
Abstract
Abstract
Background:
The incidence of gram-negative multi-drug–resistant (MDR) infections is increasing worldwide. This study sought to determine the incidence, clinical profiles, risk factors, and mortality of these infections in general surgery patients.
Patients and Methods:
All general surgery patients with a clinical infection by gram-negative MDR bacteria were studied prospectively for a period of five years (2007–2011). Clinical, surgical, and microbiologic parameters were recorded, with a focus on the identification of risk factors for MDR infection and mortality.
Results:
Incidence of MDR infections increased (5.6% to 15.2%) during the study period; 106 patients were included, 69.8% presented nosocomial infections. Mean age was 65 ± 15 years, 61% male. Extended-spectrum β-lactamases (ESBL) Escherichia coli was the most frequent MDR bacteria. Surgical site infections and abscesses were the most common culture locations. The patients presented multiple pre-admission risk factors and invasive measures during hospitalization. Mortality was 15%, and related to older age (odds ratio [OR] 1.07), malnutrition (OR 13.5), chronic digestive conditions (OR 4.7), chronic obstructive pulmonary disease (OR 3.9), and surgical re-intervention (OR 9.2).
Conclusion:
Multi-drug resistant infections in the surgical population are increasing. The most common clinical profile is a 65-year-old male, with previous comorbidities, who has undergone a surgical intervention, intensive care unit (ICU) admission, and invasive procedures and who has acquired the MDR infection in the nosocomial setting.
T
Many risk factors for MDR infections have been identified, including advanced age, comorbidities, neoplasia, long hospital stays, intensive care unit (ICU) admissions, use of invasive devices, and previous antibiotic therapy [7–9]. The gram-negative bacteria present in the hospital environment can contaminate medical devices and be carried on health care workers' hands. Increased complications, mortality, and costs have been demonstrated not only in this setting [10,11], but also in the community, where MDR infections are starting to appear and can be the cause of failure of empirical antibiotic regimes [12,13].
Among the increasing number of studies reporting on resistant gram-negative bacteria, we find two main groups. First, those focusing on epidemiology, incidence trends, microbiology and susceptibility patterns, which are mainly population-based or reporting on surveillance programs [14–16]. The second type are clinical studies of risk factors, mortality, or other clinical parameters [17] that focus on specific populations such as ICU patients, or study a specific location of infection (bacteremia, urinary tract infection, cholangitis, etc.) [18–20]. However, studies with a specific focus on surgical patients that consider surgical parameters or the complications that can arise from MDR infections in this specific population are lacking. The translation of these microbiologic considerations to the clinical setting of surgical patients is straightforward: abdominal, post-operative, or health-care associated infections by MDR bacteria in surgical patients can be the cause of poor outcomes, complications, poor response to empirical antibiotic regimes, and increased morbidity and mortality.
From a previous retrospective study [21] we learned that there was a high incidence of ESBL infections in our institution, and despite medical patients being the most common, 28% of isolates belonged to surgical wards. After internal medicine, the general surgery ward presented with the second highest number of isolates. As mentioned, with the increasing importance of gram-negative infections and emerging resistance worldwide, we believed this needed further investigation. The goal of our study was to determine the actual incidence of all gram-negative MDR bacteria in our general surgery department and describe the clinical profile, characteristics, and possible risk factors of patients presenting with these infections.
Patients and Methods
Study population
This prospective study included all patients presenting with a clinical infection by a gram-negative MDR bacteria admitted to the General Surgery Department in La Princesa University Hospital, a tertiary-care 600-bed university hospital in Madrid, Spain. The study was reviewed and approved by the institutional ethics committee, and because this observational study did not modify surgeons' clinical practices, no informed consent was required.
Included in the study were all adults (aged >18) admitted to the general surgery department in the five-year period between January 2007 and December 2011. They all had at least one positive culture for a gram-negative MDR bacteria (any location), associated with clinical signs or symptoms of infection. The patients were included prospectively and followed from the moment of diagnosis of an MDR infection, and data were reviewed from their medical charts or by direct interview with the patient. Patients with exclusive hospitalization in the ICU were excluded from the study to avoid bias, as they represent a different population with specific risk factors.
