
Abstract
Abstract
Background:
The purpose of this work was to compare pre-made antibiotic-loaded spacers with two commercially available antibiotic agents and custom-made cements with three antibiotic agents added. We evaluated: (a) the validity of our procedures, (b) the control of the rate of infection in the long term, (c) complications, and (d) quality of life and patient satisfaction.
Methods:
A retrospective cohort study was performed on 112 consecutively treated patients between January 2010 and December 2013; 56 patients were treated with a pre-formed cement spacer (clindamycin + gentamicin), and 56 patients were treated with a spacer loaded with three antibiotic agents (clindamycin + gentamicin + vancomycin). Demographic data were collected: Classification of infection according to criteria of Cierny-Mader; microbiologic results; number of previous operations; and years of disease. Infection control or relapse after at least 18 months of follow-up was evaluated. Complications were recorded. Every patient completed the SF-36 test and Oxford Knee Score.
Results:
With a follow-up of 32.87 months (standard deviation 12.04), at the end of treatment, amputation occurred in three of 112 patients because of recurrence of infection, and one patient died from other causes not related to the infection. The study population presented a rate of recurrence of infection of 2.70%.
Conclusions:
Our results suggest that a two stage re-implant with three antibiotic agents added to the spacer should be considered to avoid rescue procedures, especially in patients with multi-resistant micro-organism infections.
C
In recent decades, great advances have been made in surgical techniques and the adoption of preventive protocols throughout the peri-operative period (operating room with laminar flow, ultraviolet rays, antibiotic prophylaxis, etc.). In Italy, however, there are approximately 28,000 new osteoarticular infections per year [4]. According to data from the Italian arthroplasty record of 2013 in Italy, approximately 160,000 arthroplasty operations were performed in 750 hospitals, with an average annual increase close to 5%. Of these, 63,168 were total knee arthroplasty (TKA), and 3,868 of them were revision operations [5].
The PJI remains a persistent and worrying complication; there are several protocols to address this problem such as suppressive antibiotic therapy, debridement, removal of prosthetic implants, mechanical washing with physiologic solution, positioning of an antibiotic spacer, arthrodesis, and amputation. Currently, the two-stage treatment proposed by Insall et al. [6] is considered the gold standard to manage PJI, keeping limb function and eradicating the infection.
Sometimes, we observe multi-resistant or poly-microbial infections, and we find some difficulty in managing them with pre-formed spacers with two antibiotics loaded. The purpose of this work was to compare the pre-formed spacers with two commercially available antibiotic agents and spacers with a third antibiotic added to the two standard antibiotic agents. We evaluated: (a) the validity of our procedures, (b) the infection rate control in the long term, (c) complications and (d) quality of life and patient satisfaction.
Methods
A. Sample selection
A retrospective cohort study was performed on 112 patients between January 2010 and December 2013. Demographic data were collected, and all patients were divided according to the classification of Cierny-Mader for COM type IV, which considers host A and B: 52 patients were host A without local or systemic impairment; 60 were host B, with a local or systemic impairment present at the time of hospitalization [7].
The inclusion criteria were all patients with TKA and a history of infection greater than three months; the exclusion criteria were patients in host C of the Cierny-Mader classification, who were not suitable for operation because of an unacceptable risk-benefit correlation, and patients with inaccessible clinical data or incomplete medical history. The average age was 56.15 years (standard deviation [SD] 16.89), 79 males, 33 females, with an average time of infection of 36.78 months (SD 63.60) and average surgical procedures before reaching our structure of 2.16 (SD 1.58).
Patients were divided into two groups: Group I: 56 patients (39 M, 17 F) with an average age of 54.36 years (SD 18.09), a body mass index of 26.96 (SD 3.80), underwent an average of 2.25 operations (SD 1.77) and lived with the infection 42.55 months (SD 83.25) before reaching our structure; 27 patients were host A and 29 host B; 38 patients (67.86%) had a monobacterial infection at the time of hospitalization, eight (14.28%) had a multiple infection, and 10 (17.86%) had an unknown micro-organism infection. They were treated with Copal cement (clindamycin 1 g + gentamicin 1 g). The average follow-up time in this group was 32.19 months (SD 13.22).
