
Abstract
Abstract
Background:
The long-term significance of early and prolonged antibiotic use in critically ill patients is yet to be described. Several studies suggest that antimicrobial exposure may have as yet unrecognized long-term effects on clinically meaningful outcomes. Our group previously conducted a quasi-experimental, before and after observational cohort study of hemodynamically stable surgical patients suspected of having an intensive care unit-acquired infection. This study demonstrated that aggressive initiation of antimicrobial therapy was associated with increased 30-day deaths. In a follow-up survival analysis, we hypothesized that aggressive antimicrobial treatment would not be a significant predictor of long-term death.
Methods:
Survival data for the 201 patients included in the initial study were obtained from our clinical data repository. Univariable analysis, Kaplan-Meier, and Cox proportional hazards models were used. Survival was evaluated at one and four years. Age, gender, Acute Physiology and Chronic Health Evaluation (APACHE) II score, and co-morbidities were chosen a priori for potential inclusion in the model. Variables that met the model assumptions after testing were included in the final model.
Results:
Follow-up data were available for 190 patients (95 in each group) representing 94.5% of the initial cohort. Twenty-four (25.3%) patients in the aggressive group had initial APACHE II scores of less than 15 compared with 13 (13.7%) patients in the conservative group (p = 0.04). There was a trend toward higher deaths in the aggressive group at four years (41.1% vs. 30.5%; p = 0.13). Kaplan-Meier analysis demonstrated a difference in survival at one year but not at four years. The Cox proportional hazards model showed a higher long-term death for patients in the aggressive antimicrobial group at both one and four years (hazard rate: 2.26 and 1.70, respectively).
Conclusion:
Aggressive initiation of antimicrobial therapy is independently associated with decreased long-term survival after critical illness. While further work is needed to confirm these findings, waiting for evidence of infection before initiation of antibiotic agents may be beneficial.
A
Recent data have suggested that variations in antimicrobial exposure may have some influence on long-term outcomes [4–6]. In addition, exposure may impact outcomes for infectious episodes not usually considered temporally related to the initial exposure [7–10]. We therefore proposed a follow-up survival analysis of our initial cohort study to see whether the differences in deaths that we observed originally persisted beyond the initial study period. We hypothesized that aggressive antimicrobial exposure would not have a significant impact on long-term survival.
Methods
Over a 24-month period between September 1, 2008 and August 31, 2010, critical care surgical patients in the University of Virginia Surgical Intensive Care Unit (SICU) who were suspected of having an ICU-acquired infection were treated according to two different antimicrobial initiation protocols. The aggressive protocol was used from September 1, 2008 to August 31, 2009, and required early aggressive initiation of antimicrobial therapy for patients suspected of having an infection, once an appropriate specimen for culture was obtained but without waiting for the results. The conservative protocol was used from September 1, 2009 to August 31, 2010 and required that antimicrobial therapy be withheld until objective evidence of infection was obtained [3].
Objective evidence of infection was defined as greater than 100,000 colony-forming units (CFU) of bacteria on a quantitative endotracheal suction specimen for pulmonary infection, while the growth of any pathogen greater than 100,000 CFU per mL of urine was considered sufficient for urinary tract infections. Intra-abdominal infections required the presence of any pathogen on Gram stain from any sterilely obtained aspirate for confirmation. Similarly, the recovery of any pathogen on Gram stain from a normally sterile body cavity was diagnostic of infection [3].
We evaluated the same demographic, co-morbidity, and infection data as presented in the original analysis. Age and Acute Physiology and Chronic Health Evaluation (APACHE) II score were categorized to better fit our Cox proportional hazards analysis. In the original analysis, the appropriateness of initial empiric therapy was evaluated on a per infection basis. For this analysis, we recorded the proportion of patients who had appropriate initial antimicrobial therapy in at least two-thirds of their infectious episodes. Otherwise, there were no other variable changes. Vancomycin and piperacillin-tazobactam were the empiric agents of choice during the study period. Empiric antimicrobial rotation was not employed. Classes of antibiotic agents used during the study period were recorded on a per patient basis.
