
Abstract
Abstract
Background:
Cells of tissues and biofilm forming bacteria compete for the living space on the surface of an implant. We hypothesized the incubation of the implant (titanium, polydimethylsiloxane, and polystyrene surface) with human cells before implantation as a strategy to prevent bacterial adhesion and biofilm formation.
Methods:
After 24 hours of incubation with human osteogenic sarcoma SaOS-2 cells (1 × 105 cells/mL), the materials were incubated for 4.5 hours or two days with Staphylococcus aureus in serial 1:10 dilutions of 108 colony-forming units/mL. The bacterial adherence and biofilm biomass on materials pre-incubated with SaOS-2 cells were compared with our previous results on materials incubated only with bacteria or in simultaneous co-culture of SaOS-2 cells and S. aureus. Fluorescent microscopy and crystal violet stain were used. The number of viable SaOS-2 and bacterial cells present was tested using colorimetric methods (MTT, LDH) and drop plate method, respectively.
Results:
The pre-treatment with human cells was associated with a reduction of bacterial colonization of the biomaterial at 4.5 hours and 48 hours compared with the non-pre-treated materials. The presence of bacteria decreased the number of viable human cells on all materials. (Supplementary Fig. 1; see online supplementary materials at www.liebertpub.com/sur).
Conclusions:
These results suggest that the pre-operative incubation of prostheses with host cells could prevent infection of biomaterials.
T
Research on anti-biofilm implant properties focuses on materials loaded or coated with anti-adhesive/anti-bacterial substances or surfaces with nanostructures [8–13]. Active coatings release pre-incorporated bactericidal agents such as antibiotic agents, antiseptics such as silver ions or growth factors, chemokines, and peptides that prevent the infection. The spread of some of these substances into the neighboring tissues, however, could provide a consequent risk of inducing bacterial resistance or cytotoxicity [14]. The most recent approaches, so-called passive coatings, appear promising, because they diminish the rate of infections by enhancing tissue compatibility or integration, or by directly inhibiting bacterial adhesion [15–17].
Adherence and colonization by either bacterial cells or tissue cells on biomaterials have been studied mainly as separate phenomena [1,8,9,18]. During the development of new biomaterial coating strategies, however, these two issues must be evaluated in parallel, because it is essential to achieve a successful long-term outcome. According to our previous study, in the race between bacteria and tissue cells for the implant surface, the presence of either one reduces biomaterial adhesion and the viability of the other, which implies that host-cell integration on implant surfaces reduces bacterial contamination [19].
Micro-organisms frequently infect an implant surface during surgical procedures and start to compete for the surface before tissue integration [20]. We hypothesized that incubation of implants with host cells before implantation may be a way to reduce the living space available for the bacteria and would thus help to avoid the bacterial adhesion and consequently the infection of biomaterials, eluding the use of antibiotic-loaded biomaterials, which confers a risk for bacterial antibiotic resistance [21,22].
Methods
Materials
Magnetron sputtering technique was used for deposition of titanium samples as described previously [9]. The 2-mm thick bulk polydimethylsiloxane (PDMS) polymer sheets of size 9 × 9 mm were obtained from a commercial supplier of industrial polymers (ETRA, Helsinki, Finland). Average surface roughness Ra was approximately 300–400 nm for both materials. The 24-well cell culture plates of polystyrene (PS) (Thermo Scientific Nunc, Roskilde, Denmark) were used as control material.
