
Abstract
Abstract
Background:
Aortic graft infections (AGI) are rare, with an incidence of 0.6%–3% among patients with aortic grafts. Most previous reports are based on single-center material with limited follow-up. Because of the paucity of these cases, the optimal treatment remains unclear. A factor possibly affecting the mortality rate of these infections is whether the index procedure was emergency or elective. The aim of this study was to investigate the incidence of AGI and assess the long-term outcome after emergency and non-emergency aortic reconstruction in a large population.
Method:
A population-based, retrospective study was conducted of all patients treated with aortic reconstructive surgery at the two centers for vascular surgery in Stockholm County (population 2.2 million) during 2005–2015. Patients with AGI were identified by the in-hospital patient registry. Chart data on demographics, co-morbidity, index operation, type of infection, treatment, and outcome were analyzed.
Results:
Reconstructive aortic surgery was performed on 2,026 patients (open repair 47.7%; endovascular aortic repair 52.3%). The incidence of infection was 1.4% (29/2,026). The index operation was performed as an emergency in ten patients and non-emergency in 19. Median follow-up after the index operation was 69.2 months (interquartile range [IQR] 109.5). Patients having an emergency index procedure were older (77 vs. 69 y; p = 0.03). Time to infection was similar (30.2 ± 27.4 and 56.1 ± 51.2 mos; p = 0.21). The median time from diagnosis of AGI to surgery was 30 d (IQR 30.5 d). Infectious agents were identified in 76% of the cases. Of the conservatively treated patients, one was free of infection compared with three of the surgically treated. Conservatively treated patients had a higher graft-associated mortality rate of 57% compared with 25% of the surgically treated (p = 0.05).
Conclusions:
This population-based study with long-term follow-up confirms the low incidence of AGI, 1.4%. The similar incidence in the emergency and non-emergency groups suggests that the index operation is not decisive in the development of AGI. The outcome of these infections generally is poor but is worse for non-surgically treated patients.
A
The diagnosis of AGI is based on both symptoms and signs of infection and radiologic imaging, which helps in identifying the source of the infection. However, there are many ways of defining infection, and there are yet no commonly used criteria. Diagnosis entails blood tests, such as C-reactive protein, white blood cell count, and culture. Imaging is contingent on the available resources, but ideally employs computed tomography (CT), which can be combined with positron emission tomography, magnetic resonance imaging, or radionuclide-labeled leukocyte scanning. Computed tomography imaging often is considered the gold standard for diagnosis [3,4].
The difficulty in identifying relevant pathogens in patients with AGI is well known [2,4]. However, the most commonly reported infectious agents are Staphylococcus aureus, Enterobacteriaceae, and coagulase-negative staphylococci [2,5–7]. Fungal infections are rare and typically are seen in immunocompromised patients [8]. Infections occurring early after the index procedure (within the first three mos) generally are caused by more virulent organisms, whereas infections manifesting at a later stage commonly are caused by less virulent organisms such as S. epidermidis [9].
Treatment options consist of a combination of pharmaceutical and surgical measures, such as graft excision together with some form of reconstruction, either anatomic or extra-anatomic [9,10]. Guidelines for pharmaceutical management differ greatly [2,9,11,12], and there are no randomized studies defining a recommended length of antibiotic treatment.
Previous research consists mainly of single-center studies investigating graft infection after either endovascular aortic repair (EVAR) or open repair (OR). There are few studies covering both surgical methods, including emergency and non-emergency cases with data on long-term clinical outcomes [13–18]. The complication and mortality rates are higher in patients treated for an emergency condition than for elective procedures, and it is not unlikely that this difference could influence the risk of AGI [19]. The aim of this study was to determine the incidence of AGI in patients treated with an aortic procedure in a population-based cohort and to assess the long-term outcome after pharmaceutical or surgical treatment. Various risk factors for AGI, such as an emergency vs. a non-emergency index procedure, also were assessed.
Patients and Methods
This study was approved by the local Ethics Committee. Informed consent from the patients was not considered necessary.
