
Abstract
Abstract
Background:
Colorectal surgical procedures (CRS) are associated with the highest surgical site infection (SSI) rate among elective operations. A wide range of patient and surgical characteristics have been identified as risk factors for SSI. Most studies are limited by reliance on retrospective data or subset analysis of data that includes CRS. This study reflects analysis of SSI risk factors using prospectively collected data in an elective CRS population.
Patients and Methods:
We analyzed data prospectively collected as part of a randomized, blinded trial of skin anti-sepsis in elective CRS to identify risk factors associated with SSI, including superficial or deep SSI or cellulitis within 30 days post-discharge. Photodocumentation, patient questionnaires, and blinded review by an attending surgeon were used to identify SSI. Multi-variable logistic regression was used to identify factors significantly associated with SSI and to calculate predicted risks of SSI.
Results:
From 2011 to 2015, 787 patients undergoing clean-contaminated procedures by colorectal surgeons were analyzed as part of a randomized clinical trial. The overall SSI rate was 21.5%. Four variables—incision length, surgical indication, body mass index, and surgical approach—were significantly associated with SSI. Based on these four variables, the predicted risk of SSI ranges from <5% to >60%.
Conclusion:
This study represents the largest prospective investigation of SSI in elective CRS. There is a very wide range of SSI risk after CRS based on both modifiable and non-modifiable factors. Identification of those at the extreme ends of risk may help us both identify and mitigate contributors to infection.
S
The reported rates of SSI after CRS, however, are widely varied and appear to depend on methods of identifying and defining SSI. Many of the existing studies use the American College of Surgeons National Surgical Quality Improvement Program data (ACS NSQIP). Using this retrospectively collected database, the SSI rates after elective colorectal resections range from 9% to 15% [7–9]. In studies involving prospectively collected data, however, these rates are almost always higher; in some series, the SSI rate after elective colorectal resection is as high as 45% [10–13].
A wide range of both patient and surgical characteristics have been identified as risk factors for SSI after CRS, although most of these studies use retrospectively identified SSI as the outcome. Few studies, however, have evaluated risk factors for SSI using a rigorously maintained, prospectively collected database. In this study, we used data collected as part of a randomized, blinded trial of skin anti-sepsis in elective CRS to identify risk factors associated with development of SSI. The use of incision photodocumentation and blinded SSI analysis are unique and provide a more accurate assessment of SSI occurrence. This, in turn, allows for more reliable evaluation of the variations in, and risk factors for, SSI in our patient population.
Patients and Methods
Between 2011 and 2015, 787 patients undergoing clean-contaminated procedures by colorectal surgeons in a university health system were enrolled in a randomized trial comparing the efficacy of two alcohol-based skin preparations in preventing SSI. The study was approved by the Institutional Review Board, and informed consent was obtained from all patients before enrollment. Eligible patients included those 18 years of age or over undergoing an elective clean-contaminated colorectal procedure at one of three participating hospitals.
Exclusion criteria were antibiotic agent use within five days before operation, infected or dirty incision classification, pre-operative plan to leave the incision open, ongoing radiation or chemotherapy, history of laparotomy within 60 days, current abdominal wall infection, and known allergy to chlorhexidine gluconate or iodine. Patients were also excluded if they were participating in any concomitant pre-operative antibiotic or skin antisepsis trial or if they were pregnant or breast-feeding.
During the time of the trial, the majority of patients received mechanical bowel preparation, although bowel preparation was occasionally omitted. Surgeon preference dictated the use of, and type of, bowel preparation. Oral antibiotic agents as part of the pre-operative bowel preparation were not routinely used during the study period. Patients were administered pre-operative intravenous (IV) antibiotic agents and post-operative IV antibiotic agents per the current Surgical Care Improvement Project (SCIP) recommendations at the time of the procedure. More than 90% of the patients received SCIP compliant peri-operative antibiotic prophylaxis.
