
Abstract
Abstract
Background:
We investigated the clinical effectiveness of antimicrobial prophylaxis in lower-extremity open fractures following the Eastern Association for the Surgery of Trauma Guidelines.
Methods:
This observational, retrospective, single-center study included adults with lower-extremity open fractures of the ankle, tibia, fibula, or femur. The primary endpoint was the incidence of osteomyelitis within 12 months of the fracture. Secondary endpoint comparisons were the time of antibiotic initiation and drug selection.
Results:
A total of 90 patients were included. Patients suffered from Gustilo and Anderson grades I (14%), II (54.7%), and III (31.3%) fractures. Almost all patients received cefazolin (98%). Among grade III fractures, 59.3% (16/27) of patients received additional gram-negative coverage as recommended by the guidelines. The osteomyelitis rate was 8.9%. There was no difference in osteomyelitis rates among patients with grade III fractures who received or did not receive additional gram-negative coverage: 18.8% (3/16) and 0 (0/11) (p = 0.248), respectively. There was no correlation between median antibiotic start time or antibiotic stop time after closure and the development of osteomyelitis, respectively. Resistant organisms caused 50% (4/8) of the osteomyelitis cases. On univariate analysis, obesity had the most significant association with osteomyelitis (p = 0.026).
Conclusions:
Bacterial resistance was common among cases of osteomyelitis in our cohort. Obesity was associated with a higher rate of osteomyelitis.
P
Although these guidelines have been adopted in practice, supporting evidence for some recommendations is limited, especially for the use of aminoglycosides in Gustilo and Anderson grade III fractures [6,7]. The recommendation for the use of aminoglycosides is based primarily on a study comparing cloxacillin with clindamycin in which neither group received an aminoglycoside. The results showed that for grade III open fractures, neither agent was effective because of the high rate (43%) of gram-negative organisms contributing to the infection [8]. The most common breakthrough gram-negative organisms were Enterobacter, E. coli, and Klebsiella spp. [8]. Importantly, the foundation of the guideline recommendations is based on studies more than 10 years old and thus may not account for the antimicrobial resistance patterns seen in daily practice today [5,6,8]. We therefore sought to assess the effectiveness of guideline-based antimicrobial prophylaxis in preventing osteomyelitis in patients with lower-extremity open fractures.
Patients and Methods
Setting
Palmetto Health Richland is a teaching hospital affiliated with the University of South Carolina School of Medicine. The study center is a Level I trauma center that provides care for a 16-county region in the southeastern United States. The institution has nearly 100,000 emergency department visits annually and provides care for more than 2,000 trauma patients. The local Institutional Review Board determined this study to be exempt from review prior to data collection, and the research was conducted in accordance with the principles outlined in the Declaration of Helsinki.
Patient and Data Selection
All patients 18 years or older admitted for open lower-extremity fractures of any grade over a 35-mos period were assessed for study eligibility through hospital billing and discharge International Classification of Diseases (ICD)-9 codes (820.13, 821.3, 821.31, 821.39, 823.11, 823.12, 823.3, 823.31, 823.32, 823.92, 824.1, 824.3, 824.5, 824.7, 824.9, 825.1, 825.3, 825.31). Patients who received antibiotic therapy for purposes other than open fracture prophylaxis or who had concomitant upper-extremity open fractures were excluded to eliminate the confounding effects these conditions would have on infection rates. Data on patient characteristics and outcomes were collected using retrospective medical record review. Pertinent patient data including an assessment of renal function and patient characteristics, including age, weight, serum creatinine concentration, and race. Data on injuries included fracture grade according to the Gustilo classification system [2], site, and injury mechanism. Specific information on antimicrobial drug use was collected, including use of gram-negative coverage, time to start of drug administration, and duration of use.
Statistical Analysis
The primary endpoint was the occurrence of osteomyelitis within 12 months after the open fracture event. Osteomyelitis was identified by a positive bone culture obtained in the operating room that required antibiotic treatment, as documented in the health systems network medical records. Deep tissue or surgical site infections were not collected because of concern about the inaccuracies in documentation of these events in a retrospective study. Secondary endpoints were the rates of infection among different Gustilo and Anderson grade fractures and time to initiation of prophylactic therapy, which was defined as the time from emergency department presentation until all prescribed antibiotics were being administered. Additionally, factors such as antimicrobial drugs received, mechanism of injury, age, weight, and ethnicity were evaluated for their impact on the rate of osteomyelitis. The adverse events of Clostridium difficile infection and acute kidney injury secondary to nephrotoxicity were assessed for all patients during their hospital stays. Acute kidney injury was defined as a serum creatinine concentration greater than or equal to 1.5 times baseline during hospitalization, in accordance with the Acute Kidney Injury Network criteria.