In Group II, there were 56 patients (40 M, 16 F) with an average age of 57.95 years (SD 15.57), a body mass index of 28.15 (SD 3.94), who underwent an average of 2.07 operations (SD 1.39) and coexisted with the infection about 32.53 months (SD 32.85); 25 patients were host A and 31 host B; 38 patients (67.85%) had a monobacterial infection at the time of hospitalization, seven (12.5%) had a multiple infection, and 11 (19.65%) had an infection by unknown micro-organism. They were treated with Copal +4 g vancomycin. The average follow-up time in this group was 33.53 months (SD 10.80).
B. Surgical technique
First stage
The surgical technique was standardized, and the surgical team was always the same. Using epidural anesthesia, after placing the hemostatic loop, the surgical approach used was the same as the previous operation. In all cases, five samples of bone, soft tissue, joint capsule, and synovial fluid were taken for each patient for microbiologic and histologic analysis. Proceeded by first removing the polyethylene insert, then the femoral component and finally the tibial component. A radical debridement of necrotic and potentially infected soft tissues was performed; the bone canals were carefully cleansed, there was extensive curettage and removal of bone sequestration; protection of healthy bone and abundant irrigation of saline serum with pulsed lavage guns were performed.
To cover the interosseous spaces and to obtain a high concentration of antibiotic agents in the septic zone, an antibiotic-loaded cement spacer (COPAL G+C,® Haereus, Germany) was used. The cement was always mixed manually and modeled on a skeleton of K-wires. We opted for an articulated spacer composed of two parts: A tibial and a femoral component, thus allowing maintenance of a good range of motion (Fig. 1). Each spacer was designed during the operation and customized to the bone morphology of the patient. Once placed, micro-perforations were made in the cement to increase the contact surface of the spacer during the set time. Subsequently, the hemostatic loop was removed, cauterization was performed, drainage (that was maintained for 48 h) was positioned, followed by suture placement and medication.
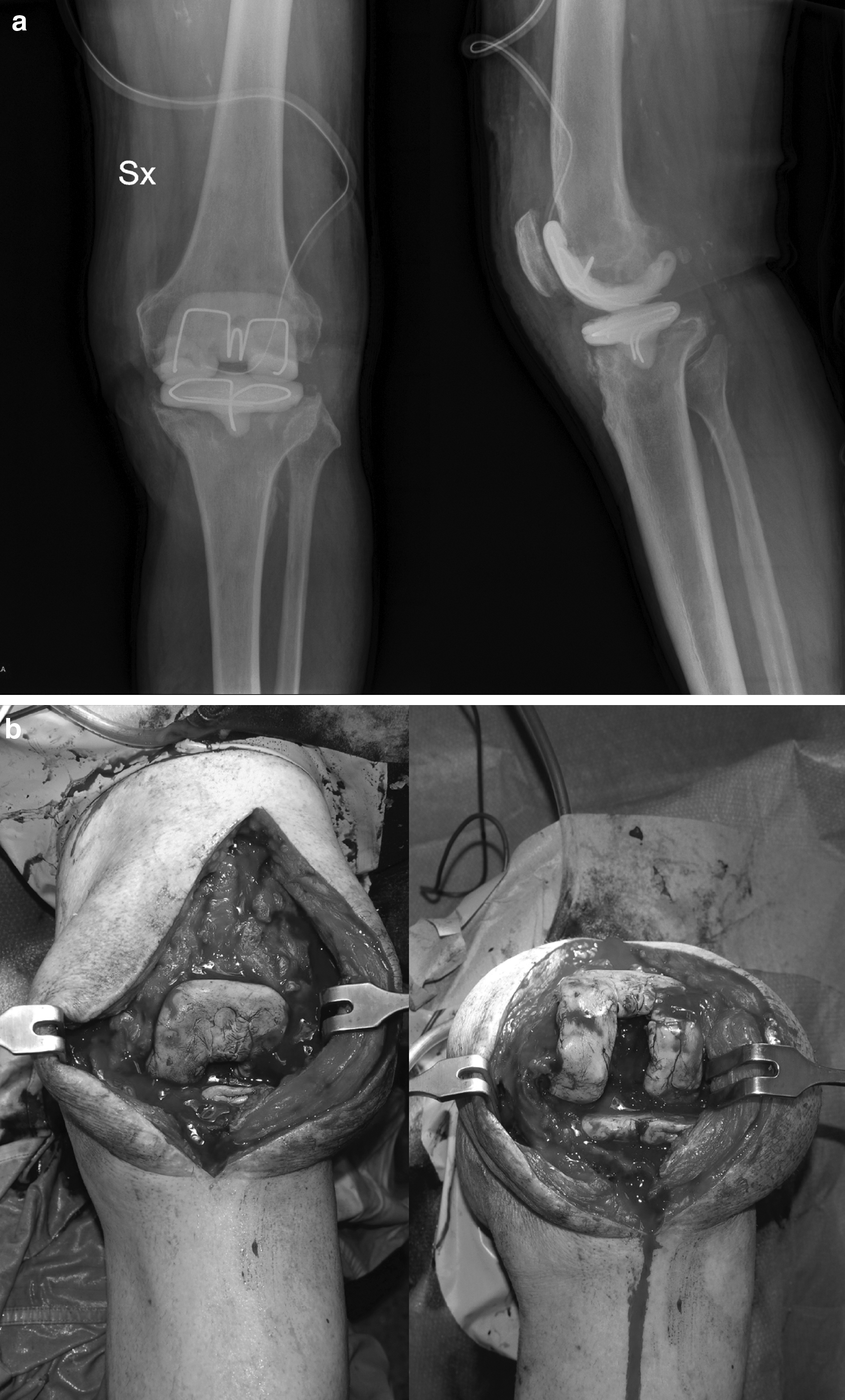
Example of our articulated spacer: (a) antero-posterior and latero-lateral, radiographs; (b) good range of motion.
Time between stages
After the first surgical stage, empiric antibiotic treatment was started. The erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were monitored, and after normalization of the CRP values, antibiotic agents were stopped, and the patient could undergo the second step. The authors considered the patient “free from infection” when, after cessation of antibiotic treatment, there were no clinical signs of infection and the values of ESR and CRP were normalized.