Outcomes
The primary outcome in this study was the occurrence of any SSI within 30 ± 5 days post-discharge. This included the occurrence of cellulitis, or superficial skin infection or deep skin infection. Centers for Disease Control and Prevention (CDC) definitions were used to classify superficial and deep skin infections [14–16]. Although the CDC does not recognize cellulitis as a post-operative wound complication, we believe that it is a clinically meaningful outcome. As such, cellulitis was included in our outcome measurements. Cellulitis was defined as wound erythema resulting in institution of antibiotic agents.
Clinical assessment
Pre-operative evaluation included a medical history, physical examination, and routine laboratory testing. Peri-operative information including prophylactic antibiotic agents, vital signs, and other relevant information was obtained from anesthesia and nursing records. The surgical site was assessed using a standard assessment form and photographed by a blinded assessor daily starting from post-operative day three to discharge (Fig. 1). Vital signs, laboratory values, relevant post-operative events, and incision culture data, if available, were also recorded.
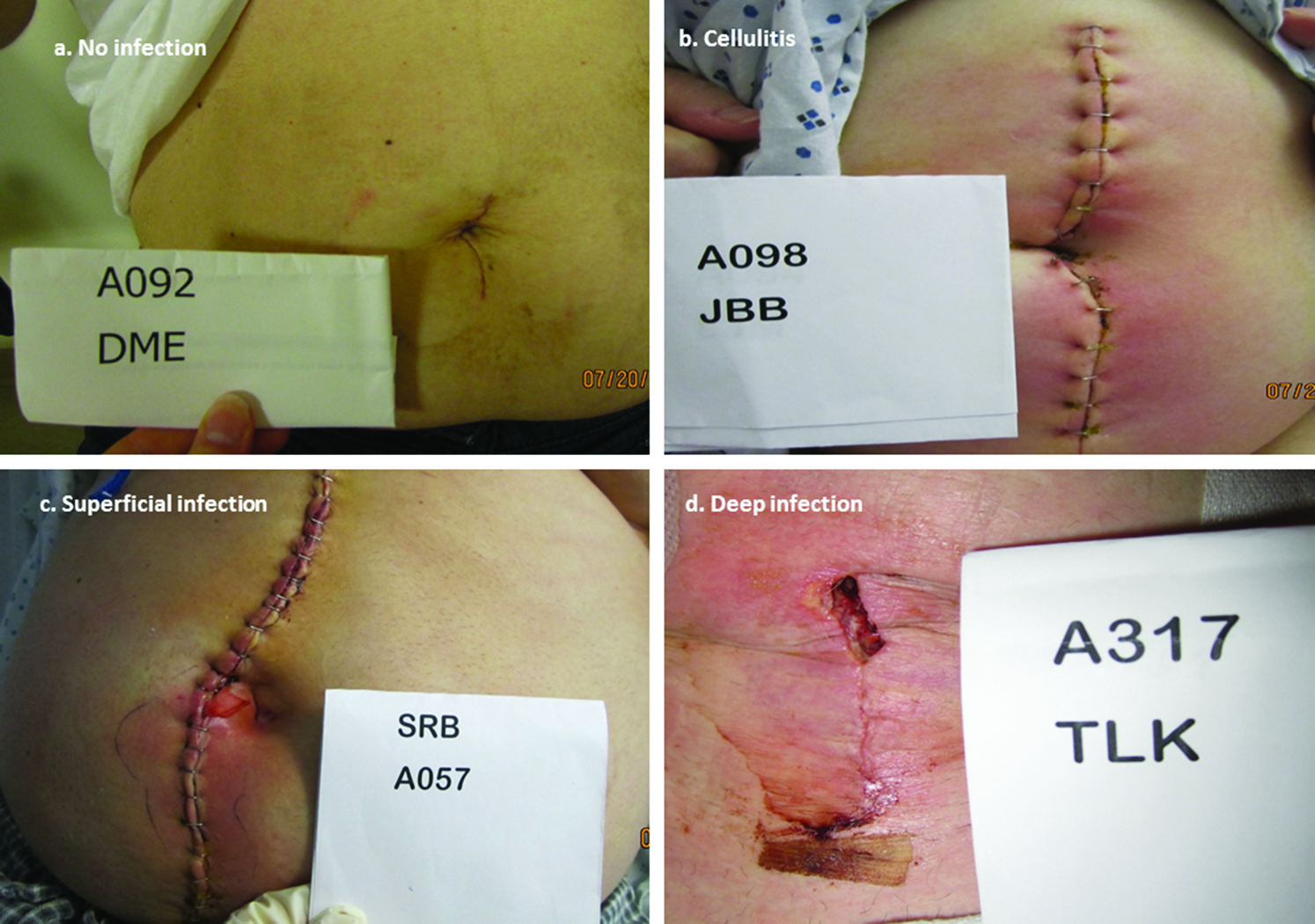
Demonstration of photodocumentation of post-operative incisions.