Bacteria and infection definitions
The gram-negative MDR bacteria selected for study were all species of Enterobacteriaceae in which ESBL, AmpC, or other β-lactamases were detected, Pseudomonas aeruginosa with confirmed resistance to three or more therapeutic antimicrobial groups, and Stenotrophomonas maltophilia whenever detected. Only clinical isolates (not colonizations or asymptomatic carriers) were included and patients were included only once, although multiple locations of infection were considered in the same patient if present. Antimicrobial susceptibility studies for each MDR bacteria were collected from the microbiology report. If the patient presented infection by more than one species of MDR bacteria, this was also registered (as second isolation).
The MDR infection was classified as community-acquired (detection of MDR bacteria less than 48 h from admission), nosocomial (detection more than 48 h from admission), or health-care associated (in institutionalized patients, recent hospitalization, or frequent contact with the hospital by means of day care, dialysis, etc.).
Microbiologic methods
Clinical samples were collected from patients and processed following standard procedures. They were classified as: surgical site infection, abscess, drain, urine, bronchial aspirate, blood, catheter, exudates, pressure ulcer, or others.
Bacterial identification and susceptibility tests were determined using MicroScan® Negative MIC panel type 32 (Siemens, Munich, Germany). Extended-spectrum β-lactamase production confers resistance to penicillins, cephalosporins, and aztreonam, and can generally be inhibited (at least in vitro) with inhibitors such as clavulanate or tazobactam. Extended-spectrum β-lactamase confirmatory tests were performed using broth microdilution following Clinical and Laboratory Standards Institute recommendations [22], using the MicroScan ESBL plus panel (Siemens) that includes cefpodoxime, cefotaxime, cefotaxime/clavulanate, ceftazidime, and ceftazidime/clavulanate. A threefold concentration decrease in a minimum inhibitory conentration (MIC) for either antimicrobial agent tested in combination with clavulanic acid versus its MIC when tested alone was considered as ESBL positive. Double-disk method and E-Test (bioMérieux, Durham, NC) were also used in those cases in which results were not conclusive. The identification of MDR P. aeruginosa and S. maltophilia was performed by disk diffusion (metalo-β-lactamase inhibition with ethylenediaminetetraacetic acid [EDTA]), microdilution, or specific E-tests. Molecular identification was the last resource for pathogens not identified otherwise.
Patient characteristics
Patient demographics (age, gender, body mass index), Charlson index, American Society of Anesthesiologists (ASA) status, comorbidities, malignancies, previous surgical procedures, previous hospitalization, invasive procedures, and antibiotic use (longer than six months) were retrieved. All procedures and invasive measures performed during hospital admission and prior to the diagnosis of the MDR infection were collected (catheters, tubes, mechanical ventilation, post-operative ICU admission). Details on the location of the surgical pathology, elective or emergent procedure, surgical approach, U.S. Centers for Disease Control (CDC) classification and National Nosocomial Infections Surveillance (NNIS) Index, incidence of re-operation, and cause were also included for each patient. Overall post-operative complications were registered using the Clavien-Dindo Classification, including mortality (grade V). To determine possible risk factors for mortality among patients with MDR infections, both groups (surviving versus deceased) were compared.
Statistical analysis
A specific database was developed for the study by the hospital's biostatistician, ensuring patient confidentiality. Descriptive statistics were calculated to describe the study population. Patient's characteristics and clinical parameters were compared using χ2 or Fisher exact test (two-tailed) for categorical parameters and Student t-test for continuous parameters. Bonferroni test for multiple comparisons was used for the 2 × 2 (post hoc) comparisons. Statistical significance was set at p < 0.05. When analyzing risk factors for mortality, significant factors in univariable models were included in a multivariable logistic regression model. All statistical analyses were performed using SPSS® for Windows, version 18.0 (SPSS Inc. Released 2009. PASW Statistics for Windows, Version 18.0: SPSS Inc., Chicago, IL).
Results
Study population and Incidence of MDR infection
One hundred six patients admitted to our general surgery department presented a clinical infection by gram-negative MDR bacteria during the study period, with an average of 26 cases per year. To contextualize these data, incidence rates of MDR infection were calculated considering all general surgery patients with infection and overall general surgery admissions (Table 1).
MDR = multi-drug resistant.