Design
A population-based, retrospective, register-based analysis was carried out of all patients with infected aortic grafts after treatment for abdominal or thoracic aortic aneurysms or aortoiliac occlusive disease (AIOD) at the two centers for vascular surgery in the Stockholm County region (population 2.2 million) during 2005–2015.
Population
Using the in-hospital electronic patient registry (Take Care®) and the Swedish National Registry for Vascular Surgery (Swedvasc), 2,026 patients who had been treated for aortic aneurysms or AIOD were identified. The validity of Swedvasc is reportedly high [20]. The Tenth International Classification of Diseases (ICD-10) codes for aortic aneurysms and AIOD, in combination with the codes indicating post-operative vascular complications, were used to identify all patients with post-operative AGIs after either OR or EVAR in both emergency and non-emergency cases (Fig. 1). The ICD codes used were I70.0, I71.1–I71.6 as well as T81.7, T82.7, and T81.4. This review yielded 219 patients. Emergency cases were defined as operations for ruptured or symptomatic aneurysms, and non-emergency cases were defined as procedures for non-symptomatic and non-ruptured aneurysms as well as cases of AIOD. Patients with a complication other than graft infection or with an infection of an origin other than the aortic graft were excluded. After a thorough review of medical records, 29 patients with aortic graft infections were identified, 1% of the total number of surgical patients (Fig. 1).
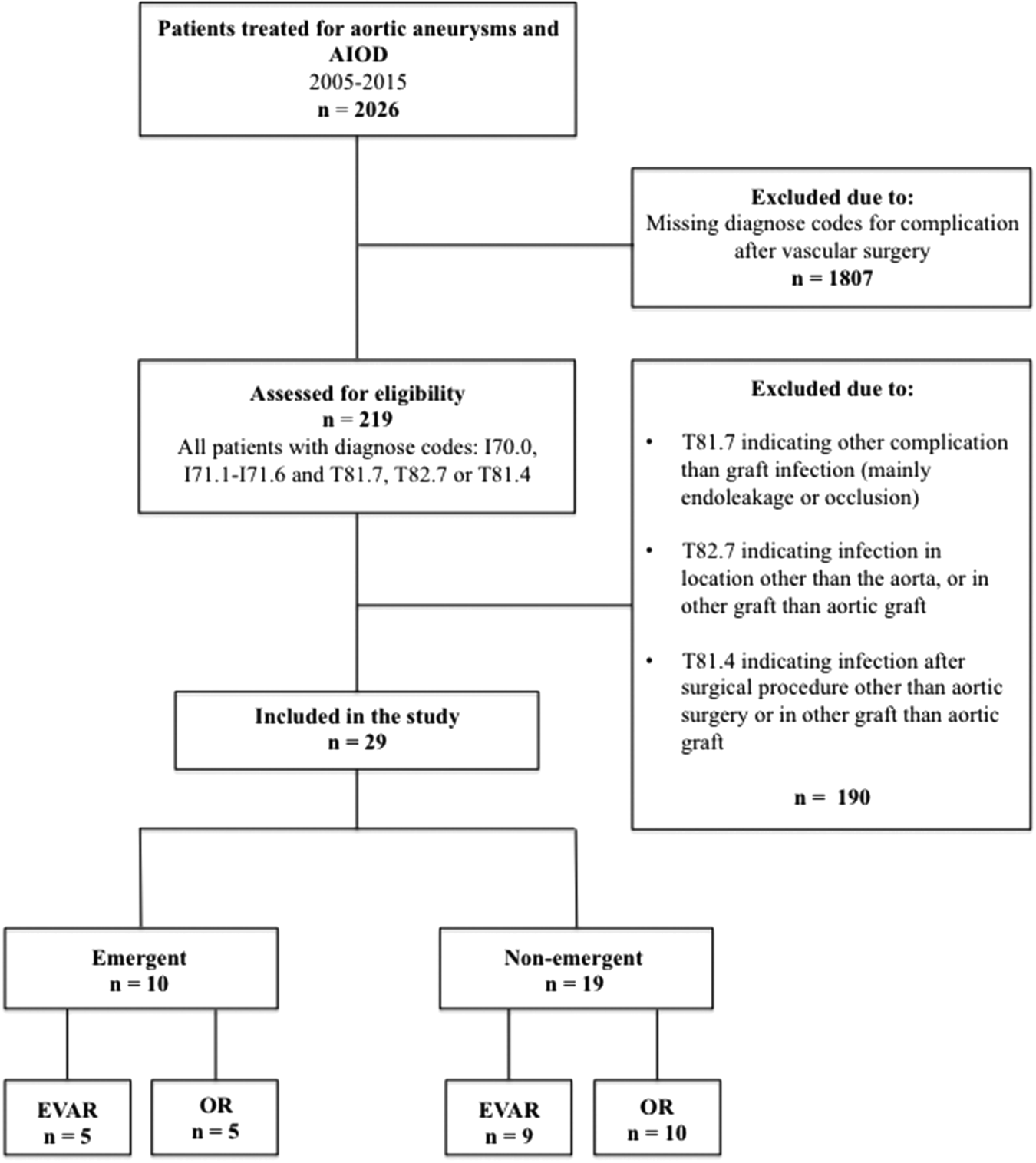
Patient population. AIOD = aortoiliac occlusive disease; EVAR = endovascular aortic repair; OR = open repair.