During post-operative clinic visits, participants completed a questionnaire to help identify possible incision complications diagnosed and treated at another facility. Photodocumentation of the incision was also obtained by a blinded assessor. Patients were monitored for up to 30 ± 5 days after hospital discharge. The questionnaires were acquired during post-operative visits or through phone interviews at 15 ± 5 days and at 30 ± 5 days post-discharge. Follow-up was discontinued if an incision infection was confirmed by culture or by CDC-defined clinical diagnosis. All photographs and other data were reviewed, in blinded fashion, twice by the principal investigator, once within two months of the assessment and a second time, at the end of the study, to make a final determination regarding SSI classification.
Statistical analysis
Univariable associations between occurrence of SSI and patient characteristics were assessed using chi-square tests for categoric variables and t-tests for continuous variables. Significant predictors (p < 0.10) were then included in the multivariable logistic regression model. The association between occurrence of SSI and those significant variables was analyzed using a multivariable logistic regression, with backward stepwise variable selection and a threshold significance of 0.05. The final logistic model included only body mass index (BMI), surgical indication, incision length, and surgical approach (laparoscopic vs. open), as factors significantly associated with SSI. Adjusted predicted probabilities of SSI were then calculated based on the four variables in the final multivariable model. Two-tailed tests were used for all analyses, and statistical significance was defined at p < 0.05. Statistical analysis was conducted using STATA 14.0 (STATA Inc., College Station, TX).
Results
Between 2011 and 2015, 787 patients undergoing clean-contaminated procedures by colorectal surgeons in the health system were analyzed as part of a randomized clinical trial. The overall SSI rate including cellulitis was 21.5%. The rates of cellulitis, superficial skin infection, and deep skin infection were 4.2%, 10.9%, and 6.4%, respectively.
The univariable association between patient factors and the occurrence of SSI is shown in Table 1. Univariable analysis identified seven variables associated with SSI with a p < 0.1; surgical site (colon vs. rectal), indication for operation, BMI, presence of a stoma, open versus laparoscopic approach, incision length, and post-operative hyperglycemia.
SSI = surgical site infection; IB2/10/17 = inflammatory bowel disease; SCIP = Surgical Care Improvement Project; BMI = body mass index.
The results of the backward, stepwise multi-variable logistic regression, starting with these seven variables, are shown in Table 2. Four variables—incision length, surgical indication, BMI, and surgical approach—remained significantly associated with SSI. The c statistic for this model model is 0.70. The Hosmer-Lemeshow goodness-of-fit test indicates no evidence of poor fit (p = 0.98). Compared with patients undergoing resection for malignancy, patients undergoing an operation for diverticulitis had a slightly higher, but not statistically different odds of SSI (odds ratio [OR] 1.3, p = 0.34). Patients with inflammatory bowel disease (IBD) had significantly higher odds of being diagnosed with an SSI (OR 1.59, p = 0.03). Those patients undergoing CRS for indications other than cancer, IBD, or diverticulitis (such as rectal prolapse or constipation) had the lowest odds of SSI (OR 0.49, p = 0.03).
IBD = inflammatory bowel disease; BMI = body mass indes.