Microbiologic results
Extended-spectrum β-lactamase–producing E. coli was the most frequent MDR bacteria throughout the study period. The distribution of isolates (classified by main resistance groups or species) per year is shown in Figure 1. A total of 130 MDR bacteria were isolated, 106 as first isolation and 24 as second. The most common were ESBL-producing E. coli (32.5%), MDR P. aeruginosa (23.5%), and ESBL-producing Klebsiella pneumoniae (12%), as shown in Supplementary Table S1 (see online supplementary material at http://www.liebertpub.com/sur).
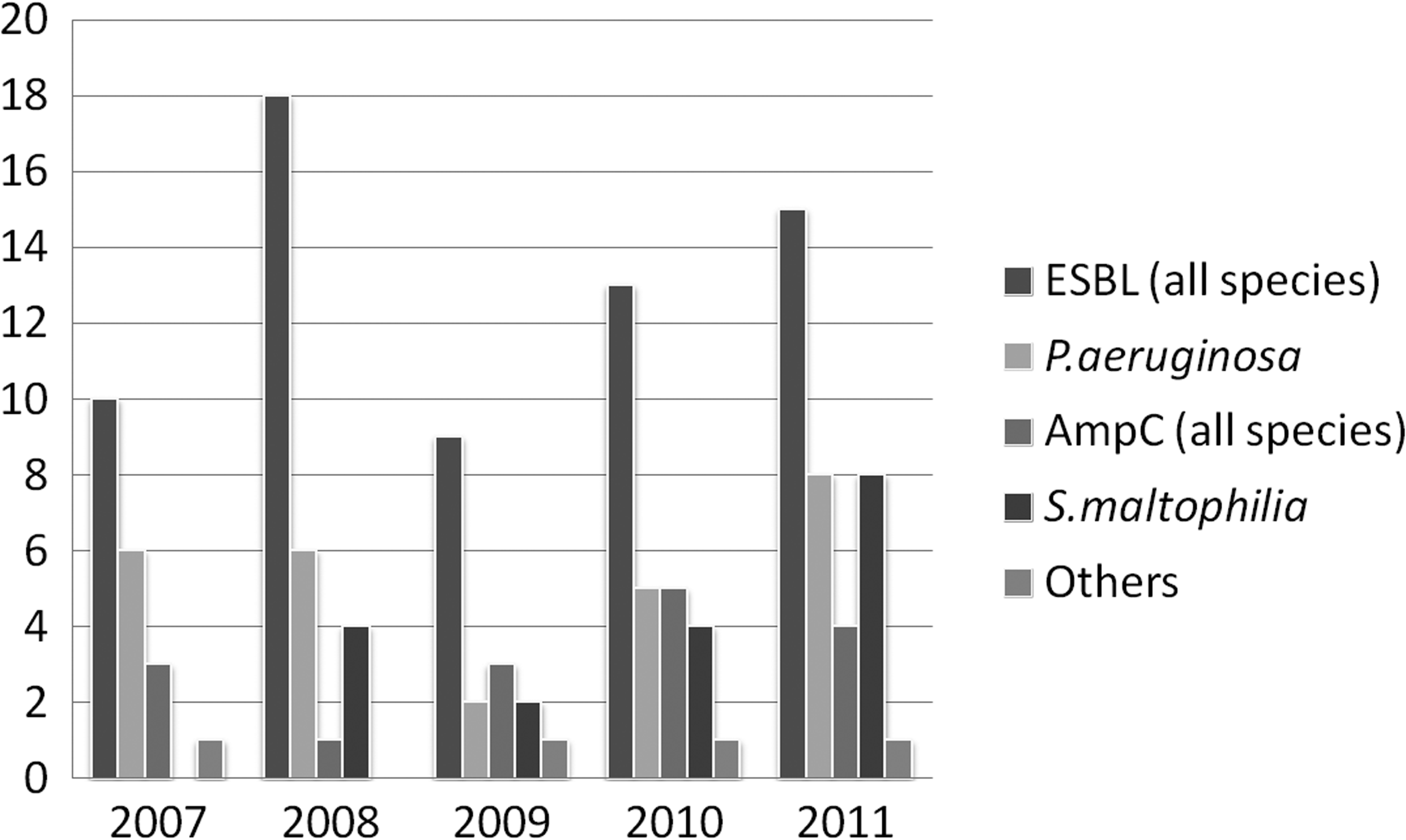
Incidence (number of cases) of multi-drug resistant (MDR) bacteria (classified by resistance groups or species) per year.