Analyses were performed using GraphPad Prism and R Core Team (2014) software. The Fisher exact and χ2 tests were used for categorical data, and Mann-Whitney tests were applied to continuous variables. The secondary objectives were addressed by cross-tabulating the risk factor with the outcome (development of osteomyelitis). Because of the small number of osteomyelitis cases, which would be reduced further by missing values in the predictors, multivariable predictor logistic regression was not performed.
Results
During the study period, 226 patients were identified by ICD-9 codes, and 40% of these patients (n = 90) met the study inclusion criteria. Patients were excluded primarily for concomitant non-lower-extremity open fractures and antibiotic administration during hospitalization for infections not related to the lower-extremity fracture. A majority of patients (68.7%) had grades I and II fractures (Table 1). Nearly all patients (97.8%) had fractures of the ankle, tibia, or fibula.
BMI = Body mass index; MC = motorcycle crash; MVC = motor vehicle crash; PedVC = pedestrian versus car.
The primary outcome of osteomyelitis after antibiotic prophylaxis occurred in 8.9% of the patients (n = 8). Osteomyelitis developed among patients with grades I, II, III, and undetermined grade fractures at a rate of 0% (0/12), 10.6% (5/47), 11.1% (3/27), and 0 (0/4), respectively. The median time until osteomyelitis diagnosis was 72 d (range 7–239 days).
The low incidence of osteomyelitis prevented a full logistic regression analysis, but Table 1 demonstrates the difference in the characteristics of patients with and without osteomyelitis. Body mass index and age were significantly higher among those who developed osteomyelitis compared to those who did not (Fig. 1).
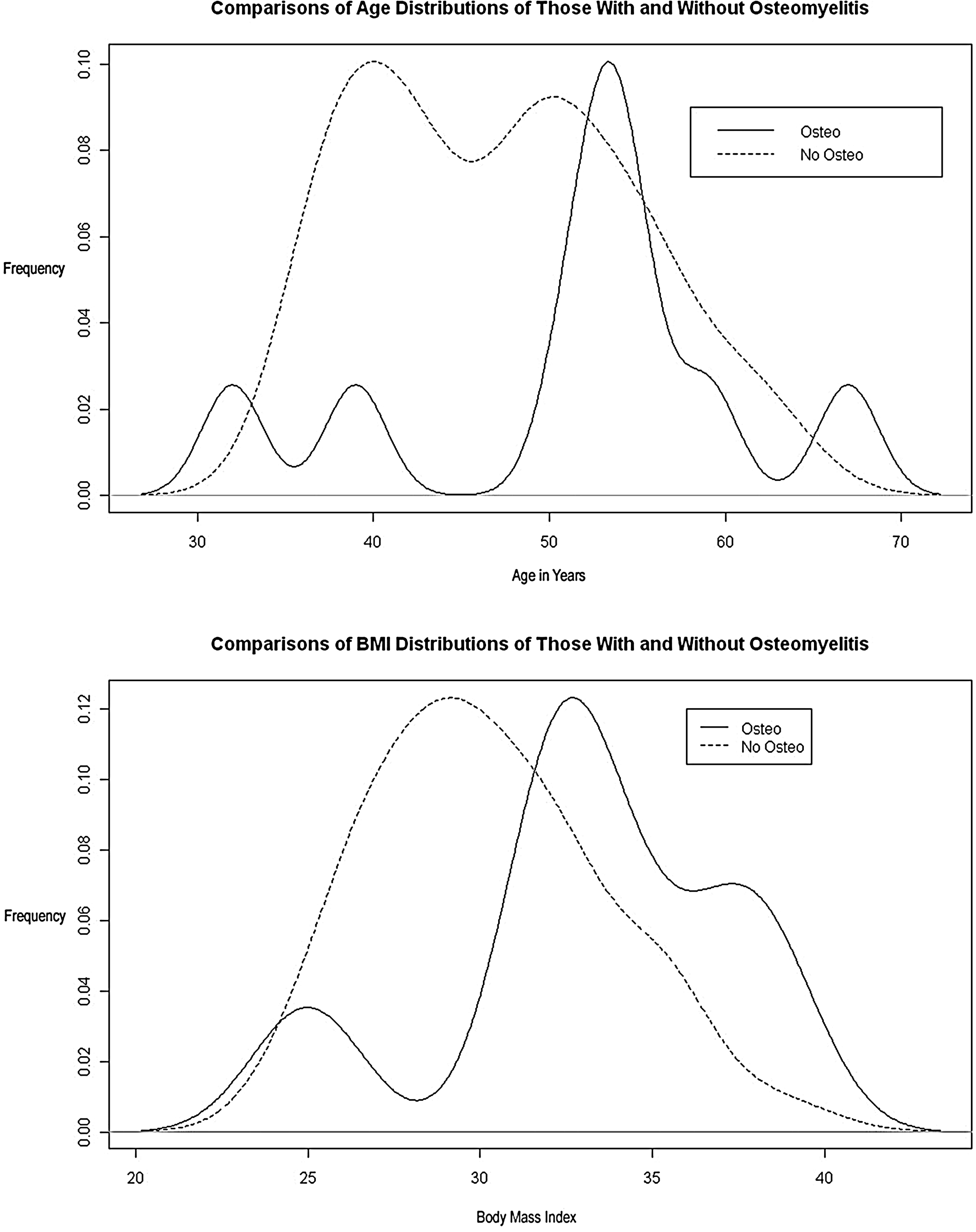
Univariable analysis of age and body mass index (BMI) demonstrated that osteomyelitis was associated with increased age and BMI (median age 53.5 vs. 41.5 years; p = 0.026; median BMI 33.4 vs. 27.8 kg/m2; p = 0.021).