The BMI also remained significantly associated with SSI. Patients in the lowest BMI category (<18.5) had the highest odds of SSI (OR 4.09, p = 0.04), compared with those in the reference group (BMI 18.5–24.9). As BMI increased, compared WITH the reference group, the odds of SSI also increased. The odds of SSI in patients with BMI 35+ were more than 2.5 times that of patients with BMI 18.5–24.9 (OR 2.53, p = 0.003)
Incision size and surgical approach were independently associated with the occurrence of SSI. All of the patients undergoing laparoscopic surgery had an incision length of less than 14 cm. In those patients, laparoscopy was associated with significantly decreased odds of SSI (0.63, p = 0.05). Increasing incision size was associated with a continuous increase in SSI, although only the largest incision size was statistically significant. Compared with an incision size of 7 cm, the odds of SSI were 1.41 (p = 0.39), 2.17 (p = 0.07), and 2.50 (p = 0.05) times as great for incisions measuring 7–13.9 cm, 14–20.9 cm, and ≥21 cm, respectively.
The adjusted, predicted probabilities of any SSI based on BMI, incision length, surgical approach, and surgical indication are demonstrated in Figures 2A and 2B.
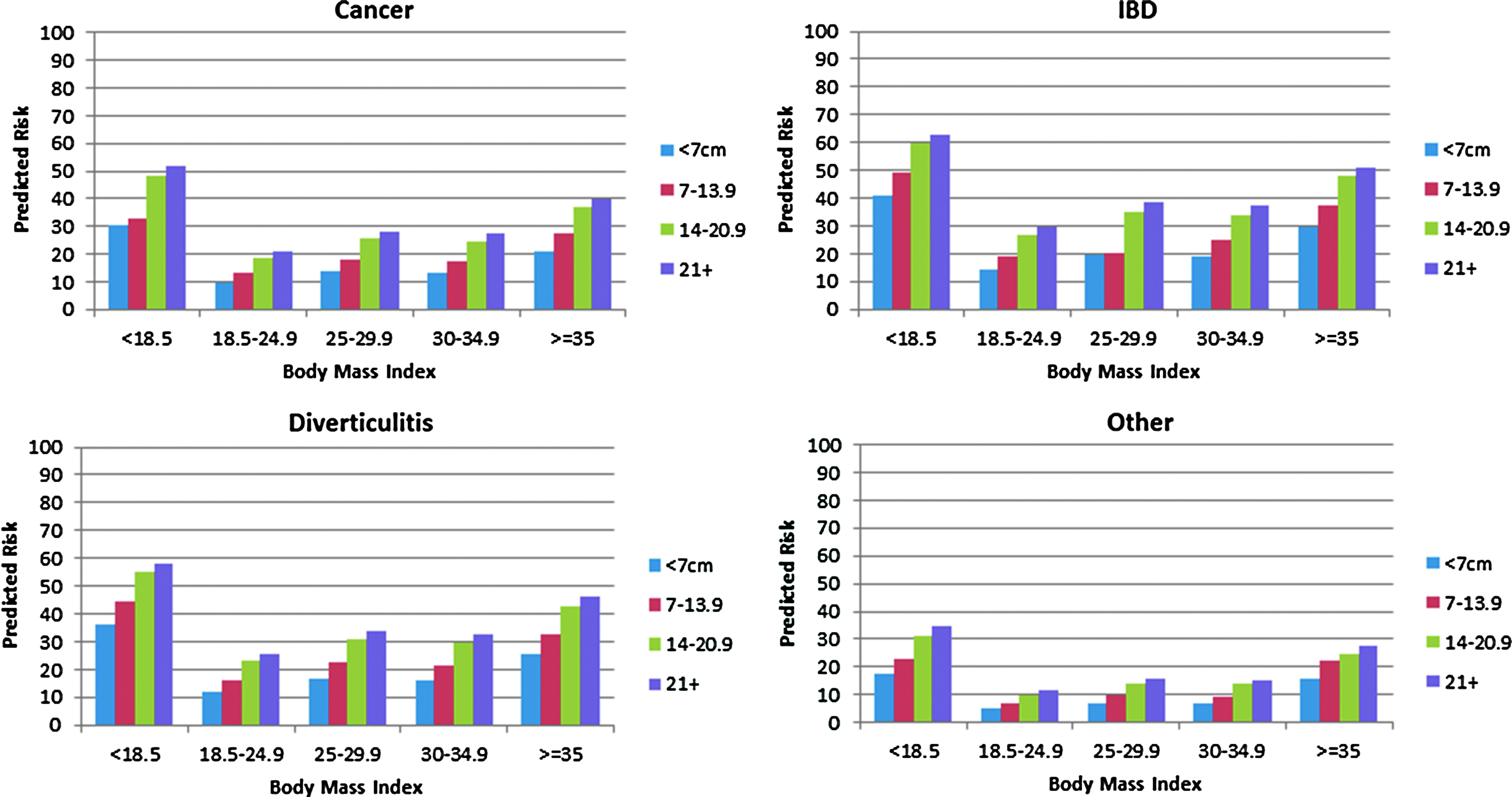
Adjusted predicted risk of surgical site infection after open colorectal surgical procedures. IBD = inflammatory bowel disease.