Co-culture of human cells and staphylococci
Culture of human cells
Human osteosarcoma SaOS-2 cells (ECACC, Salisbury, Wiltshire, UK) were grown as described by Perez-Tanoira et al. [19]. Human cells were seeded at 105 cells/mL on (a) titanium, (b) PDMS, and (c) directly on 24-well PS cell culture plates and were incubated in a total volume of 2 mL of MEM (minimal essential medium) supplemented with 10% heat-inactivated fetal bovine serum (FBS) and 1%
Culture of staphylococci
Staphylococcal adhesion experiments were performed as described by Kinnari et al. [12]. The S. aureus 15981 [23] isolated at the Microbiology Department of the University Clinics of Navarra, Spain, was selected because it has a strong biofilm production phenotype and a well-described antibiotic susceptibility profile. Bacteria were diluted in sterile 10 mM phosphate-buffer saline (PBS) to obtain suspension with a 108 colony-forming unit (CFU)/mL. The optical density of the bacterial suspension was measured at a wavelength of 550 nm with a spectrophotometer according to the McFarland standard (BioMerieux, SA Lyon, France).
Co-culture of human cells and staphylococci
Serial 1:10 dilutions were made from 108 CFU/mL S. aureus suspension to obtain the bacterial concentrations of 107, 106, 105, 104, 103, and 102 CFU/mL in a total volume of 2 mL of MEM:PBS (1:1), MEM including 5% FBS, 0.5%
A negative control (1 mL of PBS +1 mL of MEM), bacterial control (1 mL of 108 CFU/mL of S. aureus on PBS +1 mL of MEM), a cellular control (1 mL of 105cells/mL on MEM +1 mL of PBS after 4.5 hours, [24 + 4.5] hours, 48 hours, or (24 + 48) hours) were also included. In each experiment, a total of 10 samples of titanium, PDMS, and well plates were covered with each of the different dilutions, and incubated first for 4.5 hours at 37°C to allow cell and bacterial adhesion and then up to 48 hours for biofilm formation and cell adhesion in a static model.
Assessment of cell proliferation and cytotoxicity
Fluorescence microscopy
After incubation with the different dilutions of bacteria and human cells, samples were washed three times with PBS. The dried plates were stained for two minutes with a rapid fluorescence staining method using Acridine Orange (BD Diagnostics, Sparks, MD). Images were taken with a fluorescent light Leica DM6000 B/M research microscope (Leica Microsystems, Wetzlar, Germany) equipped with Leica DFC420 digital camera (Leica Microsystems), with 10 × magnification and identical settings and parameters for photographing of all samples. On each plate, eight fields were viewed and photographed. All experiments were performed in triplicate.
Assay for SaOS-2cell viability
Human cell viability was assessed by 3-(4,5-dimethylthiazolyl-2)-2,5-diphenyltetrazolium bromide tetrazolium (MTT) dye assay based on mitochondrial ability to transform soluble MTT to its insoluble purple product, formazan. After 4.5 hours or 48 hours, culture medium was replaced by 10 mcL of 5 mg/mL MTT (EMD Millipore Corp., Billerica, MA) dissolved in dimethyl sulfoxide (DMSO) (MP Biomedicals, LLC, Illkirch, France) for four hours. Then, cells were suspended by adding 300 mcL of detergent reagent at +22°C during two hours. Aliquots of 200 mcL were then transferred to 96-well plates for measurement of absorbance using CHAMELEON V Multilabel Microplate Reader (Hidex, Turku, Finland) with 570 nm test and 690 nm reference wavelengths.
Lactate dehydrogenase (LDH) cytotoxicity assay
Cytotoxicity was determined by assessing the release of cytosolic enzyme LDH into the supernatant medium. The LDH assay was performed using tetrazolium dye-based CytoTox 96 Non-Radioactive Cytotoxicity Assay (Promega, Madison, WI) according to the manufacturer's instructions. Supernatants (experimental LDH release), samples treated with the lysis solution (maximal LDH release), and non-treated control samples (spontaneous LDH release) were transferred to 96-well plates. The absorbance at 490 nm was read using a microplate reader. Percentage of cytotoxicity values was calculated using the formula (100 × [experimental LDH release – spontaneous LDH release/maximum LDH release-spontaneous release]) [24].
