
Abstract
Abstract
Background:
Hospital-acquired infections (HAI) in trauma patients increase inpatient morbidity and mortality. However, their impact on long-term mortality is not well understood.
Patients and Methods:
A retrospective trauma registry analysis of all patients admitted to an academic level I trauma center between July 1, 2008 and December 31, 2012 was performed. Patients included survived to discharge and were 18 years of age or older. Age, gender, Injury Severity Score (ISS), ventilator use, history of chronic obstructive pulmonary disease (COPD), and HAI were reviewed. Name, social security number, and date of birth were used to extract National Death Index data from 2008–2013 for an outcome of mortality after discharge, time to death, and cause of death. Unadjusted logistic regression was performed. Multiple logistic regression was used to adjust for patient and injury characteristics and to determine odds of mortality in the post-discharge period.
Results:
A total of 8,275 patients met inclusion criteria; 65.4% were male and the median age was 47. The mean ISS was 11 ± 8.9. Nine hundred seventeen patients (11.1%) died after discharge; 4.8% of patients had hospital-acquired pneumonia (HAP) and 4.2% had a urinary tract infection (UTI). The unadjusted odds ratio (OR) of mortality after discharge in patients who had pneumonia and UTI were 1.77 (1.35, 2.31, p < 0.001) and 2.44 (1.87, 3.17, p < 0.001), respectively. After adjusting for patient age, gender, ISS, ventilator use, and history of COPD (pneumonia patients only), the odds for mortality after discharge remained significant for pneumonia (OR = 1.57 (1.09, 2.23), p = 0.013) but not for UTI (OR = 1.25 (0.93, 1.68), p = 0.147). The top causes of death after discharge in patients with HAP were COPD (11.4%) and falls (7.1%).
Conclusions:
Trauma patients with HAP have higher mortality after hospital discharge. Prevention strategies for HAP including pulmonary toilet, early mobility, pain control, and early extubation must be a priority. Unfortunately, patients who develop pneumonia may have a decreased reserve, or ability to recover from their traumatic injuries and HAI. Further characterization of HAP and its subsequent treatment strategies are needed.
T
It is essential to identify whether the low inpatient mortality rate among trauma patients persists beyond acute care management and hospital stay, and whether factors such as in-hospital infection correlate with post-discharge mortality. In one large study of long-term trauma mortality, the following factors were identified as predictive of death in the year after injury: advanced age, male gender, hypotension in the emergency department, Glasgow Coma Scale score <9 with injury sustained from blunt trauma or fall. This study was the largest done to our knowledge to assess long-term mortality in trauma patients [2]. However, there is still a large gap in knowledge because these results may not be representative of all trauma patients, particularly in parts of the country that include both rural and urban populations [3].
Among the trauma population, hospital-acquired infections (HAI) have been associated with increased inpatient mortality, cost, and length of stay [4]. Furthermore, higher rates of mortality and complications after discharge among elderly trauma patients (aged 65 and above) have been identified [2,5,6]. The elderly comprise approximately 5% of the major trauma population, and represent a distinct subset of injured patients, particularly as the aging population continues to increase [7].
It is clear that there are subsets of the trauma patient population who are likely at higher risk for mortality despite inpatient survival. However, this relationship is not well understood beyond weeks after discharge. Quantifying the burden of trauma mortality can help guide the allocation of trauma care resources, provide better care, and avoid preventable factors that increase risk of morbidity and mortality, in addition to improving cost effectiveness at acute care centers nationwide. This study is one of the largest in sample size and length of follow-up to evaluate trauma mortality. We hypothesized that trauma patients with hospital-acquired infections (pneumonia and urinary tract infection [UTI]) are at higher risk for post-discharge mortality.
Patients and Methods
The database was created by merging the Epic Systems™ electronic health record (EHR) based Carilion Roanoke Memorial Hospital (CRMH) Trauma Registry with the National Death Index (NDI). The trauma registry is collected prospectively, and includes more than 100 individual patient data points such as age, gender, payer status, and pre-existing conditions. This registry is used currently as the primary basis for informing quality improvement initiatives, resource tracking, research, and planning at CRMH. Furthermore, the trauma registry is submitted to the Virginia Statewide Trauma Registry (VSTR) and the National Trauma Data Bank (NTDB) to advance trauma research locally and nationally. This data is also used to develop injury prevention programs and allow for performance comparison at the state and national levels. The NDI is a publically available, centralized database of death record information on file in state vital statistics offices. The NDI has shown at least 87% sensitivity and specificity when used to assess mortality [8,9].