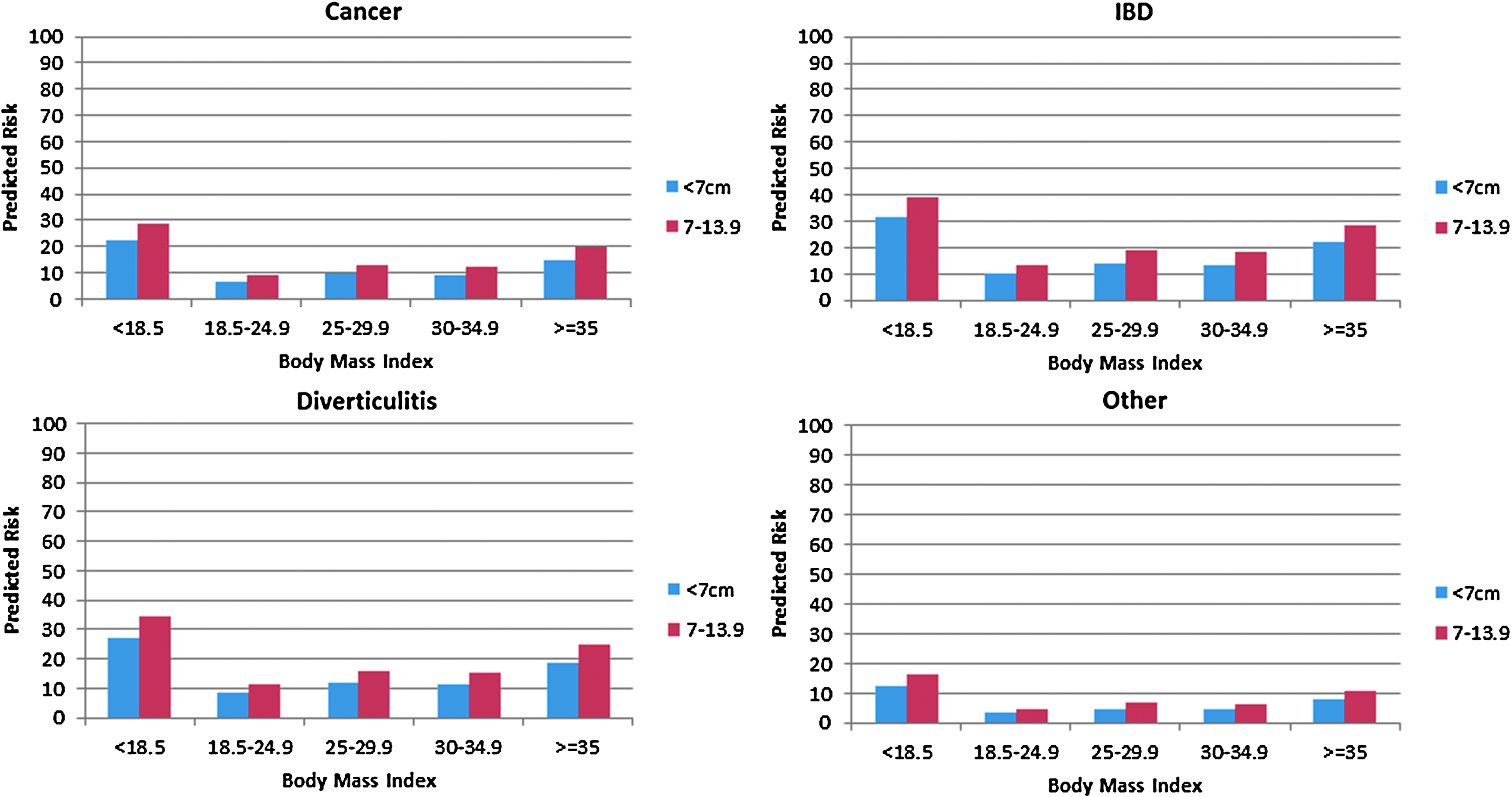
Adjusted predicted risk of surgical site infection after laparoscopic colorectal surgical procedures. IBD = inflammatory bowel disease.
Discussion
Elective colorectal procedures continue to be plagued by the highest rate of SSI in surgery. Parsing out causation to prevent SSI is a primary motive for risk factor analysis with the assumption that this knowledge will help us fashion a reasonable, evidence-based, cost-effective defense. Additional motivation is provided by the fact that increasing scrutiny of the SSI rate by quality organizations, hospital administration, and third party payers may influence how care is delivered, compensated for, and publicly commented on.
Retrospective SSI analysis and analysis of data in large administrative databases provided by organizations such as NSQIP, National Inpatient Sample, and University Health System Consortium have been helpful in driving the conversation and providing insights and clues into factors affecting infection rates. Limited and nonspecific access to patient data, lack of longitudinal assessment, and reliance on derived end points, however, limit the utility of the data and introduce bias that can only be overcome by a prospective approach.
This study represents the largest prospective investigation of surgical skin infection in elective CRS. Rigorous documentation by direct visualization, questionnaire, and serial daily photography over more than 30 days has been very important in tracking and evaluating the development of skin infection, understanding the importance of cellulitis, and in observing and determining the relevance of risk factors that differentially affect patients. It also highlights the fact that, when followed prospectively and for a period of greater than 30 days, infection rates appear high. For example, the Michigan Surgical Quality Collaborative, relying on inpatient data, published a review examining solely colorectal surgical procedures and demonstrated a rate of