Clinical data and definitions
The medical records provided information on medical history, type of infection, treatment (non-surgical vs. surgical), and outcome. Conservative treatment was defined as antibiotic or anti-fungal medication without major surgical revision. Surgical intervention was defined as either operative reconstruction with graft excision and replacement or debridement of infected aortic tissue without graft excision.
Patient characteristics from the primary aortic intervention, defined as the “index operation,” was collected: gender, age, and body mass index (BMI; kg/m2) and co-morbidities including hypertension, renal impairment (serum creatinine concentration >100 μmol/L), cardiac disease, chronic obstructive pulmonary disease (COPD), diabetes mellitus type 2, or cerebrovascular disease. Cardiac disease included congestive heart failure, atrial fibrillation, angina pectoris, and myocardial infarction. Smoking habits were defined as current smoker (smoking at time, or cessation within three mos, of the index operation), previous smoker (cessation more than three mos before the index operation), or non-smoker. Steroid treatment was defined as present if listed in the medical records.
The variables included in the treatment-related part of the study were the indication for the index operation (emergency or non-emergency), site of surgery (abdominal, juxtarenal, or endovascularly treated thoracic), and type of intervention (EVAR or OR). Data on aneurysm size, operative time, and peri-operative complications such as the need for blood transfusion, blood loss, as well as the length of the hospital stay were collected. Data pertaining to time to graft infection after the index operation, CT scan findings, or positive culture results and the number of surgical interventions or re-interventions between the index operation and confirmed graft infection also were recorded. Positive culture results were included from the time of confirmed graft infection. Earlier cultures, not pertaining to graft infection, were excluded. The culture specimen was, as far as possible, obtained directly from the graft itself or the surrounding aortic tissue. If no such culture results were found in the records, the results from blood, urine, and airways were used. Surgical interventions or re-interventions were defined as any type of surgery, including re-operations after the primary aortic operation.
Additional variables documented were the method of treatment of the graft infection, treatment type (conservative or surgical reconstruction), and follow-up time from the index operation to the last recorded appointment. Follow-up data regarding the outcome of treatment, including death from graft infection (verified by autopsy or according to the certificate of death based on the judgment of the physician in charge), cases under surveillance for graft infection, death from causes other than graft infection, and cases lost to follow-up were recorded.
Statistical analysis
The variables were compared for the different groups. The D'Agostino-Pearson omnibus test was used to determine whether the data were normally distributed (p > 0.05 indicating normality). Medians were used as the measure of central tendency for ordinal and continuous variables and interquartile range (IQR) as indicator of data spread. Comparison of medians within the groups was performed by the Mann-Whitney U test. The Fisher exact test was used for categorical variables. A value of p < 0.05 was considered significant.
Results
Patient characteristics and co-morbidities
A total of 219 medical records were reviewed, yielding 29 patients (26 male, 3 female) with verified AGI. The patients treated by an emergency index procedure were older than the other patients (77 vs. 69 y; p = 0.03). Patient characteristics, co-morbidities, and other risk factors are presented in Table 1. The median follow-up was 69.2 months (IQR 109.5; range 3.2 mos–15.8 y) after the index operation.