Patients 18 years of age and older, seen at CRMH between July 1, 2008 and December 31, 2012 were included in the study. The NDI was used to verify dead or alive status after discharge among trauma patients between the years 2008 and 2013. Each patient had mortality outcomes followed for at least one year after discharge and up to five years through the year 2013. Trauma registry patients were matched with mortality outcome (dead/alive, date of death, and cause of death) by their full name, date of birth, and social security number. Patients who could not be matched for outcomes by the NDI were also excluded from the study. This study was approved by the Carilion Roanoke Memorial Hospital Institutional Review Board (IRB). A p value <0.5 was considered statistically significant.
A diagnosis of pneumonia or UTI was cross-referenced with cultures and the hospital pharmacy database for antibiotic usage in order to be included in the trauma registry. Descriptive characteristics of all trauma patients were evaluate and include factors such as: age; gender; ethnicity; body mass index (BMI); Injury Severity Score (ISS; mild, low, moderate, severe); ventilator status; mechanism of injury; length of stay; Glasgow Coma Scale (GCS) score; and number of pre-existing conditions (i.e., hypertension, diabetes, liver disease; Table 1). Patients with pre-existing conditions were stratified by number of pre-existing conditions (0,1, 2 or greater) [10].
Baseline group for the given metric.
Significant at 0.05 level of significant.
BMI = body mass index; ISS = Injury Severity Score; GCS = Glasgow Coma Scale.
Further analysis was stratified based on in-hospital pneumonia or UTI mortality and survival after discharge using the descriptive characteristics described above. Three different tests were used for descriptive analysis. For categorical parameters with cell frequencies greater than 5, χ2 test was used, in all other cases, the Fisher exact test was used. For continuous parameters, a two-sample Student t test with unequal variance assumption was used.
Univariate analysis evaluated risk for post-discharge mortality in patients with a complication of in-hospital pneumonia or UTI. A stepwise logistic regression model was used to identify all significant parameters from the dataset (described in Table 1). A significance level of 0.3 was required to allow a parameter into the model, and a significance level of 0.35 was required for a parameter to stay in the model. The final model was cross-validated with the hypothesis that hospital-acquired infections (pneumonia and UTI) and specific patient and injury characteristics may be associated with inpatient mortality to build the final multiple logistic regression model. Multiple logistic regression was used to adjust for patient age, gender, ISS, ventilator use in both groups in addition to history of COPD in patients with pneumonia. Kaplan-Meier survival analysis was conducted to evaluate patient survival [11]. The log rank test, which places more weight on longer survival times, and the Wilcoxon test, which places more weight on early survival times were used to test for homogeneity in survival outcomes analysis.
Results
A total of 9,596 patients were admitted to the trauma service between July 1, 2008 and December 31, 2012. Of these patients, 8,716 were age 18 or older at admission; 8,281 met our inclusion criteria, giving an overall inpatient morality rate of 4.9%. After data were matched by the NDI, the final study sample size was 8,275 patients (Fig. 1). There were six patients excluded because of insufficient NDI match results. Approximately 65.4% of the population was male, and 85.3% were white. The median age was 47. The mean ISS was 11 ± 8.9, which falls into the moderate category (Table 1). The overall inpatient mortality was 493 patients (4.9%). There were 917 patients (11.1%) who were reported to have died after discharge. Of the study population, pneumonia and UTI were the most common in-hospital complications. There were 399 (4.8%) patients who had pneumonia and 348 (4.2%) that had a UTI, who were discharged alive.

Study inclusion criteria.
Pneumonia
When evaluating patients who had in-hospital pneumonia, 15.3% (72/471) of patients died in the hospital. There was no significant difference between gender or ISS. Patients who died were more likely to be obese, BMI >30 (p = 0.001). Patients who died were more likely to be age 65 and older (p = 0.001), and the median age for those in the age ≥65 category discharged alive was 80.39 compared with those who died in-patient (75.02). The average length of stay in patients who were discharged alive was significantly longer than those who died (30.33 ± 23.58 versus 14.39 ± 9.81, p < 0.001). See Table 2 for complete results.
baseline group for the given metric.
one of the cell frequencies is 0.
significant at 0.05 level of significance.
