
Abstract
Abstract
Background:
The effect of smoking on the risk of surgical site infection (SSI) after spinal surgery remains controversial. Therefore, we conducted a meta-analysis to determine whether there is an association between smoking and the risk of SSI and to calculate the relative risk of infections attributable to smoking.
Methods:
We performed a literature search of cohort and case-control studies in the MEDLINE, Embase, and ISI Web of Science databases. Sensitivity and subgroup analyses were performed to test the robustness of overall estimates of risk and to investigate potential sources of heterogeneity. We further calculated the population-attributable fraction (PAF) to evaluate the proportion of SSIs associated with smoking.
Results:
In total, 26 independent observational studies involving 67,405 patients who underwent spinal surgery were analyzed. Smokers had a significantly higher risk of SSI than did nonsmokers (odds ratio [OR] 1.26; 95% confidence interval [CI] 1.05–1.51). Subgroup analysis according to the study design revealed an apparent association between smoking and SSI in the cohort subgroup (OR 1.40; 95% CI 1.17–1.66), but not in the case-control subgroup (OR 0.99; 95% CI 0.64–1.53). After evaluation of the PAF, the proportion of SSIs associated with smoking increased to 10.37%.
Conclusions:
This meta-analysis demonstrated that smoking increases the risk of SSI after spinal surgery. False-negative associations in other studies may have resulted from defects in the study design. However, because of the heterogeneity among the studies in the present meta-analysis, the results should be interpreted with caution.
S
Smoking has been demonstrated to be a risk factor for numerous diseases, such as cancer [4,5] and cardiovascular disease [6]. In recent years, a growing literature has demonstrated that smoking encourages post-operative complications. Smokers who undergo surgery have longer hospital stays, a higher risk of re-admission, and a higher risk of in-hospital death than do nonsmokers [7–9].
Some studies in the past decade have examined the association between pre-operative smoking and the risk of incision infection after spinal surgery. However, their conclusions are inconsistent: Some found no association [10,11], whereas some observed an obviously high risk of post-operative infection among patients who smoke [12,13]. A meta-analysis was recently conducted by Gronkjaer et al. [9], and they concluded that pre-operative smoking was associated with a higher risk of post-operative complications, including incision problems. In their study, infections, as one type of post-operative complication, were mixed together with incision necrosis, delayed healing, dehiscence, and hernia. However, different complications may have different mechanisms; thus, studies of SSI that combine SSI with other complications could reveal a diminished overall association between smoking and the outcome of interest. Additionally, the meta-analysis by Gronkjaer et al. [9] analyzed various types of operations together, including abdominal, breast, oral/dental, thoracic, plastic surgery, and others, but few studies in the meta-analysis involved spinal surgery.
To the best of our knowledge, no meta-analysis has assessed comprehensively the association between pre-operative smoking and the risk of SSI after spinal surgery. Thus, we performed the present systematic review and meta-analysis to estimate the link between smoking and the risk of SSI and to calculate the relative risk of infections attributable to smoking.
Materials and Methods
Literature search
This meta-analysis was performed in accordance with the Meta-analysis of Observational Studies in Epidemiology (MOOSE) statement [14]. The MEDLINE (via PubMed), Embase, and ISI Web of Science electronic databases were searched from inception to 1 June 2016 using the MeSH terms “smoking,” “risk factors,” “surgical wound infection,” “spine,” and their corresponding free terms. The search was restricted to human subjects and the English language. Articles retrieved by these searches and relevant references cited in those articles also were searched to identify other potentially eligible studies.
Study selection
The following inclusion criteria were used: (1) The study design was cohort or case-control; (2) the study population comprised patients who underwent spinal surgery including the cervical, thoracic, lumbar, and sacral vertebrae; (3) the study contained enough information to extract or calculate the odds ratios (ORs) of smoking correlated with SSI. For accepted articles that reported on the same population or subpopulation, the most informative article or complete study was used to avoid duplication of information.
Data extraction
Data were extracted independently by two investigators and checked by the other authors, and any discrepancies were resolved by consensus. The following information was abstracted from all accepted publications: Name of first author, year, country, study design, number of patients in infected and uninfected groups, site of surgery, surgical procedure, and definition and types of infection. The ORs and their respective 95% confidence intervals (CIs) were either retrieved directly from the article or calculated from available data. When available, the most comprehensively adjusted estimates were used.
Smoking states were defined as “ever,” “current,” or “former.” Both “current” and “former” smokers were regarded as “ever” smokers. According to the SSI definition put forth by the U.S. Centers for Disease Control and Prevention, SSIs included superficial incision infection, deep incision infection, and organ space infection [15].