BMI = body mass index; COPD = chronic obstructive pulmonary disease; DM = diabetes mellitus; IQR = interquartile range; NS = non-significant (because of small number of observations); SD = standard deviation; TIA = transient ischemic attack. Missing cases: a = 3; b = 5; c = 3; d = 4; e = 4; f = 3; g = 4; h = 8; i = 3 in total; j = 5. In addition, data were missing regarding certain variables not mentioned in the table. For aneurysm size 5 cases, operative time 15, blood loss 13, blood transfusion 18, length of hospital stay 4, time to graft infection 6, and surgical interventions and/or re-interventions 7.
Index operation
Of the 29 patients, there were 24 with aortic aneurysms, three with AIOD, one with type B aortic dissection, and one with liposarcoma affecting the aorta. There were 26 abdominal lesions treated with either EVAR or OR. There were three thoracic cases that underwent EVAR. A majority of the patients were treated on a non-emergency basis (19 vs. 10)(Fig. 1). The median size of the aneurysms was 65 mm (IQR 11 mm), and there was no significant difference in aneurysm size between the emergency and non-emergency cases. The median operative time of the index operation was 241.5 min (IQR 203.5 min) and was similar for the two groups. The median blood loss was 1,250 mL (IQR 2,537.5 mL) for all patients, and was higher in the emergency operation group at 5,000 mL (IQR 2,700 mL) compared with 1,100 mL (IQR 925 mL) in the non-emergency group (p = 0.015). The median volume of blood transfused was 500 mL (IQR 500 mL) for all patients, and there was no significant difference between the groups. The median length of hospital stay post-operatively was 7 d (IQR 6 d) for all patients, again with no difference between the groups.
Graft infection