overall SSI ranging from 3.9%–7.1% [17]. By contrast, in this trial, the rate of superficial and deep SSI was more than 17%. Because the LOS averaged 6.8 days with average time to diagnosis of wound infection of 8.7 days, most incision infections were diagnosed in the clinic. The higher rate of SSI in this study likely represents a higher rate of detection rather than a higher rate of infection.
Risk factors for SSI in this study that remained significant in multivariable analysis included indication, BMI, incision size, and operative approach. Inflammatory bowel disease, in contrast to neoplasia and diverticulitis indications, was a driver of SSI for reasons that are somewhat unclear. Use of biologic immunosuppression, chronic malnutrition, ongoing steroid use, complicated presentations (fistulas, abscesses), and routine use of ostomies may make patients with IBD more susceptible to SSI, however. Further study will need to be done to better define specific differences.
Obesity and morbid obesity have been documented to increase infection rate in most surgical procedures. An association between obesity and SSI is encountered in operations ranging from orthopedic procedures to routine gynecologic operations including caesarian sections [18]. It is also encountered regardless of infectious class—high BMI remains a significant risk factor in those undergoing clean as well as clean-contaminated procedures [19]. This study confirms that high BMI is a significant risk factor for SSI in CRS and, further, indicates that increasing BMI is associated linearly with risk of infection. The study also serves, however, to highlight the risks incurred by the severely underweight as well. A BMI <18.5% was independently associated with higher infection rates. Indeed, the severely underweight undergoing an open operation had the very highest rate of wound infection (63%). Chronic illness, malnutrition, and severity of disease may all play a role in creating a milieu that may promote conditions creating SSI.
