction in death.
We also identified nine observational trials that we did not include in the generation of recommendations because of the substantial data derived from RCT and meta-analyses (Table 8).
Recommendation:
In patients with NSTI and sepsis, severe sepsis, or septic shock, hemoperfusion with PMX B may be considered (strong, moderate).
Recommendation:
In patients with NSTI and sepsis, severe sepsis, or septic shock, plasma exchange may be considered (weak, low).
Recommendation:
In patients with NSTI, we do not recommend hemoperfusion without PMX B, hemofiltration, or hemodialysis (strong, moderate).
When should blood purification be used?
The majority of studies evaluated subjects with severe sepsis or septic shock. In the meta-analysis of Zhou et al. [144], however, a sensitivity analysis suggested a greater reduction in death if blood purification is administered during sepsis, rather than in severe sepsis or septic shock: 0.40 (0.26–0.64).
Recommendation:
In patients with NSTI, we recommend the use of adjuvant blood purification early and before the development of septic shock (weak, high).
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.