Methodological quality
We applied the Newcastle–Ottawa Scale (NOS) to evaluate the reporting rigor of observational studies [16]. The NOS is a scoring checklist that addresses issues of design and implementation of a cohort or case-control study, including issues of participant selection, comparability of cases and controls, exposure, and outcomes. Studies awarded six or more stars were considered to be high-quality and were analyzed.
Statistical analysis
Odds ratios and 95% CIs were used to assess the relation between smoking and the risk of SSI. Estimates were calculated using a random-effects model except where otherwise specified because significant heterogeneity was anticipated across studies, and the results of a random-effects model usually are more conservative than those of a fixed-effect model. The distribution of ORs and 95% CIs was represented using Forest plots. The Cochran Q test was used to estimate the p value for heterogeneity. The I2 statistic also was calculated to assess heterogeneity across studies using the following interpretation: I2 <50% indicated low heterogeneity, I2 50%–75% indicated moderate heterogeneity, and I2 >75% indicated high heterogeneity. Sensitivity analyses were performed to test the robustness of overall estimates. Subgroup analyses also were performed to investigate potential sources of heterogeneity.
The population-attributable fraction (PAF) (i.e., the reduction in risk if smoking was eliminated) was calculated as follows: {prevalence of smoking × (OR − 1)/[prevalence of smoking × (OR − 1) + 1]}, where OR indicates the pooled ORs [17]. The prevalence of smoking was estimated on the basis of a population-based cohort study with a sample size >20,000 [18].
Publication bias was assessed with a funnel plot and a combination of the Begg and Egger tests. STATA version 11.0 (StataCorp, College Station, TX) was used for all analyses. All statistical tests were two-sided, and p values of <0.05 were considered statistically significant.
Results
Literature search
In total, 1,524 citations were retrieved using the above-described search strategy. Of these, 532 records were duplicates. After a review of the titles and abstracts, 922 articles were deemed irrelevant, and 70 were considered of interest; the full text of these 70 articles was retrieved for detailed evaluation. Forty-four articles were excluded, so 26 articles were ultimately included in the meta-analysis [19–24,11,25–29,10,18,13,30–38,12,39] (Fig. 1).

Flow chart illustrating results of search strategy.
Study characteristics
The 26 independent observational studies included in this meta-analysis were published from 1999 to 2016 and included a total of 67,405 individuals. Of the studies, 15 were cohort studies and 11 were case-control. Four studies investigated the lumbar spine, two investigated the sacrum, two investigated both the thoracic and lumbar spine, and the remaining 18 investigated the entire spine. Eighteen studies were conducted in the United States and three in Japan. The other five were conducted in China, France, The Netherlands, Korea, and Singapore.
Adjusted ORs were provided in five studies, and crude ORs were extracted from the other 21 studies. Sixteen studies defined infection using the U.S. Centers for Disease Control and Prevention definitions [15]. Two studies investigated spinal injury, and two studies investigated sacral surgery. According to the NOS scale, 10 studies were awarded eight stars, six were awarded seven stars, and 10 were awarded six stars.
The spinal infection rate among the 11 cohort studies was 3.01%, and the lumbar spinal infection rate was 2.16%. Detailed information on the study characteristics is shown in Table 1.
CDC = U.S. Center for Disease Control and Prevention; CI = confidence interval; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification procedure codes; NOS = Newcastle-Ottawa Scale; NR = not reported; OR = odds ratio.
Smoking and risk of SSI
Overall, smoking was associated with a significantly greater risk of developing SSI (OR 1.26; 95% CI 1.05–1.51). There was evidence of moderate heterogeneity in the ORs across these studies (I2 = 52.4%; p = 0.001) (Fig. 2). The OR did not change after analyses with the fixed-effects models. Sensitivity analysis, in which the meta-analyses were repeated serially after exclusion of each study, showed that the OR ranged from 1.20 to 1.33, but no individual study affected the difference in the overall OR.