Bacterial adherence and biofilm formation
Bacterial adherence and biofilm formation results obtained in this study from materials pre-incubated with SaOS-2 cells during 24 hours were compared with results of our earlier study obtained from materials incubated with S. aureus only or in a co-culture with SaOS-2 cells [19]. After 4.5 hours and 48 hours incubation time, samples were washed three times with 250 mcL of PBS to remove non-adherent bacteria and cells, followed by treatment with 400 mcL of trypsin. To compare the results, all the materials, incubated or not with SaOS-2 cells, were treated with trypsin to take into consideration the possible effect of trypsin. Controls were performed simultaneously with the tests to avoid bacterial adaptation to laboratory conditions.
Drop plate method
All materials were sonicated in an ultrasonic bath USC100T (VWR, Leuven, Belgium) at 45 kHz with a power output of 300W for five minutes in 2.5 mL of PBS as described earlier [25,26]. The number of viable bacteria in each sonication product was quantified by the drop plate method [27]. The bacterial count obtained from co-cultures was compared with the results of bacterial monocultures. The experiments were all performed in sets of three.
Crystal violet
Based on the methods of Pitts et al. [28] and Stepanovic et al. [29], at the end of the incubation period, each material was washed to remove all non-adherent bacteria. The remaining attached bacteria were stained for 15 minutes with 1% crystal violet stain. Excess stain was rinsed off by placing the plate under running tap water. The dye bound to the adherent cells was re-dissolved in 300 mcL of 95% ethanol. Aliquots of 200 mcL were then transferred to 96-well plates for measurement of absorbance using Chameleon-V microplate reader with 570 nm (test) and 690 nm (reference) wavelengths.
Statistical analysis
The statistical analyses were performed with four independent experiments per test condition. The data are reported as (mean ± standard deviation [SD]). Data were analyzed using IBM SPSS Statistics for Windows Version 22.0 software (IBM Corp., Armonk, NY). Non-parametric tests were used. Mann-Whitney or Wilcoxon tests were used for two samples, and the Kruskal-Wallis test was used for more than two samples.
Results
Effects of bacterial exposure on number of viable cells and on cytotoxicity
Figure 1 shows representative images of the titanium surfaces incubated with human cells for 4.5 hours or 48 hours in the presence or absence of bacteria. When SaOS-2 cells were pre-incubated with the biomaterial for 24 hours before addition of bacteria, the number of attached S. aureus on biomaterials was clearly lower than with the same bacterial density without cells (panels a and f), or when cells and bacteria were added simultaneously (b and g). The data of panels (a, b, c, f, g, and h) are presented for comparison and are obtained from our previous study [19]. When bacteria were added, the number of viable SaOS-2 cells on biomaterial was significantly reduced both in simultaneous co-culture (panels b and g) and materials pre-incubated with SaOS-2 cells (panels d and i), as compared with SaOS cells incubated alone, both after 4.5 and 48 hours of culture (panels c, e, h, and j).

Representative fluorescence microscope images of titanium surface incubated with 108 colony-forming units (CFU)/mL of Staphylococcus aureus (a), simultaneous co-culture of 105 SaOS-2 cells/mL and S. aureus (b), or 105 SaOS-2 cells/mL (c) for 4.5 hours or for 48 hours (f–h). Panels d,e and i,j had similar conditions except that SaOS-2 cells had been pre-incubated for 24 hours before adding S. aureus. Incubation times in d,e were 4.5 hours and in i,j, they were 48 hours. The samples were stained with Acridine Orange (BD Diagnostics, Sparks, MD).
The results were confirmed for all bacterial densities by using MTT proliferation assay. The reduction was not affected by the bacterial density for PS (p = 0.685 and p = 0.100, Kruskal-Wallis test, for 4.5 hours and 48 hours, respectively) or PDMS (p = 0.158 and 0.246 for 4.5 hours and 48 hours, respectively). This was visible on the titanium surface, however, where CFU/mL >106 diminished number of viable SaOS-2 cells compared with CFU = 102. There were no statistically significant differences on number of attached human cells on titanium surfaces for CFU = 103-108 (p = 0.187 and 0.550 for 4.5 hours and 48 hours, respectively).