The overall incidence of graft infection was 1.4% (29/2026) and was similar for non-emergency and emergency cases. The incidence among patients treated endovascularly was 1.4% compared with 1.9% for patients treated with open repair. The median time to graft infection after the index operation was 3.2 y (IQR 4.9 y) for all patients, and there was no difference between the non-emergency and the emergency group. The median number of surgical interventions and re-interventions between the index operation and the onset of infection was two (IQR four) for all patients, and there was no significant difference between the emergency and non-emergency cases. The median time from infection diagnosis to surgical treatment was 30 d (IQR 30.5 d).
Culture results were positive in 22 patients (76%), 15 among the non-emergency surgery group and seven from the emergency surgery group. The slight majority of patients (n = 14) had polymicrobial infections; a single agent was identified in eight cases. Among the fungal agents, Candida spp. were the most common, and among the bacterial agents, the most common type was Enterococcus spp. A total of 67 positive culture results were found among the patients, where the non-emergency group accounted for 75%. The distribution of infectious agents within the groups is shown in Figs. 2 and 3.
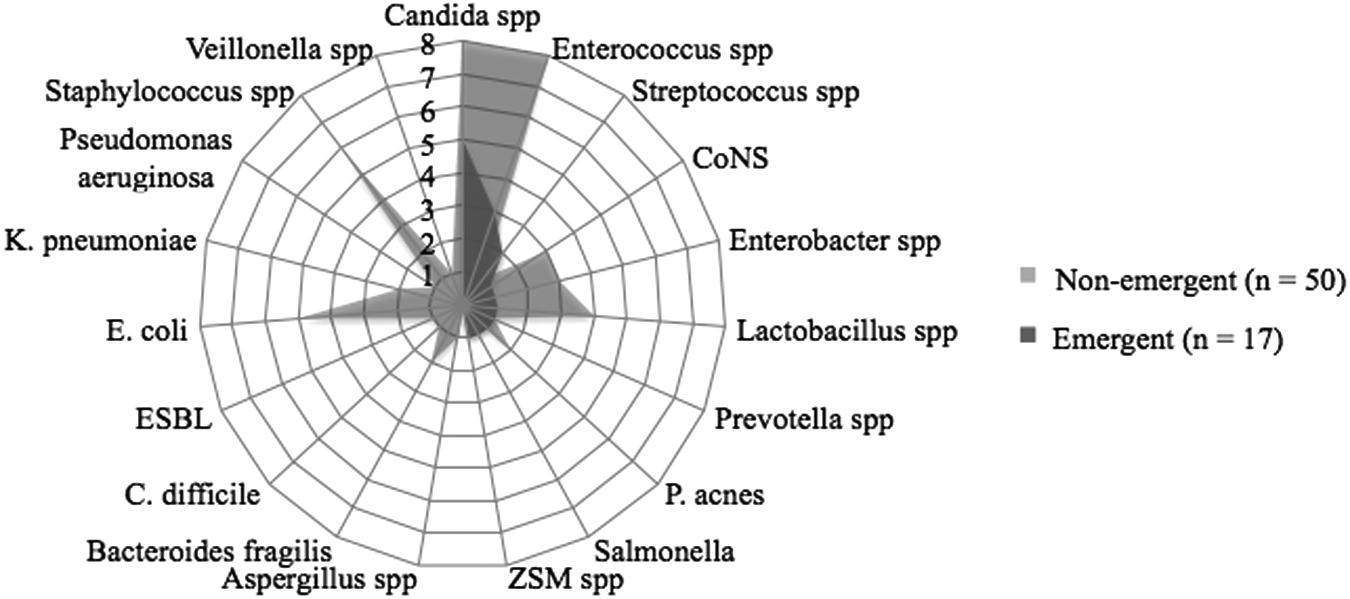
Distribution of infectious agents in the emergency and non-emergency groups (N = 67). Abbreviations: C. difficile = Clostridium difficile; CoNS = coagulase-negative Staphylococcus; ESBL = extended-spectrum beta-lactamase; E. coli = Escherichia coli; K. pneumoniae = Klebsiella pneumoniae; P. acnes = Propionibacterium acnes; ZSM = Zygosaccharomyces.
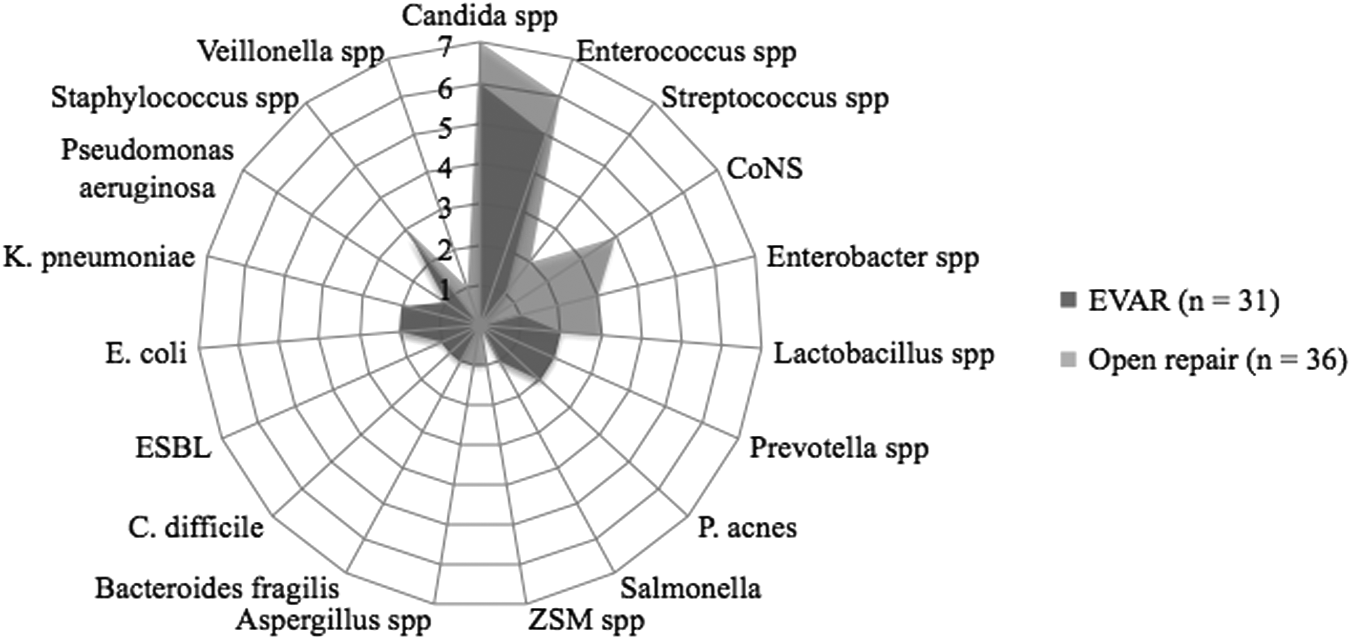
Distribution of infectious agents in the endovascular and open repair groups (N = 67). For abbreviations, see Fig. 2.