Multi-drug–resistant infections (by acquisition) were most frequently nosocomial (74 cases; 69.8%), followed by community-acquired (16%) and health-care associated (14.2%). Extended-spectrum β-lactamase–producing bacteria were most common as first isolations, followed by P. aeruginosa, which was also isolated as second MDR bacteria in 47.4% of cases. Other non-resistant micro-organisms cultured prior to the MDR infection were gram-positive bacteria in 50 patients (47.2%), gram-negative bacteria in 42 (39.6%), and yeasts in 39 (36.7%).
Location of MDR infection and antimicrobial susceptibility
The most common surgical conditions and interventions of patients by location were the colon (18%), pancreas (15%), and biliary tree (13%; Supplementary Fig. S1; see online supplementary material at http://www.liebertpub.com/sur). The locations sampled for culture where MDR bacteria were identified are shown in Table 2. When analyzing the bacterial species by culture location, ESBL-producing E. coli was significantly more present in abscess isolates (p = 0.001), MDR P. aeruginosa in exudates (p = 0.001), drains (p = 0.009) and bronchial aspirates (p = 0.02), and S. maltophilia in drains (p = 0.009).
Some patients presented the same bacteria in multiple locations upon first isolation.
The susceptibility patterns of the four most common bacterial species are shown in Figure 2. Extended-spectrum β-lactamase–producing bacteria presented associated resistance to other antibiotic groups such as quinolones, tobramicin and cotrimoxazole, but were susceptible to all carbapenems. Multi-drug resistant P. aeruginosa presented a high percentage of resistance to carbapenems, gentamicin, and quinolones, however, more than 70% of isolates were susceptible to piperacillin/tazobactam and amikacin, and more than 90% to colistin. Stenotrophomonas maltophilia, intrinsically resistant to carbapenems, was also resistant to piperacillin/tazobactam, gentamicin, quinolones, and aztreonam in most isolates. However, cotrimoxazole maintained a good susceptibility pattern (78%). AmpC bacteria were mostly susceptible to carbapenems (99%), amikacin (100%), gentamicin (88%), and presented increased resistance to (50%) piperacillin/tazobactam and ciprofloxacin (27%) (data not shown in Fig. 2).
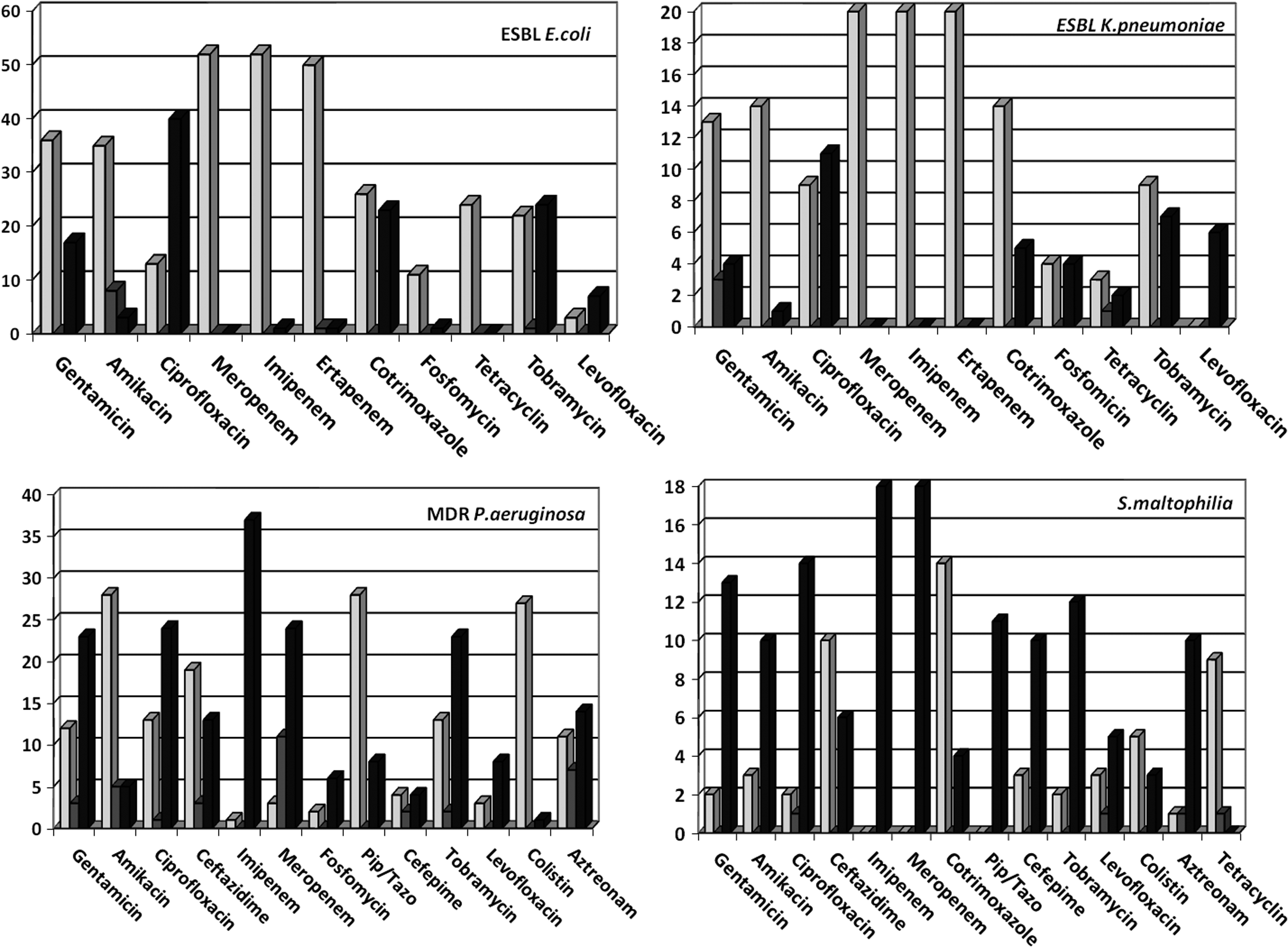