Stage two
The second stage procedure was the same as the first one; the the purpose was to preserve vital tissue as most as possible. Subsequently, a new prosthesis or an arthrodesis was positioned. In some cases, it was necessary to renew the spacer because of bone and soft tissue conditions or recurrence of infection; for this reason, stage two was postponed.
After stage two, antibiotic therapy continued for three weeks, first with intravenous therapy for one week, followed by oral therapy to complete the protocol. In most patients, the antibiotic agents used were vancomycin and rifampicin.
Statistical data
All data were entered into the IBM SPSS Statistical 22 software to check for possible errors and process data. The Kolmogorov-Smirnov test was used to study demographic characteristics; two statistical tests were used to compare the data between the groups: Student t-test for continuous quantitative variables and chi-square for qualitative dichotomous variables. The average ±, SD, and percentages (%) were applied for data description. All statistical tests were two-tailed, and a value of p < 0.05 was considered statistically significant.
Results
The demographic data of the groups under study are summarized in Table 1; the groups under study do not present different statistically significant demographic or baseline characteristics. At the end of treatment and after 32.87 months of follow-up (SD 12.04), in the last follow-up, three patients from the 110 had received amputations after relapse of infection, one patient died from other causes unrelated to infection, and one patient had to leave the study because he could not continue the surgical treatment in our structure because of his co-morbidities. This means that the re-infection rate regardless of the treatment followed was 2.73%.
In group I (n = 56), in the last follow-up, one patient died, and one continued treatment in another structure. Of 54 patients, 52 (96.30%) were free from infection. The average time between the two stages was 9.08 weeks (SD 1.79). Of the 54 patients, 39 underwent total knee re-implantation; one presented recurrence of multi-resistant Staphylococcus aureus (MRSA) infection at follow-up and decided to undergo amputation of the lower limb; 11 underwent arthrodesis. Four patients re-iterated the antibiotic cement spacer because the infection was still active, although silent; one of them was in arthrodesis and three had total knee re-implantation; one of these patients presented a recurrence of S. aureus infection at follow-up and finally underwent amputation. Other procedures that were used were surgical cleanings and mobilization in narcosis. The results are shown in Table 2.