The time to the start of antimicrobial prophylaxis was not correlated with the development of osteomyelitis by Wilcoxon rank sum testing (median 5.75 h vs. 3.99 h; p = 0.30). The median antibiotic stop time after wound closure was 22.9 h (interquartile range [IQR] 19.6–37.6 h). Antibiotic stop time was not different in those who developed and did not develop osteomyelitis (median 23.0 h vs. 22.9 h; p = 0.7145). Twelve patients received antibiotics for longer than 48 h after site closure without any apparent harm compared with patients receiving antibiotics for ≤48 h after closure. One patient developed acute kidney injury, but no patient manifested C. difficile infection.
Ninety-eight percent of the patients (n = 88) received cefazolin for prophylaxis. Twelve patients had a documented penicillin allergy, but only two of these were given clindamycin instead of cefazolin. Cefazolin was dosed at 2 g q 8 h for 48.9% of patients and 1 g q 8 h for the remaining patients. Cefazolin was appropriately dosed in 74% of patients according to recent guideline recommendations [9]. Additional gram-negative coverage was added in 0 (0/12), 21.3% (10/47), and 59.3% (16/27) of patients with grade I, II, and III fractures, respectively. Aminoglycosides, namely gentamicin (n = 23) and tobramycin (n = 1), were the primary agents selected. The other agents were aztreonam (n = 3), ceftriaxone (n = 1), and piperacillin/tazobactam (n = 1). There was no statistical difference in osteomyelitis rates among patients with grade III fractures who received and did not receive gram-negative coverage (18.8% [3/16] vs. 0 [0/11]; p = 0.25). Of note, gram-negative organisms were the cause of all grade III fracture osteomyelitis cases (3/3) and half (4/8) of the cases among all fracture grades. The remaining 50% of the osteomyelitis cases were caused by Staphylococcus aureus, 75% of which were methicillin resistant (MRSA) (Table 2).
MC = Motorcycle crash; MRSA = methicillin-resistant Staphylococcus aureus; MSSA = methicillin-sensitive S. aureus; MVC = motor vehicle crash; R = resistant; S = sensitive.
Discussion
The overall incidence of osteomyelitis was 8.9%, which is similar to the figures observed in prior studies [10–12]. Similar to previous studies, which have shown a low incidence of osteomyelitis in grade I open fractures, no patients in our series with a grade I fracture developed osteomyelitis. Patients with grades II and III fractures developed osteomyelitis at similar rates, 10.6% and 11.1%, respectively, whereas previous cohorts have shown an increase in osteomyelitis rates between grade II and III open fractures, 7.4% and 19.2% or 4.7% and 12.2% [5,6]. The difference in the present study may be explained by the higher rate of MRSA infection among patients with grade II open fracture and the slightly lower incidence of osteomyelitis in grade III open fractures compared with published series. This study examined osteomyelitis rates longer than previous studies (12 mos vs. 6 mos), but this additional time captured more data related to osteomyelitis and, possibly, non-union [2,6,10]. We are unable to determine if these differences are attributable to changes in microbial flora or to random effects.
