
Abstract
Abstract
Background:
Anastomotic leak is the most dreaded septic complication of colorectal surgical procedures. Death is proportional to the time between occurrence and diagnosis of the leakage. Biomarkers, which may help to predict anastomotic leakage before appearance of its clinical features, may be beneficial in preventing adverse outcomes. This study investigates a biomarker that might be useful to predict rectal anastomotic leakage before its clinical presentation.
Patients and Methods:
Serum procalcitonin and C-reactive protein (CRP) levels, bacterial proliferation, interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α) levels of drain fluid were evaluated in 50 consecutive patients who underwent low anterior resection without diverting ostomy for rectal carcinoma.
Results:
Anastomotic leakage occurred in seven of 50 (14%) patients. Serum CRP and procalcitonin levels at post-operative day three were higher in patients with anastomotic leakage (p = 0.01, p = 0.02 respectively). Drain TNF-α values were increased 63.2% on post-operative day five when compared with post-operative day three in patients with anastomotic leakage, but were decreased in patients without leakage. There was no statistical difference for drain IL-6 levels between groups. The bacterial proliferation rate of drain fluid culture in the leakage group was 42.9% at post-operative day three and 85.7% at post-operative day five (p = 0.29 and p = 0.0001, respectively).
Conclusions:
High serum CRP and procalcitonin values on post-operative day three are alarming, and assessment of anastomotic leakage by abdominal imaging with rectal contrast is suggested. In addition, increasing levels of TNF-α and bacterial proliferation in drain fluid are predictive, whereas IL-6 is not.
S
Further, shortening of hospital stay in parallel with wide use of laparoscopic procedures makes the earlier diagnosis/prediction of anastomotic leakage more crucial. Particularly in this patient population, an early indicator of anastomotic leakage may lead to detection of risky patients in a timely manner and their closer follow-up, and hence shortening of hospital stay and duration of the treatment [2].
Patients and Methods
After ethical committee approval of the study design, 50 consecutive patients who underwent low anterior resection without diverting stoma and primary anastomosis for rectal cancer between March 2012 and April 2013 at Istanbul University, Cerrahpasa Medical Faculty were included in the present study. Patients presenting with obstruction and those receiving immunosuppressive treatment were excluded. A pelvic drain was placed in all patients. A bowel cleansing was applied systematically, using oral Fleet® Phospho-Soda 90 mL (C.B. Fleet Company, Inc., Lynchburg, VA) on the day before the operation and Fleet Enema 133 mL rectally on the morning of operation. Ampisid 1 g (MN Pharmaceuticals, Istanbul, Turkey, ampicillin sodium 1 g, and sulbactam sodium 500 mg) was administrated intravenously as prophylaxis 30 minutes before incision and repeated every three hours if the operation was longer according to the regulations of the hospital infection control committee.
After completion of anastomosis (either hand-sewn or stapled), a leak test was performed: The colon was occluded at 2–3 cm proximal to the anastomosis by holding between the index and middle fingers and the pelvic cavity was filled with sterile %0.9 saline until the anastomosed area was fully covered. After that, air was administered through the anus via a 50 mL syringe. If no air bubble came out from the saline-filled pelvis, it was assumed that the anastomosis was complete and secure.
The age, gender, body mass index, pre-operative serum albumin and hematocrit levels, existence of neo-adjuvant therapy, eventual metastases, intra-operative blood loss, and operative time were recorded. Patients were divided into two groups according to the occurrence of clinical anastomotic leakage (LG: leakage group) or not (NLG: non-leakage group).
Radiologic evaluation (computed tomography with rectal contrast enema) was performed only when leakage was clinically evident or suspected—not routinely. A suspicion for an anastomotic leakage occurred when the patient had fever after the post-operative third day, existence of fecal or suspicious fluid coming from the drain was observed, or the patient had abdominal tenderness.