MRSA = multi resistant Staphiloccus aureus; MRSE = Multi Resistant Staphylococcus Epidermidis; SA = Staphylococcus aureus; SE = Staphylocccus epidermidis; P.A. = Pseudomonas aeruginosa; E.F. = Enterococcus faecalis; K.P. = Klebsiella pneumoniae; U. = Unknown
The re-infection rate in group I was 3.70%. Most known infections were caused by S. aureus, and eight patients had an infection caused by multiple micro-organisms. In 10 patients, the micro-organisms were not isolated at any time. The results are shown in Table 3.
Replantation PTK after cement reiteration; **arthrodesis after cement reiteration.
In group II (n = 56), at the last follow-up, 55 of 56 (98.21%) patients were free from infection. The average time between the two stages was 9.25 weeks (SD 1.68); of the 56 patients, 49 underwent re-implantation of a total knee prosthesis; one who presented recurrence of infection with Pseudomonas aeruginosa in the follow-up finally underwent amputation of the lower limb; four underwent arthrodesis; three re-iterated the cement spacer with antibiotic agent because the infection was still active, although silent; all three underwent re-implantation of the total knee prosthesis. Other procedures used followed the same treatment plan as Group I. The results are shown in Table III.
The rate of re-infection in group II was 1.79%. Most known infections were caused by S. aureus: seven patients were infected by multiple micro-organisms; in 11 patients, the micro-organism was not isolated at any time.
The host type (A or B) did not influence the risk of relapse of infection. In fact, in Group II, the patient with relapse was Host B; in Group I, one patient was Host A and another Host B; we found small differences, but without statistical relevance.
Discussion
Osteomyelitis is one of the most devastating diseases found during the treatment of patients with bone diseases. The incidence of infection in TKA is approximately 2%, increasing to 10%–15% when we talk about revision surgery [8,9]. There are several methods to approach this pathology: Treatment with irrigation; debridement and change of polyethylene [10] with rates of infection control approximately 30%–80% according to the studies; one-stage revision with control rate of infection elevated 75%–85% [11]. Two-stage revision is, however, considered the gold standard with an infection control rates between 75% and 95% [8–10].
The two stages treatment allows us, in the first surgical time, to be more radical and meticulous in the debridement, by removal of necrotic and infected areas from bone and soft tissues. It is important to perform the exportation of all the prosthetic material.
During the second surgical time, after removal of the spacer, a less aggressive debridement and a new surgical cleaning were performed as we worked on tissue initially not infected, although in seven patients (Table 2), we had to repeat the spacer because of the lack of guarantees to eradicate the infection; in three patients, during the second surgical time, we observed that the infected tissue was not completely eradicated—two belonged to Group II and one to Group I. It is very important, in this second stage, to evaluate the articulation during surgery to decide whether, once phlogosis indexes are normalized to consider re-implantation of a TKA or re-iteration of the spacer. In these cases, surgeon experience is relevant in the management of this pathology. Published studies demonstrate the success of eradication of infection after two-stage surgical treatment [12,13], even though the rates of recurrence of infection remain high and those are largely correlated with surgical cleaning and elimination of necrotic areas. There are some studies for [14] and against [15] the re-iteration of the spacer, always maintaining systemic antibiotic therapy.
In our study, when the surgeon suspected a recurrence of infection, the second phase was postponed and the cement spacer was repeated, either because of the ESR and CRP values or because of the local conditions found once the surgical approach was performed.
ESR and CRP are commonly used as markers to diagnose and monitor the COM. In our cohort, however, the efficacy of these markers as prognostic factors was not demonstrated; the ESR and CRP values were not useful in predicting the risk of re-infection after the second phase. This correlates with a previous study that minimizes the role of these markers in total knee revision [16]. To support the surgeon in choosing the right time to re-implant the TKA, more accurate diagnostic tests are required, with greater sensitivity and specificity. New tests capable of detecting infection through the levels of α-defensin and neutrophils in the joint fluid are promising [17].