Finally, although there is a link between incision length and operative approach, it does appear that these two factors are independent of one another. Like obesity, the rate of SSI is linearly related to the length of the incision with larger incisions sustaining much higher rates of SSI. This, combined with data convincingly supporting a protective effect of laparoscopy, is compelling and may represent the most modifiable of the risk factors reviewed and identified. This effect has been identified in other specialties as well and is not specific to colorectal procedures, although the effect is more dramatic in CRS [20]. Less surface area for infection and use of incision protectors may influence the rate of SSI in smaller incisions and in those undergoing laparoscopy. There may also be an association between reduced severity of disease and smaller incision/laparoscopic approach that may be influential as well, although the elective status of the patients in this cohort and exclusion of contaminated and dirty cases does serve to reduce heterogeneity.
Cellulitis was an end point that was specifically included in the study, although it does not meet the CDC definition of SSI. The rate of cellulitis for the study was 4.2% overall. Because the presence of cellulitis drives the use of antibiotic agents, can result in opening of the wound, and generates patient pain, concern, and anxiety, it was an end point that merited measurement. The rate of cellulitis decreased as the study progressed as did both superficial and deep SSI. Better recognition by investigators of cellulitis versus wound hematoma also improved as the study progressed. Pain and warmth were better indicators of cellulitis than erythema. Lack of drainage and prompt resolution of symptoms with institution of antibiotic agents helped distinguish this condition from hematoma. Although superficial and deep SSI were associated with increased LOS when diagnosed in inpatients, and in some cases were responsible for re-admission, cellulitis did not affect either LOS or re-admission. It did, however, generate additional office visits and costs associated with antibiotic prescriptions.
It is clear from these data that there is a very wide range of predicted SSI rate. For example, patients with BMI 18.5–24.9 undergoing a laparoscopic resection through an incision <7 cm for an indication other than cancer, diverticulitis, or IBD have a predicted SSI risk of 3.3%. On the other end of the spectrum, a morbidly obese patient undergoing an open resection through a large incision for IBD has a predicted risk for SSI of 51.1%. If that same patient is underweight (BMI <18.5), the predicted risk goes up to 63%. Modifying these risk factors and investigating ways to mitigate SSI will require a much better understanding of how these factors interact. Identification of disease process, wound length, and BMI as risk factors may serve to help in selection of surgical approach. Modification of open surgical approaches, when appropriate, with routine use of incision protectors, for example, may be borrowed from laparoscopy. Encouraging the use of minimally invasive approaches to minimize skin infection has merit and should be strongly considered.
Limitations of this study include the fact that it was conducted within the same health system among the same group of surgeons, thereby possibly limiting variation that may occur with a broader sample or in different types of hospitals. Also, the sample size is relatively small compared with many of the retrospective studies relying on administrative databases. This could limit our power to identify factors significantly associated with SSI. We believe that this is offset by our robust prospective data collection, which allowed us to accurately diagnose SSI, as well as collect a wealth of accurate clinical information regarding patients and surgical characteristics.
Conclusions
This is the largest prospective investigation of surgical skin infection in elective CRS. Rigorous analysis with photodocumentation and post-discharge follow-up demonstrates that the SSI rate is higher than reported in most retrospective studies and that the risk of SSI varies widely based on both modifiable and non-modifiable factors. Identification of those at the extreme ends of risk may help us focus on these populations in an effort to both identify and mitigate contributors to infection.
Footnotes
Acknowledgment
This work was supported by 3M, Inc.
Based on a poster presentation at the American Society of Colon and Rectal Surgery Annual Meeting, Los Angeles, CA, April 30–May 4, 2016.
Author Disclosure Statement
Dr. Mahmoud received funding from 3M, Inc. to support a randomized trial of skin antisepsis in CRS. For the remaining authors, no competing financial interests exist.