Biochemical studies
Blood samples were collected on the day before the operation and on post-operative days one and three for serum C-reactive protein (CRP) and procalcitonin (PCT) measurements. Samples from drain fluid were collected by a sterile method at post-operative days one, three, and five. The fluid samples were centrifuged for 20 minutes at 1,500 rpm and kept at −80°C for subsequent tumor necrosis factor- α (TNF-α) (Eastbiopharm Co. Ltd, Hangzhou) and interleukin-6 (IL-6) (Eastbiopharm Co. Ltd, Hangzhou) analyses by the enzyme-linked immunosorbent assay method.
Microbiologic analysis
Gram staining preparations were made for direct microscopic examination, and standard aerobic and anaerobic cultures were performed from the samples obtained from drain fluid on post-operative days one, three, and five by the microbiology department. Sheep-blood agar, chocolate agar, and McConkey agar plates were inoculated for aerobic cultures. Plates were incubated at 37°C in 5%–7% CO2 for 2–4 days. The bacterial proliferation was identified by standard clinical microbiologic methods [3].
Anaerobic blood agar, phenyl ethyl alcohol blood agar, kanamycin-vancomycin-laked blood agar, Bacteroides bile-esculine agar plates (BD Diagnostic Systems, Sparks, MD), and thioglycolate broth were inoculated for anaerobic culture. Anaerobic incubation was made in anaerobic jars (Thermo Scientific,™ Oxoid, MA) at 37°C for seven days before initial examination. Anaerobic conditions were obtained with AnaeroGen (Thermo Scientific). The anaerobic bacteria grown were identified by standard clinical microbiologic methods and using API 32 ID (BioMerieux® SA, Marcy-L'Etoile, France) [4].
The positive culture rates and the bacteria identified among the patients with and without anastomotic leakage were compared and analyzed.
Statistical analysis
For the statistical analysis of the study, the parameters taken into consideration were mean, standard deviation, frequency, and percentage. The comparison of frequency and percentage between the groups was performed using chi-square and Fisher exact tests. For the comparison of the variables with normal distribution in two different groups, the Student t test, and for the groups with different variants, Mann-Whitney U test, were used.
In dependent sampling, for the experimental settings with three or more cross-sections, the significance of the differences were tested by analysis of variance (ANOVA) (General Linear Model, repeated measures ANOVA). When the significant difference was detected, for the comparison of the differences among the cross-sections, post hoc LSD (least significant difference) test was used.
Depending on the subject number and the homogeneity testing, non-parametric Wilcoxon test and Friedman two-way ANOVA methods were used in suitable experimental settings. Statistical significance was defined as p < 0.05. For statistical analysis, Statistical Package for the Social Sciences (SPSS 17.5 Inc, Chicago, IL) software was used. This study is registered in ClinicalTrials.gov under ID NCT02361918.
Results
Among the 50 patients included in the study, 35 were male. In seven (14%) of patients, anastomotic leakage was observed in post-operative follow-up while none was detected during operation. All patients with observed anastomotic leakage were male (p > 0.05). The average age of patients was 61 ± 4.9 years in the LG and 63.1 ± 11.7 years in the NLG (p > 0.05). In five of seven patients, the leakage was major, and they were promptly re-operated to perform a peritoneal cleaning and a diverting stoma. In two patients, the leakage was minor, and they were treated conservatively. The leakage was diagnosed mostly on days six and eight (median 6, range 5–9).
From the aspect of body mass index, pre-operative serum albumin and hemoglobin level, history of neo-adjuvant therapy, metastases, performed surgical technique, intra-operative blood loss, and post-operative intensive care requirement, both groups were similar (p > 0.05 for each factor), whereas the operative time was significantly longer in the LG (p < 0.05). Those parameters are given in Table 1.
One patient in the LG (2.3%) and one patient in the NLG died, the former at post-operative day 40 because of severe sepsis and the latter, who had liver metastases, at post-operative day 35 because of hepatic failure.
Drain TNF-α levels were increased at a rate of 63.2% at post-operative day five when compared with post-operative day three in patients with anastomotic leakage, but were decreased in patients without leakage. The high standard deviation value precluded the statistical significance of this increase (p = 0.067) (Fig. 1). Drain fluid IL-6 levels were comparable between groups but no statistical differences were found (Fig. 2). Drain fluid TNF-α and IL-6 levels are given in Table 2.