All three cases of osteomyelitis in grade III open fractures were caused by gram-negative organisms. Indeed, the current practice guidelines suggest administering cefazolin plus an aminoglycoside for grade III open fractures, as the risk of gram-negative infections is higher than in other grades of open fracture [1,12]. These patients received additional gram-negative coverage but still developed osteomyelitis caused by gram-negative organisms. There could be several explanations for this occurrence. First, the incidence of infections caused by multi-drug-resistant organisms is increasing [13]. However, the pathogenic organisms infecting our patients with grade III open fractures were susceptible to the prophylactic antibiotics administered. Therefore, it is unlikely that antimicrobial resistance played a role. Of note, three patients with osteomyelitis (one Grade II fracture, two Grade III fractures) had Enterobacter cloacae as the causative organism. This organism frequently is multi-drug-resistant because of the production of beta-lactamases. In all three of our cases, the Enterobacter was resistant to cefazolin, but where data were available, it remained sensitive to gentamicin. Second, bone penetration of the aminoglycosides has been reported infrequently; and for gentamicin specifically, there is a large variability in bone to serum concentrations [14]. Fluoroquinolones concentrate in bones and could be an alternative to aminoglycoside therapy, especially for patients who have or are at high risk for acute kidney injury. The use of ciprofloxacin monotherapy was evaluated in a prospective study, which found an unacceptable rate of infection in patients with grade III fractures (31%) [6]. However, the addition of a fluoroquinolone in place of an aminoglycoside to cefazolin has not been evaluated. The routine use of fluoroquinolones is discouraged because of the development of resistance to these widely used drugs [15]. Additionally, some clinicians hesitate to use ciprofloxacin, as its use delays fracture healing, which is a risk factor for infection [16]. For future studies, targeted gram-negative therapy utilizing local antibiograms should be evaluated.
Other than antimicrobial characteristics, host factors may play an important role in the development of osteomyelitis. By univariable analyses, the most predictive factor for osteomyelitis was increasing BMI. Indeed, all patients with grade III open fractures who developed osteomyelitis were obese. Interestingly, a study found that vasculogenic progenitor cells in obese compared with non-obese patients showed less adhesion and decreased migration to damaged tissue and slower proliferation, which ultimately reduced the revascularization of the injured tissues in the obese patients [17]. These factors led to prolonged healing time, which is a known risk factor for infection [18]. Furthermore, obese patients may require higher doses of antimicrobial drugs than non-obese patients. In a pharmacokinetic study, it was suggested that obese patients may require greater than 2 g of cefazolin to obtain adequate tissue concentrations [19]. The present study did not find a difference in rates of infection between those who had weight-based dosing of cefazolin compared with those who did not, but this could be an effect of the sample size. Taken together, these factors likely place obese patients at higher risk for the development of osteomyelitis after open fracture. Additionally, univariable analysis showed a higher incidence of osteomyelitis with increasing age. Previous small studies have not shown an association between osteomyelitis and age; however, a recent study of the epidemiology of osteomyelitis found an association between increasing age and the risk of the infection. This association seems plausible, given the possibility of age-related reduced vascularity and impaired healing [20,21].
In the present study, time until antibiotic administration was shorter among patients who did not develop osteomyelitis, but the difference was statistically non-significant. However, because of the small number of osteomyelitis cases, it is difficult to rule out the importance of this variable. A previous study found a significant decrease in osteomyelitis when antibiotic administration began within three h compared with a later start, 4.7% and 7.4%, respectively [7]. Clinicians should prioritize timely administration of antimicrobial prophylaxis in patients with open fractures.
As a retrospective study, our data were limited to those found in the electronic medical record. The rate of osteomyelitis also depended on patients reporting to the study center for follow-up, and a longer 12-mos follow-up could have included patients with osteomyelitis and prosthesis infection also. Further, antibiotics received between hospital discharge and the onset of osteomyelitis could not be accounted for. Additionally, the number of drug-resistant pathogens may differ at other centers. Limited sample size because of the large number of exclusions has hindered the detection of independent predictors of osteomyelitis by multivariable analysis. There are additional data that are lacking, limiting this study. This includes classifications of injury severity and data on non-fusion and skin and soft-tissue infection rates. Data also are unavailable on other causative factors, including the presence of foreign bodies/prostheses and contributing co-morbidities, including diabetes and peripheral vascular disease.
Overall, this study demonstrates that osteomyelitis remains a prevalent complication in patients with open lower-extremity fractures despite recommended antimicrobial prophylaxis. Drug resistance was present in some cases of osteomyelitis, and clinicians may consider coverage for resistant organisms when choosing antimicrobial agents for prophylaxis. Additionally, we observed obesity to be a risk factor for the development of osteomyelitis. This finding warrants further investigation, and clinicians should consider the pharmacokinetics of antimicrobial agents and provide optimal dosing for obese patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist for any of the authors.