BMI = body mass index; ISS = Injury Severity Score.
In patients with pneumonia who were discharged alive, there was no substantial long-term survival difference by gender or race. In both age groups, patients who died were older (51.30 versus 41.52 y, p = 0.001, and 77.36 versus 73.10 years, p = 0.004). Patients who were obese continued to be at increased risk for death compared with all other BMI categories (p = 0.009). Patients who had an ISS of 16–24 (severe) and >24 (very severe) were also at increased risk of death, despite being discharged alive and not demonstrating this correlation between ISS and survival in the inpatient setting. See Table 3 for complete results.
Baseline group for the given metric.
One of the cell frequencies is zero.
Significant at 0.05 level of significant.
BMI = body mass index; ISS = Injury Severity Score; GCS = Glasgow Coma Scale.
Urinary Tract Infection
Similarly, in patients with an in-hospital UTI, there was no difference by gender or race. The average age for those that were discharged alive was younger in both age groups (43.29 vs 45.75, p = 0.0010; 78.67 vs 83.08, p = 0.008). There was no difference in survival based on BMI, or hospital length of stay in this group. Patients who were on the ventilator in the hospital setting had increased risk of death after discharge compared with those not on the ventilator (p = 0.0177). See Table 4 for complete results.
baseline group for the given metric.
one of the cell frequencies is 0.
significant at 0.05 level of significance.
BMI = body mass index; ISS = Injury Severity Score.
In patients with UTI who were discharged alive, there was no long-term survival significant difference by gender or race. In the younger age group, patients who died were significantly older (53.45 versus 41.94 y, p = 0.0003, but patient survival in the older group was comparable, the average age for those discharged alive was 78.13 compared with 79.67 in those who died (p = 0.2302). Patients who were underweight were at increased risk for death compared with all other BMI categories (p = 0.007). Patients who had an ISS of >24 (very severe) were also at increased risk of death, despite being discharged alive, which was also demonstrated in the inpatient setting. See Table 5 for complete results.
Baseline group for the given metric.
One of the cell frequencies is zero.
Significant at 0.05 level of significance.
BMI = body mass index; ISS = Injury Severity Score; GCS = Glasgow Coma Scale.
Logistic regression
The unadjusted odds of mortality in patients with HAP was 1.77 [1.35, 2.31] times higher than those who did not have pneumonia (p < 0.001). Patients with UTI were 2.44 [1.87, 3.17] times more likely to die after discharge (p < 0.001). However, on multiple logistic regression only pneumonia held a significant predictor of increased long-term mortality (Table 6). The top causes of death after discharge in patients with HAP were chronic COPD in 11.4% and falls (7.1%).
Adjusted for patient age, gender, ISS, ventilator use, and history of COPD (pneumonia patients only).
ISS = Injury Severity Score; COPD = chronic obstructive pulmonary disease.
Kaplan-Meier survival analysis
The Kaplan-Meier survival analysis similarly showed that the survival time for patients with or without UTIs do not statistically differ. The rank tests for homogeneity did not indicate a significant difference between the strata (p = 0.3266 for the log-rank test and p = 0.1837 for the Wilcoxon test, Fig. 2). However, patients with pneumonia survived shorter than those without in-hospital pneumonia. This difference was evident within 30 days of discharge and remained evident through 1,500 days post-hospital discharge. The rank tests for homogeneity indicated a significant difference between the strata (p = 0.0218 for the log-rank test and p = 0.0050 for the Wilcoxon test; Fig. 3).