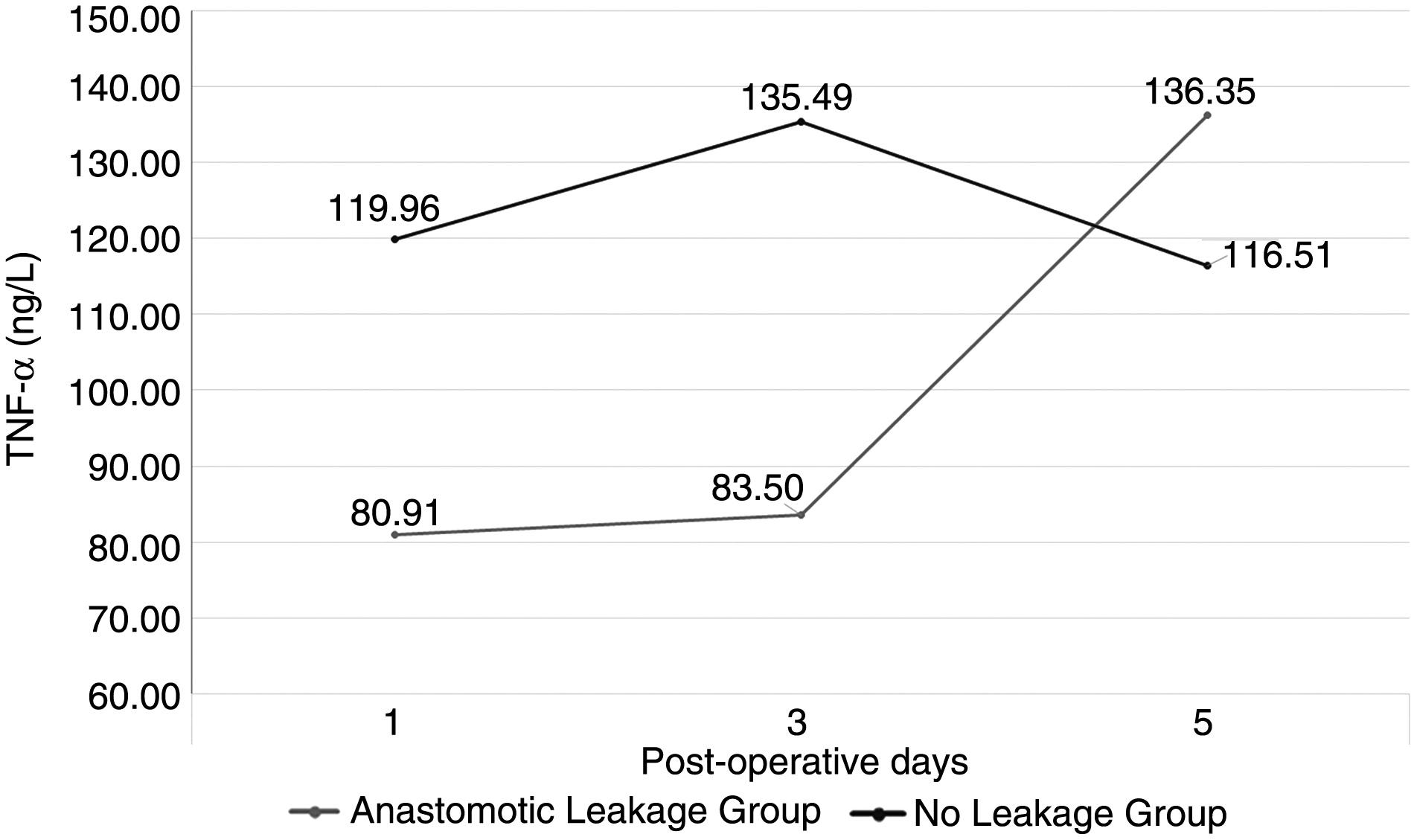
Mean tumor necrosis factor-α (TNF-α) values in drain fluid.