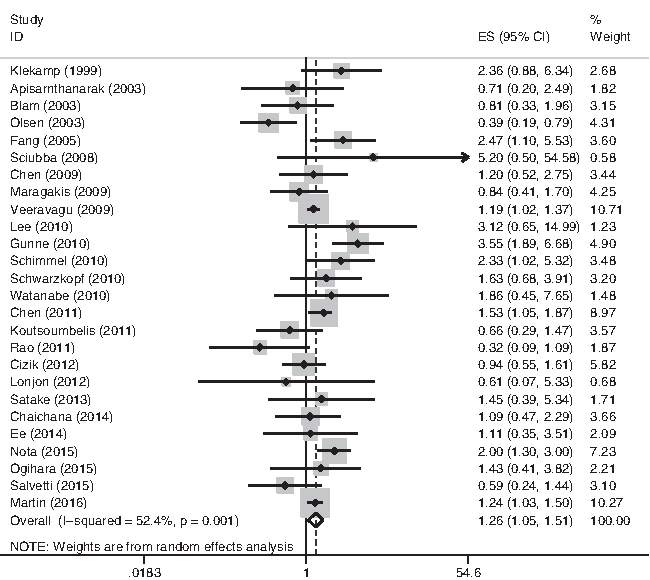
Forest plot of association between smoking and surgical site infection. Random-effect model was used to estimate summarized odds ratios.
Among the studies, two reported spinal injury [20,29], two focused on the sacral vertebrae [38,22], two analyzed a small population [38,22], and three did not clearly define infection [25,29,34]. After serial exclusion of these studies, the combined ORs were not changed materially, but moderate heterogeneity was still present. When we pooled the cohort studies or studies with adjusted estimates, the heterogeneity among the studies decreased to a low degree without a material change in the combined ORs (Table 2).
Sample size is more than 10,000.
Sample size is less than 50.
CIs = confidence intervals; ORs = odds ratios.
The funnel plot for publication bias in Figure 3 showed a symmetrical distribution of the published studies. Neither the Egger nor the Begg test showed evidence of significant publication bias (Egger p = 0.99; Begg p = 0.98).
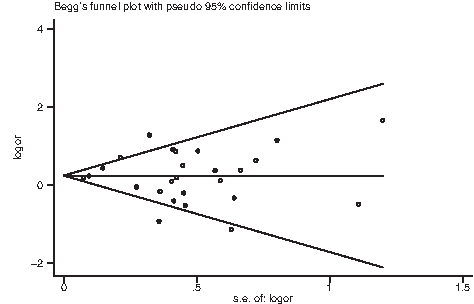
Funnel plots showing associations between smoking and surgical site infection.
Subgroup analysis
We performed stratified analyses across a number of key study characteristics and clinical features to explore study heterogeneity. The type of study, definition of infection, multiple adjusted estimates, and sample size were not significant sources of heterogeneity. When the studies were stratified by type, the p value showed no statistical significance in the case-control subgroup, but there was a significant association between smoking and SSI (OR 1.40; 95% CI 1.17–1.66) with low heterogeneity (I2 = 38.2%; p = 0.07) in the cohort subgroup (Fig. 4). Similarly, when the studies were stratified by adjusted estimate, there was a significant association between smoking and SSI (OR 1.50; 95% CI 1.08–2.09) with low heterogeneity (I2 = 48.4%; p = 0.10) in studies with multiple adjusted estimates, although the pooled estimates without adjustment showed no significant association between smoking and SSI (Table 3).
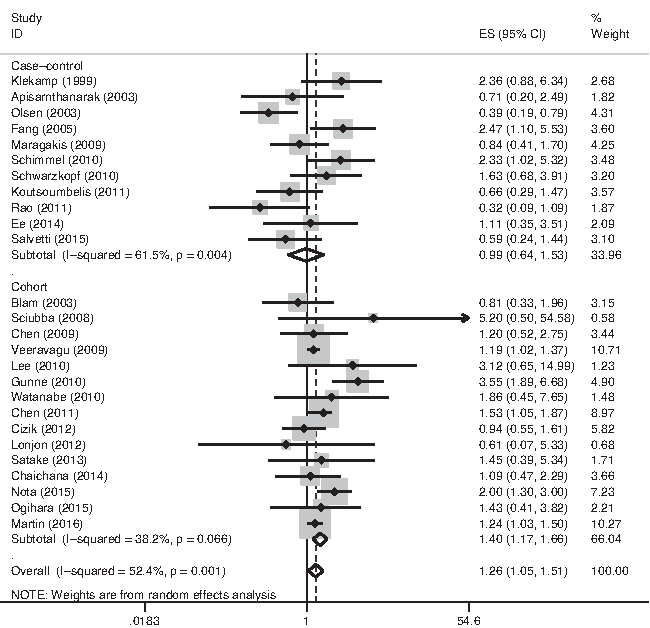
Forest plot of association between smoking and surgical site infection after subgroup analysis according to study design. Random-effect model was used to estimate summarized odds ratios.