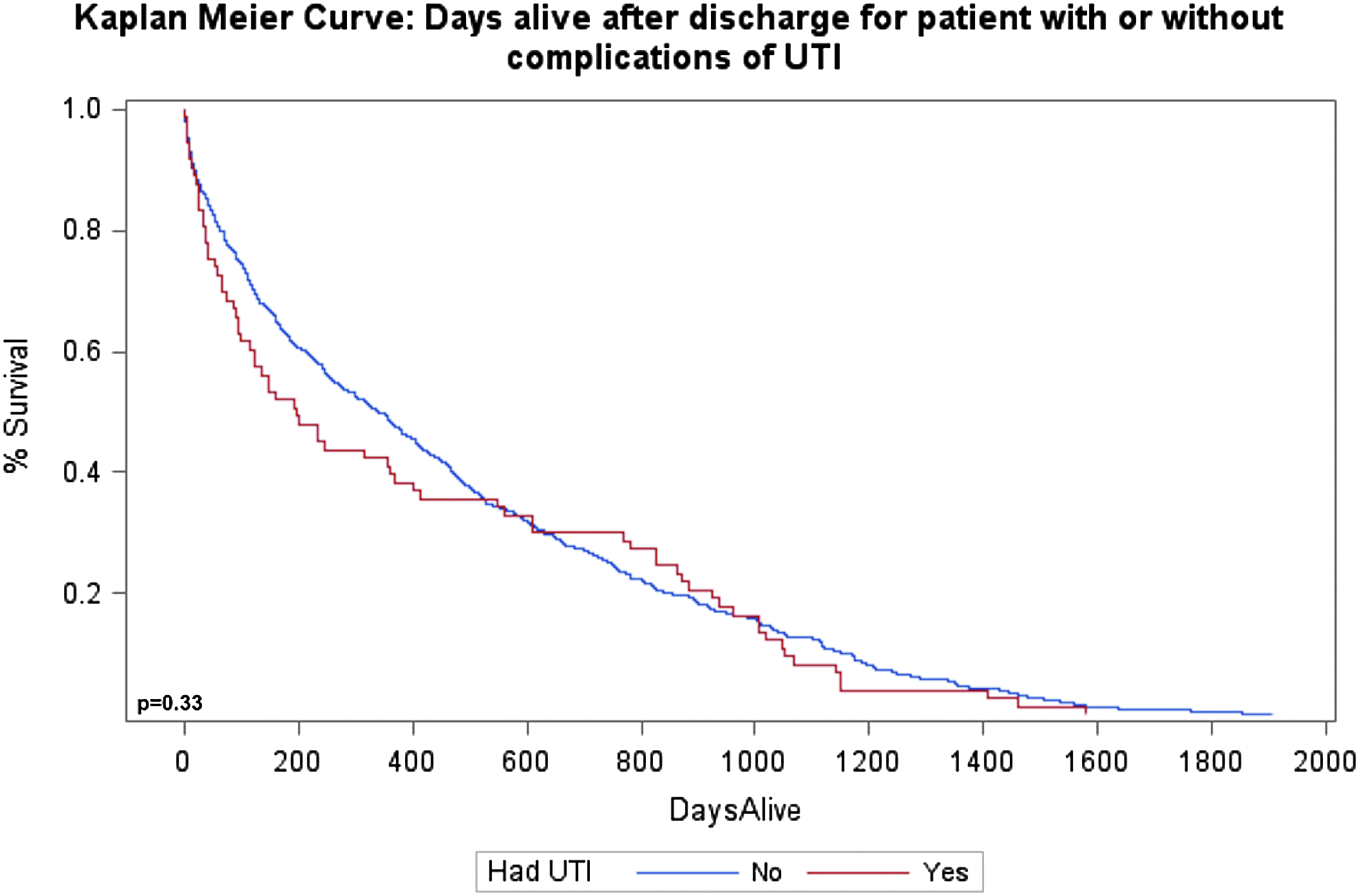
Kaplan-Meier plot: days alive after discharge for patients with or without complications of urinary tract infection (UTI).

Kaplan-Meier plot: days alive after discharge for patients with or without complications of pneumonia.
Discussion
This study was a retrospective analysis to evaluate the impact of HAIs on long-term mortality in trauma patients. Prior studies have shown that trauma-related mortality is the leading cause of post-discharge mortality through one year after discharge [12]. Ours was one of the largest studies of its kind done to date, and encompassed mortality outcomes of up to five years beyond hospital discharge. Our findings indicate that HAP increased patient risk for long-term mortality, although this relation was not observed in patients who had hospital-acquired UTIs.