Our institute is a high-level center in the treatment of patients with infections, and the vast majority of patients had been treated for infection previously in other hospitals in our cohort. Previous operations or long periods of infection have not been factors determining the rate of recurrence of infection (Table 2), and were excluded as confounding factors, as well as the type of antibiotic treatment received after operation.
In our study, 3.70% of patients treated with a cement spacer with two antibiotic agents and 1.79% of patients treated with a cement spacer with three antibiotic agents had recurrence of infection. These percentages are lower than those reported in scientific literature that present an incidence of 10%–25% recurrence after treatment in two stages [8–10]; however, they do not present statistically significant differences with a p value of 0.537.
In the first stage, the surgeon opted for a pre-formed cement spacer with two or three antibiotic agents. Gentamicin and vancomycin have a synergistic effect [9,10,18], as is demonstrated in various scientific studies. For clindamycin, there are two in vitro studies that show antagonism because of a reduction in the time kill curve [11,19]. An in vivo study, however, demonstrated clinical improvement in patients with MRSA bacteremia who were treated with vancomycin in association with clindamycin [20]. The choice of vancomycin as the third antibiotic agent is because of its ability to inhibit the formation of biofilm and its ability to penetrate and maintain bactericidal activity (21,22) also in biofilm. In vitro studies, such as that of Gasparini et al. [23] showed that there is also an increase of elution from the cement of tobramycin between aminoglycosides, but at concentrations comparable if not inferior to those of vancomycin.
Among the tested antibiotic agents, they also noted a reduced release of rifampicin. This is another reason that led us to choose vancomycin as the third antibiotic agent. The antibiotic spacer, in addition to assisting in the eradication of infection by ensuring the release of local antibiotic agents, maintains limb length to avoid severe dysmetria, provides adequate stability, and facilitates the second stage of TKA re-plantation.
In the second step, the surgeon reiterated the cement spacer in 11 patients—five patients in group I and six in group II—with no statistically significant differences. Previous studies suggest that there is a greater failure rate in the COM treatment caused by MRSA [24–26]. In this study, we found one patient with MRSA in group I who relapsed with the same micro-organism at follow-up; three patients with MRSA and one with multi-resistant Staphylococcus epidermidis in group II were free of infection at the last follow-up. The “Proceedings of the International Consensus Meeting on Periprosthetic Joint Infection” recommends with a strong consensus (86%) that patients with MRSA should be given pre-operative antibiotic prophylaxis with vancomycin or teicoplanin. We observed that all the patients who underwent treatment with the cement spacer of three antibiotic agents were free of infection. In terms of results of the Oxford Knee Score and SF 36 score, we observed that in Group I, a higher score was achieved, but without statistically significant differences (Table I).
Our results, therefore, demonstrate that a two-stage treatment with spacers with two or three antibiotics has a high success rate in the management of chronic osteomyelitis. We observe that the patients of group II, compared with those of group I, present an almost 2% lower rate of relapse, but with a p value of 0.537, so we can affirm that there are no statistically significant differences.
We observed that after the first stage, a great number of patients in group II were in optimal condition to continue with a re-implantation surgical procedure, finding a statistically significant difference with a p value of 0.045. Another statistically significant difference with a p value 0.043 was that the most patients who ended up with arthrodesis after the first stage were in group I, either because of the quality of the bone or because of the patient's limited chances of being free of infection. Regarding the need to reiterate the spacer or perform other procedures because of complications, we did not find statistically significant differences.
Previous attempts to manage the infection did not affect the results negatively. Our results suggest that a two-step re-implantation with three antibiotic agents should be considered in these patients to avoid rescue procedures, especially in patients with multi-resistant micro-organism infection.
We find some limitations in this study. The non-randomized retrospective design may cause errors when data are not correctly reported in medical records, although in these cases, patients were excluded from the study. We believe that our study offers important information about the cement spacer with three antibiotic agents. After a search in the scientific literature, we have verified that there is no study using the two-stage surgical procedure that compares the results of the spacers with two or three antibiotic agents. We believe, however, that it is important to perform controlled randomized studies in the future, with a larger study group to observe statistically significant differences.
Footnotes
Author Disclosure Statement
No competing financial interests exist.