CIs = confidence intervals; ORs, odds ratios.
PAF calculations
The prevalence of smoking in patients who underwent spinal surgery was extracted from a cohort study with a large sample [18], and the summary estimates were obtained from all studies combined. Using the prevalence and summary estimates, the PAF of SSI attributable to smoking was 5.67% (range 1.14%–10.56%). When adjusted risk estimates were used, the proportion of SSI associated with smoking increased to 10.37% (range 1.82%–20.14%).
Discussion
The present meta-analysis of 26 observational studies revealed a higher risk of incision infection in smokers than in nonsmokers. This risk was obvious in cohort studies and studies with adjusted estimates. The calculated proportion of SSIs associated with smoking was 10.37%. These data suggest that smoking increases the risk of SSI after spinal surgery.
The main finding in the present study may be explained by the following pathophysiological mechanisms. (1) Tobacco can damage organ systems as well as surgical incisions. Several types of organ damage have been shown to impair immune function and increase the risk of infection [40]. (2) Attenuation of the inflammatory healing response and impairment of oxidative bacterial killing mechanisms lead directly to SSI. (3) The acute detrimental vasoactive effect of smoking leads to incisional necrosis, a delayed proliferative healing response, and alterations in collagen metabolism that lead to dehiscence, incisional hernia formation, and impaired bone healing; these complications increase the risk of infection indirectly [41–43].
The advantage of a meta-analysis is that different study designs and settings can be examined by reviewing the evidence of multiple studies. Some questions that cannot be answered by a single study may be settled in this way. In the subgroup analysis of the present meta-analysis, the combined association between smoking and SSI became neutral in the case-control subgroup. In a study conducted by Olsen et al. [31], smoking actually showed a protective effect on post-operative infection (OR 0.4). We consider that the results of case-control studies have a higher chance of being influenced by selection bias. In these studies, smoking was not regarded as the primary outcome. It is difficult to avoid selection bias even when a random selection method is used. Unlike case-control studies, cohort studies investigate a population from the same cohort. Therefore, the results are less likely to be affected by selection bias and are more reliable.
The association between smoking and SSI may be confounded by many factors. For example, smoking is correlated with a high risk of diabetes mellitus [44,45], and patients with diabetes mellitus are more likely to develop SSI [46,36]. Thus, researchers should ensure adjustment for possible confounding factors such as prior radiation, body mass index, length of incision, and duration of surgery. This could be another reason some case-control studies using univariable analyses showed a negative association between smoking and SSI. Our subgroup analysis with adjusted estimates confirmed the effect of smoking on SSI, demonstrating the robustness of the final results.
Gronkjaer et al. [9] reported that pre-operative cessation of smoking seems to reduce the risk of post-operative complications among smokers. However, whether smoking cessation can reduce the risk of incision infection is unknown. Besides, if smoking cessation is effective, the length of time for which smoking must be stopped before surgery also needs to be elucidated. Prompt abstinence from smoking before surgery is important if a benefit of short-term smoking cessation is demonstrated. Thus, studies on these topics are required in the future.
The strengths of the present study include the extensive literature search, strict inclusion criteria, and quantitative analysis of the proportion of SSIs associated with smoking. The absence of important publication bias and the stable sensitivity analyses support the robustness of the study findings. However, there are several limitations to the study. First, although subgroup analyses were performed, none of the analyzed factors was able to explain all of the heterogeneity. The considerable differences across studies in factors such as race, smoking period, and definition of SSI might have resulted in greater heterogeneity and thus affected the final results. Second, most studies provided only crude ORs, and adjustment for multiple variables was found in only some of the studies. The difference in the degrees of adjustment is another source of heterogeneity. Third, few studies clearly distinguished former smokers and current smokers; thus, performance of a subgroup analysis according to smoking status is impossible. Moreover, no studies described the results of smoking according to different amounts of cigarette consumption. Without this information, a dose–response analysis cannot be performed. Future studies that examine the association between pre-operative smoking and post-operative infection should include a sufficient number of participants, adjust for potential confounding variables, and use a clear definition of smoking status.
In summary, the results of this meta-analysis suggest that smoking increases the risk of SSI after spinal surgery. False-negative associations in other studies may have resulted from defects in the study designs. After calculation of the PAF, the proportion of SSI explained by smoking increased to 10.37%. However, because of the heterogeneity among the studies, the results of this meta-analysis should be interpreted with caution.
Footnotes
Author Disclosure Statement
No competing financial interests exist.