Interestingly, elderly patients were most at risk for poor outcomes after HAP. This suggests there may be a component of frailty that plays a role in the ability to recover from a traumatic injury, or a decreased reserve to improve after a hospital acquired infection, which then acts as a second insult. Patients who were intubated and placed on the ventilator had worse outcomes in both pneumonia and UTI groups. Patients that are placed on a ventilator are a subset that overall have a more severe injury burden, requiring intensive care unit care (ICU). Prior literature has also shown that ICU stay worsens long-term trauma mortality outcomes, and is worse in mechanically ventilated patients [13,14]. Similarly, the ISS in patients with pneumonia also reflected that a decline in reserve, represented by a severe or very severe injury greatly increased risk for mortality, even after being discharged alive after hospital stay for a traumatic injury.
In a previous study of post-discharge mortality among trauma patients at a level I center, it was found that lack of insurance and government insurance status were associated with statistically significantly increased risk of two-year mortality after discharge [15]. It was also noted that discharge disposition among the elderly varies, and is influenced by insurance status as well as socioeconomic status [16,17]. This implies that age and access to care show a potentially multiplicative correlation with inpatient mortality. Hence, it is possible that in the post-discharge setting, there may be an even more apparent disparity in outcomes, which needs to be explored further.
Finally, patients with increased comorbidies had worse outcomes in patients with pneumonia as well as those with UTI. This further supports that patients with less reserve (i.e., those with additional co-existing medical problems) are at a disadvantage in their ability to recover after trauma. When specifically looking at obese patients who had pneumonia, these patients did worse compared with those who had a BMI <30. This may be explained by poorer mobility leading to an increased likelihood of atelectasis and development of pneumonia.
There are challenges to doing a project of this magnitude. In order to evaluate long-term outcomes, patients who could not be matched by the NDI criteria were not included in our analysis. However, this number was less than 0.01% of the total number of patients admitted within our study dates. Using the NDI database was unique in that it allowed us to identify causes of death in our study population, and gain insight into patient diagnoses that were linked with death after discharge. Additionally, because our study was a retrospective analysis, we were not able to assess quality of life in patients. This is significant, because survival after traumatic injury and HAI does not translate to a comparable quality of life. Assessing quality adjusted life years (QALYs) may be beneficial to incorporate into future research. Furthermore, parameters such as blood stream infections (BSI) or surgical site infections were not represented as robust parameters in our dataset, and therefore, the two most common infections (pneumonia and UTI) were analyzed. Recording of BSI and surgical site infections in the trauma registry will be improved upon for analysis in future studies.
This study enumerated the long-term trauma mortality rate at a level I trauma center. By identifying certain populations that may face a disparate risk for premature death after discharge, we aimed to identify potential disparities that may exist in long-term mortality, and inform policy changes both locally and at the national level about longevity among trauma patients and preventable causes of “earlier than expected” trauma-related mortality after hospital discharge. Our results characterized a population with less reserve (higher rates of comorbidities and ISS) or those who were frail (elderly) as being at increased risk for long-term mortality after discharge. Even after adjusting for factors associated with worse outcome (age, gender, ISS, ventilator use, and history of COPD), pneumonia still held true as a risk factor for increased mortality after discharge. Thus, pneumonia likely represents an independent parameter, particularly in the subset of patients who are frail and are unable to recover from this complication.
Further research is needed to characterize potential areas of focus for reducing hospital-acquired infections. Currently, there is a large focus on preventing catheter-associated urinary tract infections (CAUTI) in the hospital setting. However, as these patients have demonstrated equivalent risk for mortality, it may be a more effective use of resources to reduce HAP, as there was a continued risk of mortality over our five-year study follow-up. For example, there is emphasis on increasing early mobility, pain control, and pulmonary toilet while patients are hospitalized, however, this does not persist to the same degree after patients are discharged. Thus, it is important to address continuing pneumonia prevention measures through patient education prior to discharge.
This analysis showed that of the two most common HAIs studied, pneumonia increased patient risk for mortality in the inpatient setting and by greater than 50% in the five-year study period compared with trauma patients who did not develop pneumonia. Pneumonia prevention in trauma patients, particularly in those who are believed to have decreased reserve as a result of additive patient or injury factors, is essential for improving outcomes after discharge.
Footnotes
Author Disclosure Statement
No competing financial interests exist.