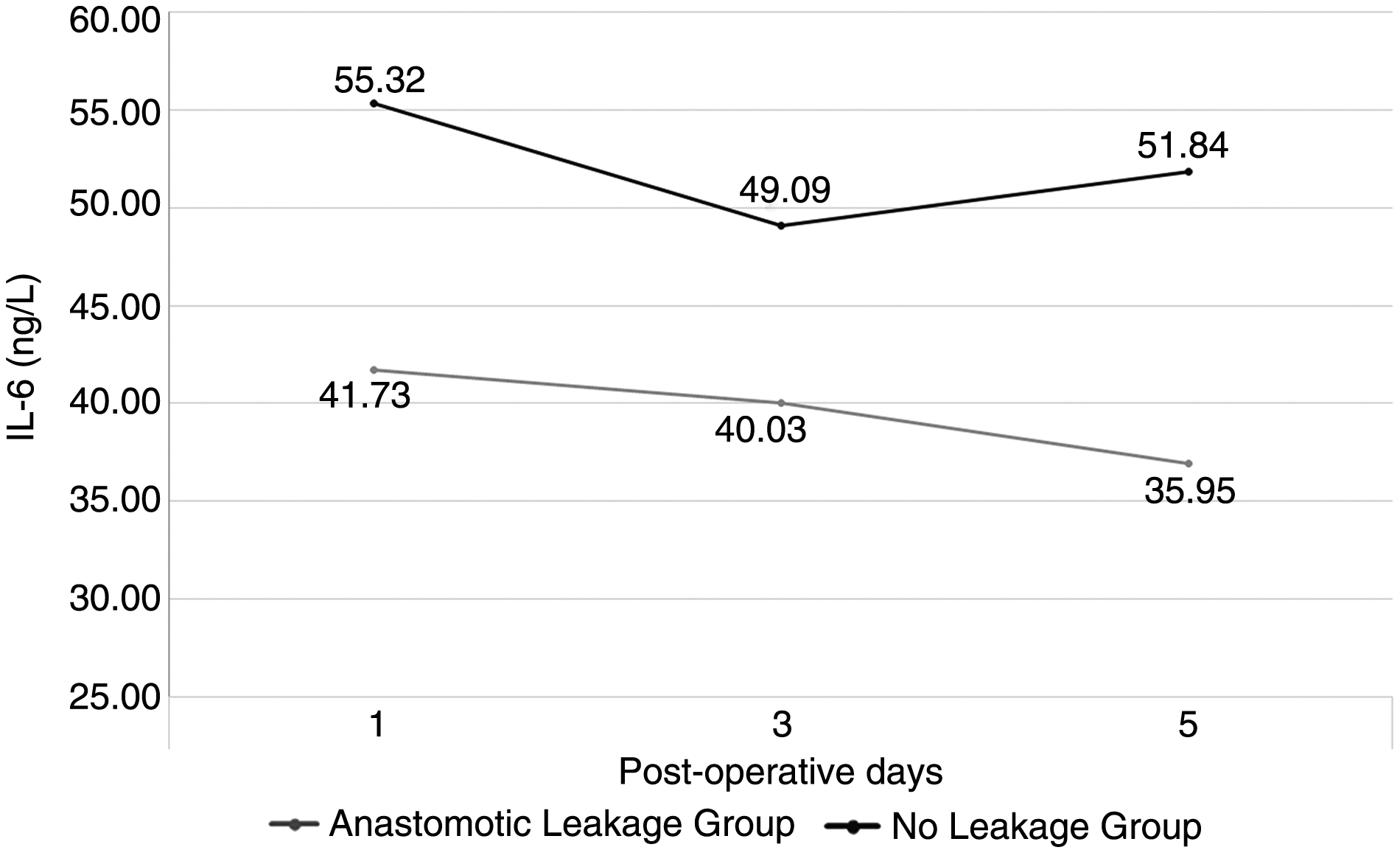
Mean interleukin-6 (IL-6) values in drain fluid.
TNF-α = tumor necrosis factor-α; IL-6 = interleukin-6.
Because of great fluctuations within group variants, the Mann-Whitney U test was used.
Pre-operative and post-operative day one serum CRP values were quite identical in the two groups. On post-operative day three, CRP increased at a rate of 45.1% compared with post-operative day one in the LG group, whereas it was decreased in the NLG (p = 0.01) (Fig. 3).

Mean serum C-reactive protein levels.