Susceptibility patterns of the four most common bacterial species. White = susceptible; gray = intermediate; black = resistant.
Patient characteristics and clinical parameters
Demographics, comorbidities, and identified pre-admission risk factors of patients are summarized in Table 3. During hospital admission, and prior to the diagnosis of MDR infection, all invasive measures and procedures, including the most frequent empirical antimicrobial regimes are detailed in Table 4. Most patients had undergone a surgical intervention with mechanical ventilation and post-operative ICU admission, and had tubes and catheters present at the time of MDR bacteria infection detection. In patients receiving blood transfusions, the mean was 3.37 (±2.6) times, and the mean number of blood units 6.6 (±5.9). Beta-lactam/inhibitor combinations, carbapenems, and quinolones were the most common empirical antibiotic regimes. Specific parameters related to the surgical procedure are shown in Table 5.
SD = standard deviation; UTI = urinary tract infections; ICU = intensive care unit; ASA = American Society of Anesthesiologists.
MDR = multi-drug resistant; ICU = intensive care unit.
CDC = U.S. Centers for Disease Control; = NNIS = National Nosocomial Infection Surveillance; NA = not applicable; MDR = multi-drug resistant.
Outcomes
The global mean hospitalization was 53 ± 53 d, with a median of 36.5 d (range, 3–309). The overall mortality rate was 15%. Deceased patients were older (mean, 72 y) than surviving patients (63.8 y). The multivariable analysis identified as pre-admission risk factors for mortality: malnutrition (OR 13.5), chronic digestive pathology (OR 4.7), and chronic obstructive pulmonary disease (OR 3.9). Related to the hospital admission, the only factor associated to mortality was surgical re-intervention (OR 9.2), as shown in Table 6.
OR = odds ratio; CI = confidence interval; COPD = chronic obstructive pulmonary disease.
Discussion
In this single-center prospective study, the incidence of gram-negative MDR infections in general surgery patients increased over a period of five years. The profile of the infected patient was a 65 year-old male, with a nosocomial infection, previous comorbidities and risk factors, including recent surgical intervention, ICU admission, and invasive procedures during a long hospitalization.