Complications and treatment
Nineteen patients were treated conservatively with pharmaceutical therapy and ten were treated surgically for AGI Figure 4. Among the conservatively treated patients, 5% (1/19) were free of signs of infection at the last visit compared with 30% (3/10) of the surgically treated. There were five patients with early onset of infection (≤3 mos), of whom three had emergency surgery as the index operations and two had non-emergency surgery. Among the three patients in the emergency group, infection was diagnosed after 67, 86, and 89 d. The infectious agents were Salmonella, Enterococcus faecalis, Candida spp., Proprionibacterium acnes, and Zygosaccharomyces spp. One patient was treated surgically with adjuvant lifelong antibiotics and survived seven y. The second patient was treated conservatively and survived three mos. The third patient was lost to followup, still alive.

Outcome of treatment for graft infection.
In the non-emergency early-onset group, the infection was diagnosed in the two patients after 51 and 86 d, and the infectious agents found were Candida spp., P. acnes, and Escherichia coli. Both patients were treated conservatively, one with antibiotics for one y, who currently is free of signs of infection, and the other with lifelong antibiotics, who survived 11 mo.
Among the 29 patients, there were five with aorto-enteric fistulae. Two were treated conservatively for infection, and both died (two d and 5.5 y after the diagnosis of AGI). Among the three who were treated surgically, one is alive, and two died from sepsis 8 mos and 5.5 y after their AGI infection diagnosis.
Survival
The all-cause mortality rate for the non-emergency surgery group was 53% and that for the emergency group 80% during the entire time of follow-up (range 3.2 mos–15.8 y). The mortality rates were 74% for the conservatively treated and 40% for the surgically treated. In the conservatively treated group, 57% (8/14) of the deaths were caused by graft infection compared with 25% (1/4) in the surgically treated group (Fig. 4). Survival and outcome for patients treated surgically and conservatively are presented in Tables 2 and 3, respectively. Survival is known for six of the eight conservatively treated patients who died from graft infection, where five of the six patients died within one y from the diagnosis of AGI.
AXBF = axillobifemoral; E = emergency; MOD = multi-organ dysfunction; NAIS = neo-aortoiliac system; N = non-emergency.
AEF = aortoenteric fistula; MOD = multi-organ dysfunction.
Discussion
Aortic graft infection is a feared complication of aortic surgery, but fortunately, its incidence—as confirmed in this population-based series covering a decade of aortic surgery— is low. The overall incidence of AGI was 1.4%, which correlates well with findings in previous studies [1,16,21,22]. The other main findings from this study were the similar rates of infection and time to infection for patients in the emergency and non-emergency surgery groups. Furthermore, better long-term survival was found for patients treated surgically compared with those treated conservatively. Previous research consists mainly of single-center studies with relatively small cohorts and heterogeneous patient populations that do not differentiate between EVAR and OR and where there is a general lack of data on the long-term clinical outcome [13–18]. This is reflected in the absence of a consensus regarding the treatment of these patients [2,12,23,24].
Surgical treatment for AGI resulted in better long-term clinical outcomes in both the emergency and the non-emergency groups, with higher rates of survival and fewer deaths caused by infection than in the patients having conservative management. Our findings correspond well with recently published litterature, showing a generally better outcome in patients treated surgically [1,9,14,21,25]. There are, however, reports that have shown similar mortality rates in surgically and conservatively treated patients [13,26]. This disagreement emphasizes the need for further studies with larger samples to differentiate better the outcomes of each treatment modality. However, with support from the majority of studies in this area, surgical treatment currently is the preferred option for AGI.