Figure 2 shows a statistically significant reduction of the percentage of viable SaOS-2 cells after 48 hours compared with 4.5 hours for all bacterial densities and materials with respect to the materials incubated only with SaOS-2 cells.

Percentage of viable SaOS-2 cells pre-incubated for 24 hours (measured by MTT assay) on polystyrene, titanium, and polydimethylsiloxane in the presence or absence of different concentrations of Staphylococcus aureus after incubation of 4.5 hours and 48 hours. Results are means ± standard deviation of four determinations in quadruplicate culture. *Statistically significant means p < 0.05 for 4.5 hours compared with 48 hours unless otherwise mentioned. CFU = colony-forming units.
Bacteria were cytotoxic to the pre-incubated SaOS-2 cells as evidenced by increased LDH release from cells on all materials studied (Fig. 3). Cytotoxicity was not dependent of the bacterial density for PS (p = 0.494 and p = 0.275 for 4.5 hours and 48 hours, respectively) and PDMS (p = 0.361 and p = 0.457 for 4.5 hours and 48 hours, respectively). Only in the case of cells incubated on titanium for 4.5 hours, the presence of S. aureus CFU/mL ≥106 increased the death of SaOS-2 cells (p = 0.388 for CFU/mL = 102-105 after 4.5 hours and p = 0.382 for CFU/mL = 102-108 after 48 hours). On the other hand, the percentage of cell cytotoxicity after 48 hours was higher compared with the same bacterial density and materials after 4.5 hours, only with the exception of titanium for CFU ≥107 (p = 0.248 for CFU/mL = 107-108).
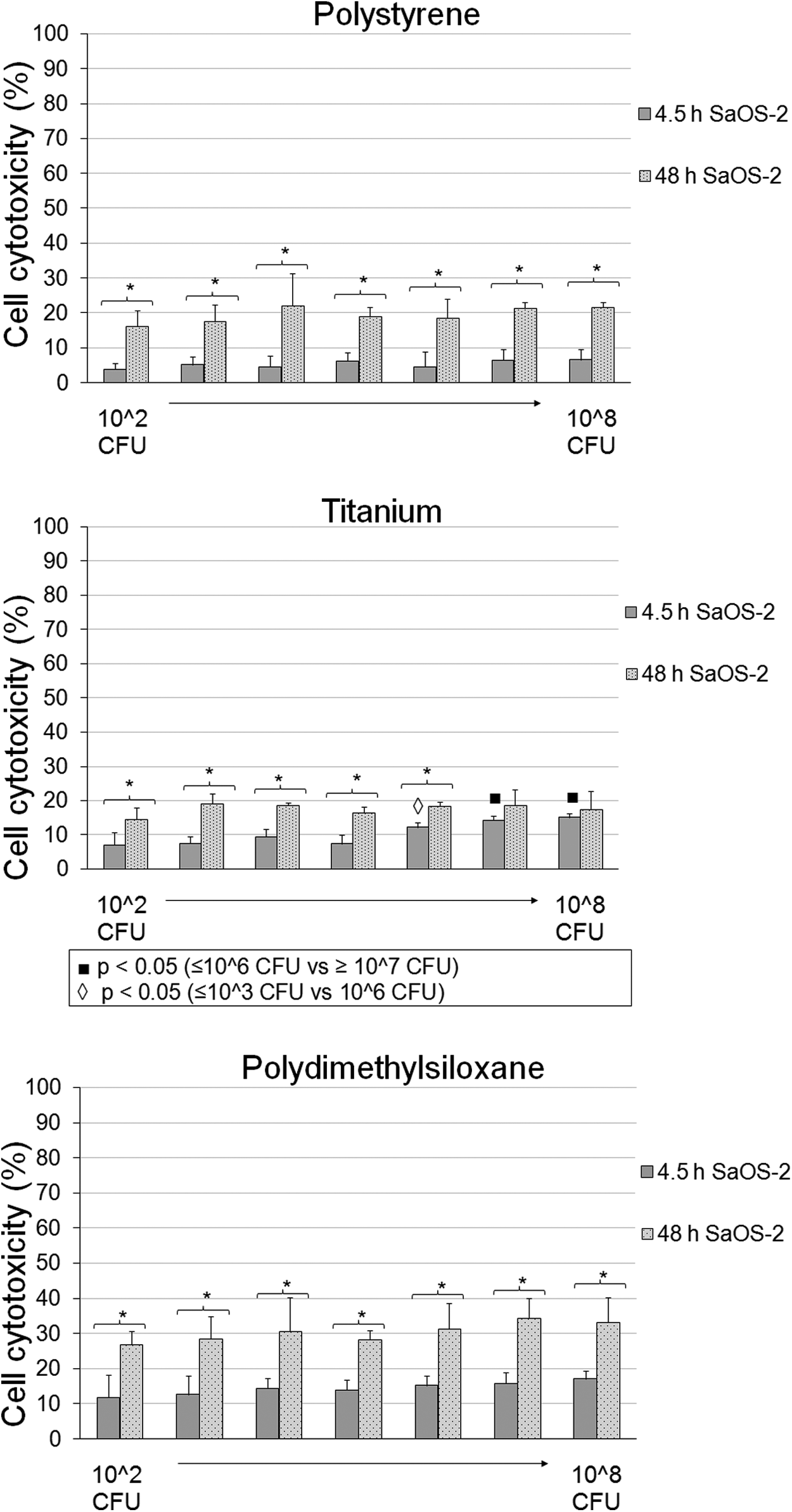