The reported incidence of our institutional MDR bacteria remained among the estimated national percentages, reported by epidemiologic studies such as the European Antimicrobial Resistance Surveillance System (EARSS) report from the European Centre for Disease Prevention and Control (ECDC) [23]. The general trend in epidemiologic studies about MDR bacteria is that both the incidence and prevalence are increasing worldwide. There is a wider distribution of specific clones, and an increasing report of endemic outbreaks. Variations in the incidence per year and resistance patterns highlight the importance of local epidemiology, as each institution has endemic pathogens to consider. In our population, ESBL and AmpC-producing bacteria can be both nosocomial and community acquired, whereas other gram-negatives such as P. aeruginosa and S. maltophilia continue to be mostly hospital-acquired or health-care associated infections.
The incidence of MDR infections among hospitalized patients varies between departments and type of patients. When reviewing institutional studies on epidemiology of MDR bacteria, we find variable (usually low) inclusion of surgical patients and isolates. Buke et al. [8] report a 7.5% incidence of ESBL bacteria in 439 patients hospitalized for more than 30 d in a 900-bed university hospital in France. Among them, only 22.5% were in surgical wards, with only 10 ESBL isolates identified from surgical patients, either infected or colonized. In a national study by the GEIH group including 44 Spanish hospitals [15], 254 ESBL-producing E. coli samples were studied; among them only 25 belonged to intra-abdominal infections (10 biliary) and only 16 were classified as surgical site infections.
Intra-abdominal infections are one of the most common causes of surgical admission, and surgical infections represent the most common cause of nosocomial infection, as reported by CDC [24]. The profiles and special characteristics of surgical patients demand specific studies to understand the risk factors, locations, and outcomes of MDR bacteria in these scenarios. An interesting worldwide initiative is the SMART study [25,26], that analyzes intra-abdominal culture samples specifically, informing on the most common bacterial species and resistance trends. However, it lacks specific clinical data and does not consider other surgical samples (such as wound infections), that can be most representative of infection in surgical populations. As demonstrated in the present study, the most common culture locations of MDR bacteria were surgical site infections and abscesses.
In a Portuguese study [27] post-operative wound infections and soft tissue infections by Enterobacteriaceae were reviewed specifically, with a high incidence of resistance and ESBL production, and 18% co-infection with other resistant bacteria, such as P. aeruginosa. This agrees with our present findings in which nosocomial patients can present a second MDR bacteria isolate, and associations of MDR gram-negatives are not uncommon. In the same line of investigation, Seni et al. [28] report an alarming increase of resistance in isolates from surgical site infections in Uganda. Patients were mostly from gynecology and general surgery wards, and swabs taken from the wounds were positive in 68%, with 23.7% of Escherichia coli, and more than 75% of ESBL production among Enterobacteriaceae species. Montes et al. [29] studied the incidence of resistance (ESBL production) in surgical site infections of patients treated for cancer in an oncology center in Mexico. Patients with untimely or prolonged antibiotic prophylaxis or receiving cephalosporins post-operatively had a higher risk of ESBL infections. Also, the organ/space location of infection had a higher risk of ESBL isolation. In the present study, organ/space infections were the most common post-operative complication among our patients.
Another approach to MDR infections in surgical populations has been the analysis by specific location. In our study, colorectal and hepato-biliary locations of MDR infection were the most common, but these are also the most common surgical conditions. Considering other specific surgical locations, published studies are limited. In a study from India [30], were MDR infections are highly prevalent, the incidence of ESBL-producing bacteria in patients treated surgically for appendicitis was specifically addressed. It concluded that routine cultures were not necessary (and costly) and should only be taken in case of complications and that empirical antibiotic regimes should only be changed in high-risk patients or after culture confirmation. This point of view differs from the trend in Europe, where cultures are encouraged and early detection of MDR bacteria is considered a priority to avoid treatment failures.
Post-operative peritonitis has been a most developed subject of study, because patients are usually in critical care units, present various risk factors for MDR infections, and have received broad-spectrum antibiotics. Montravers et al. [31,32] demonstrated that the emergence of MDR organisms in post-operative peritonitis was related to inadequacy of empirical treatment or prolonged use of broad-spectrum antibiotics. They conclude that not all regimes proposed by guidelines such as the Infectious Diseases Society of America (IDSA) [33] are acceptable, with carbapenems or antibiotic combinations being the most desirable to avoid treatment failures. However, again these surgical ICU patients were a specific population, and not representative of the general surgery patients in a common hospitalization ward.