Similarly, while pre-operative and post-operative day 1 serum PCT levels were quite equal among groups, on post-operative day three, the value increased at a rate of 26% in the LG. This increase was only 5.8% in the NLG (p = 0.02) (Fig. 4). Serum CRP and PCT levels are given in Table 3.
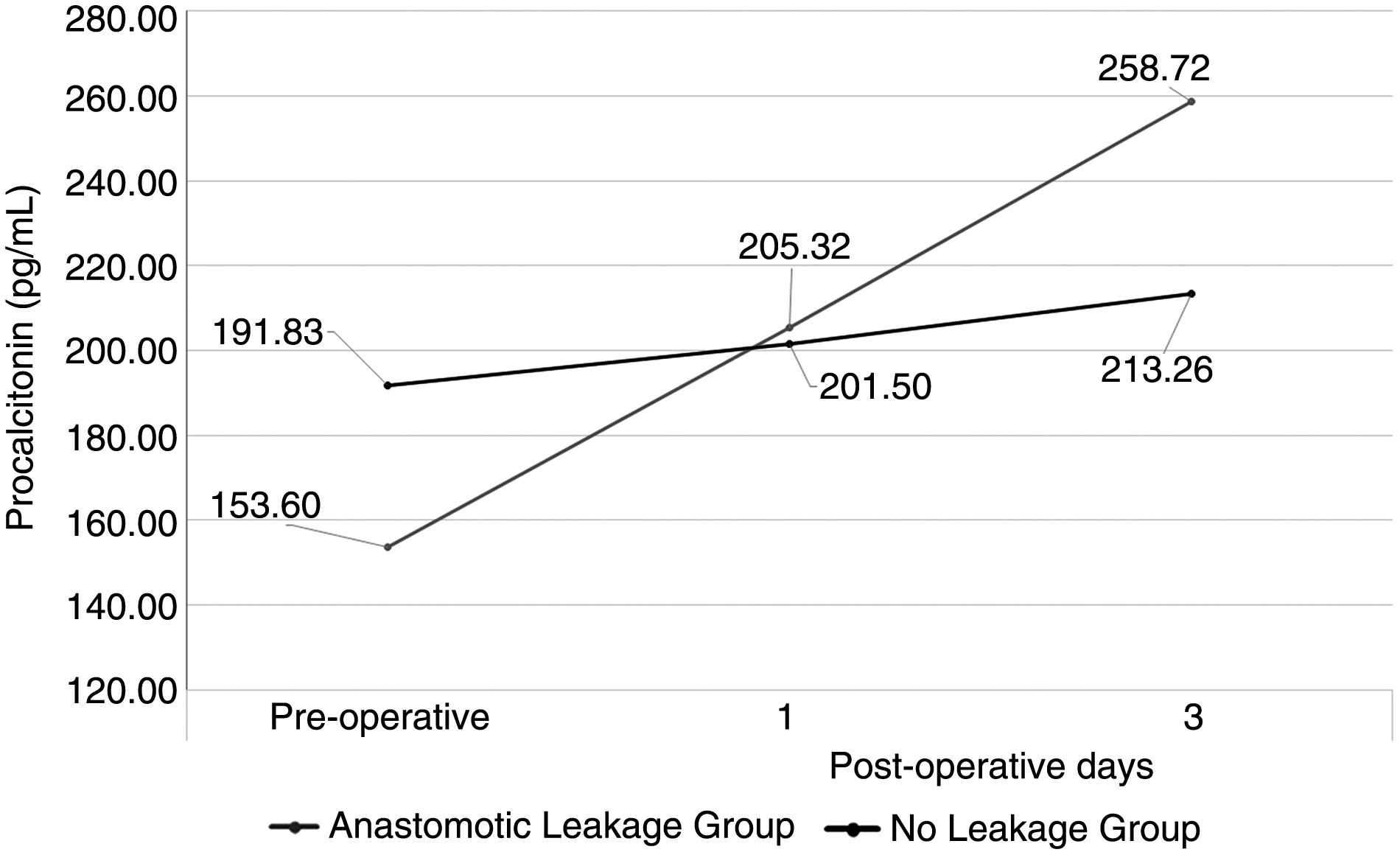
Mean serum procalcitonin levels.