The difference in median age between the emergency and non-emergency patients was expected. This difference is commonly reported [27] and is believed to be a product of patient selection. The emergency and non-emergency groups had the same incidence of AGI and time to infection. This is in contrast to the generally accepted fact that emergency surgery increases post-operative complication and mortality rates [19]. The peri-operative blood loss is a variable that plays a significant role in the development of post-operative complications, and it has been shown, both in this study and in previous research, to be greater in emergency cases [19,28,29]. However, more recent findings have shown similar results, where emergency and non-emergency cases have the same incidence of AGI [16]. The explanation may lie in the shifting trends in the management of emergency cases, whereby more patients are treated with EVAR, leading to shorter operating time and less per-operative blood loss, at the same time as more high-risk patients—older and more susceptible to infection—are treated prophylactically.
The majority of patients with positive culture results were treated after a non-emergency index operation. There were 15 patients (68%) who accounted for 75% of the total number of infectious agents found in all cultures. The variability in the accessibility for cultures of AGI introduces a degree of uncertainty as to the relevance of the agents isolated, but nonetheless, it forms the basis for the choice of antibiotic/anti-fungal treatment. In a recent review by Kilic et al. [9], the difficulties of obtaining positive culture results from areas close to the graft are highlighted. It also is emphasized that negative cultures cannot exclude AGI, particularly in late-onset infections with low-virulence and slow-growing bacteria [9]. Because of the difficulties inherent in obtaining accurate culture results, findings on CT scans indicative of AGI were the only diagnostic methods used in some cases.
Because of the difficulties in obtaining culture results, it also is difficult to determine the etiology of infection. The relatively long median time to AGI (3.2 y) is suggestive of either a secondary infection or early infection with low-virulent agents as the cause of AGI. Bacteriemia (present or previous) or mechanical erosion into adjacent tissue often are seen during the investigation of AGI. However, because of the retrospective nature of this study, it is not possible to draw any conclusions regarding the primary cause of AGI.
The major limitations in this study are inherent in its retrospective nature, consisting of missing data and the lack of standardized definitions of various variables, including graft infection. The difficulty of obtaining reliable results from cultures also contributes. Further, a multivariable analysis was not performed because of the small number of observations. On the other hand, the length of follow-up strengthened by the high validity of Swedvasc [19], coupled with the thorough review of the medical records and centralized care of AGI patients, increases the generalizability of the results.
The initial analysis of all patients identified in the electronic chart system who had undergone aortic operations with a post-operative complication yielded a greater number of patients than were included in the study because of verified AGI. This was secondary to the ICD codes used for various vascular complications, which did not necessarily concern AGI. Therefore, 190 of the 219 patients initially identified were verified as not having AGI. Further, no meaningful comparison between abdominal and thoracic cases was possible, given the small number of thoracic cases, which all were treated with EVAR.
In the absence of a consensus on the most appropriate diagnostic and treatment algorithm for AGI, the findings of this study provide some insight into the long-term clinical outcome for both treatment modalities. Surgical treatment for infection had the better long-term outcome. This could be of importance for future formulation of guidelines, especially in cases where the choice of method teeters between surgical and conservative treatment.
Conclusions
This population-based retrospective investigation of AGI confirms its previously reported low incidence. Surgical treatment combined with adjuvant antibiotic/anti-fungal treatment appears to result in a higher rate of eradication of infection and better long-term survival than conservative treatment.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest relating to this article.
This research was supported by the Swedish Heart–Lung Foundation (Hultgren) and through the regional agreement on medical training and clinical research (ALF) between Stockholm County Council and the Karolinska Institutet (Hultgren).
Conception and design of this study were by A.D. and R.H. Data collection was performed by J.P., A.D., and P.G. Statistical analysis was done by J.P. and R.H. Analysis and interpretation was carried out by all the authors. The writing was done by J.P., A.D., and R.H. All authors were involved in the critical revision of and gave final approval to the manuscript. Overall responsibility for the project was in the hands of R.H., who also obtained the funding that supported the study.