Whereas hospital-acquired infections remain the most common source of MDR bacteria in surgical patients, we also find an increasing awareness of the importance of community-acquired infections and asymptomatic fecal carriers [34]. This can be especially relevant in endemic populations, household contacts of patients with demonstrated MDR infections, or travelers. The so-called environmental acquisitions coming from farming industry, agriculture, or food processing can also be a source of infection in the community, still not completely understood [35]. Associated with this capacity of gram-negative bacteria to colonize, become part of gut flora, and transfer resistance plasmids (even inter-species), we find an increased risk of a new infection in case of a new aggression or selection of bacterial populations by new antimicrobial treatments [36]. This has also been considered as a mechanism of bacterial spread, considering fecal carriers as reservoirs. In a multicenter study from Sweden [37], the prevalence of fecal carriage of antibiotic-resistant bacteria in patients with acute surgical abdomen was specifically reviewed. Rectal swabs from all patients admitted with intra-abdominal infections were performed and tested for ESBL production. A high resistance rate to the most commonly used antibiotics (such as cephalosporins) was reported and the isolation of ESBL-producing strains reached 5%.
Mortality by MDR bacteria has been analyzed widely, especially in critically ill patients, in studies evaluating empirical antibiotic adequacy and in clinical scenarios such as bacteremia. There is high-quality evidence demonstrating an increased mortality by MDR bacteria, with risk factors such as inappropriate empirical therapy, previous hospitalization, or nosocomial infection and comorbidities (cancer, immune suppressors, hepatopathy, etc.) clearly identified in various studies [7,38,39]. In the present study, MDR infection-related mortality in general surgery patients was associated with age and the presence of comorbidities such as malnutrition, chronic digestive conditions, and chronic obstructive pulmonary disease. According to the specific surgical condition, the presence of a re-intervention for complications was also associated to a higher risk of mortality. It could be analyzed whether these factors would increase mortality in any kind of infection, as comorbidities represent the patient's poor pre-operative condition, and complications leading to re-intervention consume the last resources to fight against infection. However, there is evidence that among patients with the same clinical conditions and comorbidities, the presence of an MDR infection is a risk factor in itself [7,11,19].
In conclusion, MDR infections in the surgical population are increasing and these patients present specific characteristics and a distinct clinical profile. Nosocomial infections in patients with surgical interventions, invasive measures, and long hospitalizations are the most common, but community-acquired and health-care associated MDR infections are starting to appear and should be suspected by investigating risk factors (such as previous antibiotic therapy or hospitalization). The surgical site of infection differentiates these patients from others in medical wards, and specific risk factors for mortality have been identified, which include previous comorbidities and surgical re-intervention.
Limitations of the study
Because of the low incidence of gram-negative MDR infections in general surgery patients the sample and statistical power may be insufficient to evaluate some potentially important parameters or risk factors. As a descriptive, non-comparative study, the evaluation of specific risk factors against controls was not performed. As a single-center study, results may not be representative of other populations. Regarding microbiologic methods, molecular identification of specific ESBL, or other enzyme types was not performed, and clonal relations between local community or nosocomial strains were not established.
Footnotes
Acknowledgments
We thank Dr. J.M. Badia, Dr. N. Herrera, and Dr. J. Ruiz-Tovar for their participation as PhD committee and evaluation of this work. We thank the Departments of Microbiology and Preventive Medicine in La Princesa University Hospital for their collaboration and assistance during the study. We thank the Department of Biostatistics (IdiPaz) in La Paz University Hospital for the database development and data analysis. We thank all surgical colleagues from La Paz and La Princesa University Hospitals who have collaborated in this study.
This work was presented as doctoral thesis by Ines Rubio-Perez in the Faculty of Medicine, Universidad Autonoma de Madrid (Spain) in November 2015. Previous (partial/preliminary) data were presented in the following congresses/meetings: Rubio-Pérez I, Pichiule M, Martín-Pérez E, Domingo D, Figuerola A, Larrañaga E. Application of infection control measures for multi-resistant ESBL-producing bacteria among hospitalized general surgery patients: an institutional study. 8th World Congress on Trauma, Shock, Inflammation and Sepsis-TSIS 2010, in conjunction 23rd SIS-Europe Congress on Surgical Infections, 2nd Interdisciplinary Summit on Inflammation. 9–13 March 2010. Munich, Germany.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.