Because of great fluctuations within group variants, the Mann-Whitney U test was used.
Culture results of drain fluid in the LG were positive at a rate of 28.6% at the first, 42.9% at the third and 85.7% at the fifth post-operative days. In the NLG, these values were 9.3%, 7%, and 11.6%, respectively (Fig. 5). The difference of the third and fifth post-operative days' levels between groups was statistically significant (p = 0.29 and p < 0.001, respectively).

Bacterial growth percentages.
In the LG, drain fluid culture showed Klebsiella spp. in two patients (28.5%) at post-operative day three. On post-operative day five, culture results were Escherichia coli in five (71.4%) patients and Klebsiella spp. in four (57.1%) patients. The culture results are shown in Table 4.
In addition to findings related to possible early predictors of anastomotic leakage, all leakages were observed in patients whose anastomosis was performed with the stapler technique (17.1% in stapler used patients vs. 0% in hand-sewn patients, p = 0.325). This difference, however, did not reach statistical difference because of unequal distribution of patients (41 patients with stapler and nine patients with hand-sewn anastomosis).
Discussion
Anastomotic leaks lead to increased morbidity, death, prolonged hospital stay, and high local recurrence rates after surgical resections of rectal cancer [5,6]. The anastomotic leakage rate after anterior resection is 8%–24% [7]. In this study, this rate was 14%.
The diagnosis of anastomotic leakage is still based on clinical signs, appearance of fecal material through drains or incision, and laboratory findings such as leukocytosis and elevated serum CRP levels. This conventional attitude may cause important delays in diagnosis [8]. Alves et al. [9] showed that death increased significantly in patients in whom anastomotic leakage was diagnosed after post-operative day five. On average, the leakage is detected at post-operative day seven [10]. In this study, the time point for detection of leakage was 6.4 days (range 5–9 d).
According to the International Study Group of Rectal Cancer, anastomotic leakage is classified as Grade A, B, and C. Grade A is defined as asymptomatic, radiologic leakage. Grade B is a leakage that necessitates percutaneous or transanal drainage, and Grade C is major leakage mandating surgical re-intervention [11]. In this study, the leakage may be graded as B in two and as C in five patients. Grade B patients were treated conservatively. Because they already had a drain, they did not require any additional intervention whereas Grade C patients were re-operated and abdominal cleansing and a diverting stoma were performed.
Although the use of drains in rectal operations is disputed, drains prevent serous and bloody fluid collections. Thus, infection in the anastomotic area is prevented, and detection of anastomotic leakage by draining fluid contaminated with bowel content in case of anastomotic leakage is eased by using drains [12]. The beneficial effect of drains, however, has not been proved yet [12]. Further, drains do not always reflect anastomotic leakage [13]. In the present study, a drain was placed in all of the patients.
Parallel to the widespread use of laparoscopy, early discharge of patients from the hospital (at day 5 or even day three) makes the early detection of anastomotic leaks more valuable, even indispensable. Clinical surveillance is insufficient, and yet no serologic/biochemical marker is available in the prediction of leakage [8]. An indicator that might reflect the peri-anastomotic medium may aid in the early diagnosis of leakage before appearance of septic and clinical signs.
Mesothelial cells, fibroblasts, and white blood cells are said to be the major source for peritoneal cytokines [14,15]. On the first post-operative day, the level of peritoneal cytokines reflects the magnitude of surgical stress, and its decline is expected in the following days; however, its increase may be an indicator of the earliest stage of leakage [16–19].
TNF-α is produced by macrophages and T-cells in response to tissue damage and/or infection. Its half-life is shorter than 20 minutes and represents one of the earliest cytokine responses. Herwig et al. [18], Uğraş et al. [16], and Matthiessen et al. [20] found that TNF-α levels in the peritoneal fluid were elevated at post-operative day one in anastomotic leakages. Fouda et al. [21] and Yamamoto et al. [22] concluded that post
In the present study, although the TNF-α values at post-operative day three were elevated, the difference was not statistically significant (p = 0.294). Further, the values at post-operative day five were augmented at a rate of 63.2% compared with post-operative day three levels (p = 0.067) in the LG, whereas they were decreased in the NLG. Although it was statistically insignificant in this study, when combined with information obtained from the literature, it can be said that in patients with anastomotic leakage, peritoneal TNF-α values increase in post-operative day five [16,18,21].