Lactate dehydrogenase activity levels of media of SaOS-2 pre-incubated for 24 hours on polystyrene, titanium, and polydimethylsiloxane in the presence or absence of different concentrations of Staphylococcus aureus after 4.5 hours or 48 hours. Results are means ± standard deviation of four determinations in quadruplicate culture. *Statistically significant means p < 0.05 for 4.5 hours compared with 48 hours unless otherwise mentioned. CFU = colony-forming units.
Incubation of biomaterial with human SaOS-2 cells reduces the viability of bacterial cells and the biofilm formation
The pre-incubation of prosthetic materials with SaOS-2 cells reduced bacterial adherence and biofilm biomass compared with the materials incubated only with bacteria or with simultaneous co-culture with S. aureus and SaOS-2 cells as detected by crystal violet. This was observed with all bacterial concentrations with the exception of simultaneous co-culture at 4.5 hours, on PS with CFU/mL ≥107 (p = 0.080 and 0.561 with CFU/mL = 107 and 108, respectively), and titanium with CFU/mL = 108 (p = 0.081) and at 48 hours on PS with CFU/mL = 108 (p = 0.149) (Fig. 4).

Absorbance value of crystal violet assay after 4.5 hours and 48 hours incubation. Mean and standard deviation are shown. *Statistically significant means p < 0.05 versus all other situations unless otherwise mentioned. CFU = colony-forming units.
As demonstrated in Figure 5, the amount of viable bacteria in all materials and with different concentrations of bacteria was reduced by the pre-incubation with SaOS-2 as compared with the materials incubated only with S. aureus or in simultaneous co-culture (Fig. 5).

Colony-forming units as determined by viable cell count after 4.5 hours and 48 hours incubation. Mean and standard deviation are shown. *Statistically significant means p < 0.05 versus all other conditions unless otherwise mentioned. CFU = colony-forming units.