TNF-α and IL-1 stimulate secretion of IL-6. Its level rises after trauma and remains elevated for more than 10 days. Peritoneal IL-6 values had been reported elevated at the first and third post-operative days in patients with anastomotic leakage by Yamamato et al. [22]. Drain IL-6 levels were lower in the LG at post-operative days one, three, and five, similar to those in the study of Bertram et al. [23].
Early rise of serum CRP and PCT before clinical and radiologic presentation of leakage was shown in the literature, which might lead to early diagnosis and reduction of morbidity [24]. Increased serum CRP levels after operation decrease to normal levels at the third post-operative day. In this sense, serum CRP may be a valuable marker of infectious complications in colorectal surgery [25–28].
Welsch et al. [26] concluded that serum CRP was a sensitive, but nonspecific biologic marker of infectious complications. Pedersen et al. [29] reported that CRP levels more than 200 mg/L at post-operative day three suggest further evaluation but were not sufficient for diagnosis. In that study, patient groups were heterogeneous, and there was a wide range of CRP values. Almeda et al. [30] showed that a serum CRP level more than 140 mg/L at post-operative day three might be predictive for anastomotic leakage when other septic foci are ruled out.
Matthiessen et al. [25] concluded that serum CRP levels were a strong and early indicator of anastomotic leakage and recommended regular follow-up of CRP. Similarly, Korner et al. [31] demonstrated that CRP levels more than 190 mg/L at the third post-operative day was an indicator of anastomotic leakage in four of five patients. Ortega-Deballon et al. [27] concluded that CRP values less than 125 mg/L at the fourth post-operative day might allow secure discharge of patients. Parallel to those findings, in this study, high CRP levels were measured in the LG group, and this finding must generate further evaluation.
PCT reflects the presence of post-operative infection. Mokart et al. [32] demonstrated its superior sensitivity and specificity over CRP. Garcia-Granero et al. [24] reported that elevated PCT levels at post-operative day one increased further at the third and fifth post-operative days in the major LG. They concluded that PCT levels were more sensitive and specific. Reith et al. [33], however, concluded that PCT levels can also be increased in extra-intestinal infectious conditions such as pneumonia. In this study, CRP and PCT levels were not significantly different between major and minor leaks. At the third post-operative day, however, serum PCT values were significantly increased in the LG.
In the microbiologic analysis of drain fluids, the rate of bacterial proliferation in cultures of drain fluid samples was 28.3% at the first day, 42.9% at the third day, and 85.7% at the fifth day in the LG, whereas these values were 9.3%, 7%, and 11.6% in the NLG. The third and fifth day culture results were statistically different between groups. Conventional culture results were available in 2–5 days after inoculation. Although the culture results are reliable, they are time consuming. The quantitative bacterial evaluation by the polymerase chain reaction method may be more practical for earlier detection [12,34–36].
The present study differs from its analogues by the homogeneity of the series (all of the patients underwent low anterior resection for rectal cancer) and the plurality of criteria combining microbiologic and many biochemical parameters of serum and drain fluid. Comparison of anastomotic technique, however, was not an aim of this study; dominance of anastomotic leakage in stapler used patients and unequal distribution of patients to techniques were observed. Thus, results from this study cannot be used to compare the effect of anastomotic technique on occurrence of anastomotic leakage.
Conclusion
Early diagnosis of rectal anastomotic leakage is of paramount importance. Elevated levels of serum CRP and PCT at post-operative day three and increasing levels of TNF-α in drain fluid were found to be alerting. In this study, drain fluid IL-6 levels were inconclusive and culture of drain content was meaningful but impractical because of its delayed results.
Footnotes
Acknowledgments
This work was supported by Scientific Research Projects Coordination Unit of Istanbul University. Project number: 21889.
Author Disclosure Statement
No competing financial interests exist.