Discussion
The present findings support the hypothesis that pre-operative incubation of biomaterial with osteoblast host cells could prevent infection of the biomaterial. We found that in vitro, after tissue cells have adhered to the surface of the biomaterial, bacteria cells are more unlikely to displace them. This seems to prevent the colonization of the implant surface with circulating planktonic bacteria that can lead to biofilm development. Otherwise, within the high dense bacterial population, efficient horizontal transfer of resistance and virulence genes takes place leading to the spread of resistance to conventional antibiotic therapies necessitating the use of alternative agents [30,31].
Much of the recent research work in this field has focused on the design of coatings that prevent infection while ignoring bone mineralization or vice versa [1]. The promotion of tissue integration as a mean of protection against infection has been poorly studied [32,33]. According to Subbiahdoss et al. [33], if an implant is integrated rapidly by the tissue to levels above critical cell surface coverage, it will be protected effectively against post-operative contaminating bacteria. Dexter et al. [32], who considered separately the presence of human cells and bacteria, suggested that by controlling the density of proteins or ligands on a surface, cell adhesion and surface coverage could be stimulated without stimulating bacterial adhesion, hence reducing the likelihood of infection.
Our results are in good agreement with the important implication of these findings. Because micro-organisms are frequently introduced on an implant surface during surgery, however, they start the race for the surface with an advantage. We decided to try to prevent the peri-operative contamination by adhering the human cells to the surface before contamination [34].
We need to develop strategies in which bacterial adhesion on biomaterial is avoided; less than102 CFU of S. aureus is needed to develop biofilm in an implant and establish a prosthesis infection [35,36]. Several studies have shown a reduction of bacterial adherence at high bacterial densities, CFU/mL ≥106; however, the clinical relevance of such high bacterial densities may be questionable. We found that at longer incubation times, the presence of bacteria produces a higher decrease of osseointegration. We tested serial 1:10 dilutions from 102 CFU/mL up to 108 CFU/mL. Our results show a biomaterial-associated infection prevention by pre-operative incubation with human cells when materials are contaminated with bacterial density related to clinical circumstances (102-104 CFU/mL).
Starting from the lowest bacterial density, the presence of S. aureus diminished osteoblast viability and proliferation, even when bacteria were not detected or isolated from the surface of the implant. The fact that it was not dependent of the bacterial density, however, is in agreement with our previous study [19], while it contrasts with that of Subbiahdoss et al. [33], who found that once cell surface coverage exceeded a critical value, contaminating bacteria ceased to negatively affect cell growth.
These results are not conclusive, but we think this study can be used as a proof of concept. One question, still unanswered, is how the pre-operative incubation with autologous osteoblast cells affects the tissue integration of the implant. In the future, we will assess the use of primary osteoblast cells. Compared with SaOS-2 cells, longer pre-incubation time will be required with primary cells to obtain coverage of most of the surface area of the implant. Future research will involve the effects of phagocytosis, considering the presence of macrophages in co-culture with bacteria and osteoblasts. These findings could also be proved using clinically significant bacterial strains isolated from prosthetic infections, which may show more virulence against human cells.
Implant infection is a rising problem especially in devices implanted to bone contact such as in orthopedic, maxillofacial, and ear surgical procedures. The implantation to bone contact is increasing and involves patients of all ages. We tested materials mainly used in bone contact, despite the fact that the rate of infection is lower compared with implants used elsewhere [1]. In the next stages of our research, it would be interesting to investigate whether biomaterials such as polytetrafluoroethylene that are used more for soft tissue implantation would show similar prevention of infection when pre-operatively incubated with cells from soft tissue such as fibroblasts.
Conclusions
The concept of tissue integration over microbial colonization provides an important guideline for which “in vitro” assays may be indispensable tools and should be part of the development process of any tissue engineered constructs and devices [37]. It can be argued that the prevention of bacterial adhesion without drugs, through pre-operative incubation of prostheses with host cells, may be one of the most effective ways to reduce biomaterial infections.
Footnotes
Acknowledgments
This work was supported by the Department of Otorhinolaryngology – Head and Neck Surgery of Helsinki University Hospital and University of Helsinki.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.