The primary outcome of this study was long-term survival. We analyzed all patients included in the original study for which follow-up data were available. Survival was determined by last known survival date via the Clinical Data Repository (CDR). The CDR is updated with survival data from the Virginia Vital Statistics Registry on a biennial basis, and at the time of this study was up-to-date through December 31, 2014. We evaluated long-term deaths at two separate time points—one year and four years based on the maximum survival follow-up time available for both groups.
Standard univariable analysis techniques were used to evaluate all demographics, co-morbidities, and raw outcomes. Wilcoxon rank sum, chi-square, and Fisher exact test were used where appropriate. Raw survival estimates were obtained using Kaplan-Meier analysis. Cox proportional hazards analysis was used further to evaluate survival while controlling for demographics and co-morbidities. All demographics and co-morbidities that met the proportional hazards assumptions were listed for potential inclusion in the model. Proportional hazards assumptions were assessed by evaluation of Schoenfeld residuals and Kaplan-Meier curves for each variable. Backward selection was then used to further limit the number of variables to a more appropriate events-per-variable threshold [11,12]. A post hoc survival analysis (four year) was performed excluding all patients for whom less than two-thirds of their infectious episodes received initial antimicrobial therapy. Statistical significance was defined as an alpha value of less than 0.05. All statistical analysis was conducted using SAS software, version 9.3 (SAS Institute, Cary, NC).
Results
Follow-up data were available on 190 (94.5%) of the original 201 patients with ICU-acquired infections. There were no statistical differences between the original and follow-up cohorts with these 11 patients missing. The remaining patients were evenly divided between the two study groups with 95 patients in each group. There were no differences in patient demographics and co-morbidities based on study period (Table 1). Patients in the aggressive antibiotic group received a median of one additional day of antibiotic agents (five days on average). There was no difference in days from ICU admission to infection between groups.
APACHE = Age and Acute Physiology and Chronic Health Evaluation; WBC = white blood cell count; IQR = interquartile range; SEM = standard error of the mean.
Data presented as median (IQR).
Defined as baseline creatine ≥2.0 mg/dL.
Refers to any renal replacement required at the time of diagnosis.
Patients in this analysis had 456 instances of ICU-acquired infection during the study period. Two hundred fifty-one (55.0%) of these occurred in the aggressive group while 205 (45.0%) occurred in the conservative group. Each patient had a median of two ICU-acquired infections (interquartile range [IQR] 1–3), with no differences in the median number of infections per patient between groups. When evaluated on a per patient basis, there were no differences in the number of patients who had appropriate initial antimicrobial therapy at least two-thirds of the time. As in the original analysis, there were more episodes of pneumonia in the conservative group than the aggressive group.
There were no other differences in ICU-acquired infection sites based on study period. Infection sites are listed in order of frequency in Table 2. The original analysis identified lower rates of methicillin-resistant Staphylococcus aureus in the conservative group (7% vs. 2%; p = 0.004) and higher rates of Escherichia coli (4% vs. 12%; p = 0.004) compared with the aggressive group. A more complete list of identified organisms can be found in the original analysis [3]. A per-patient list of antimicrobial agents is included in Table 3.
Percentages add up to more than 100% because patients received multiple antimicrobials.
Overall deaths at 1 year were higher in the aggressive group (33.7% vs. 19.0%; p = 0.02); however, this difference was no longer evident by four years of follow-up (41.1% vs. 30.5%; p = 0.13). Similarly, patients in the aggressive group had a lower one-year survival probability on Kaplan-Meier analysis (Fig. 1) than those in the conservative group (p = 0.02). There was a trend toward lower four-year survival probability in the aggressive group, which did not reach statistical significance (p = 0.06).
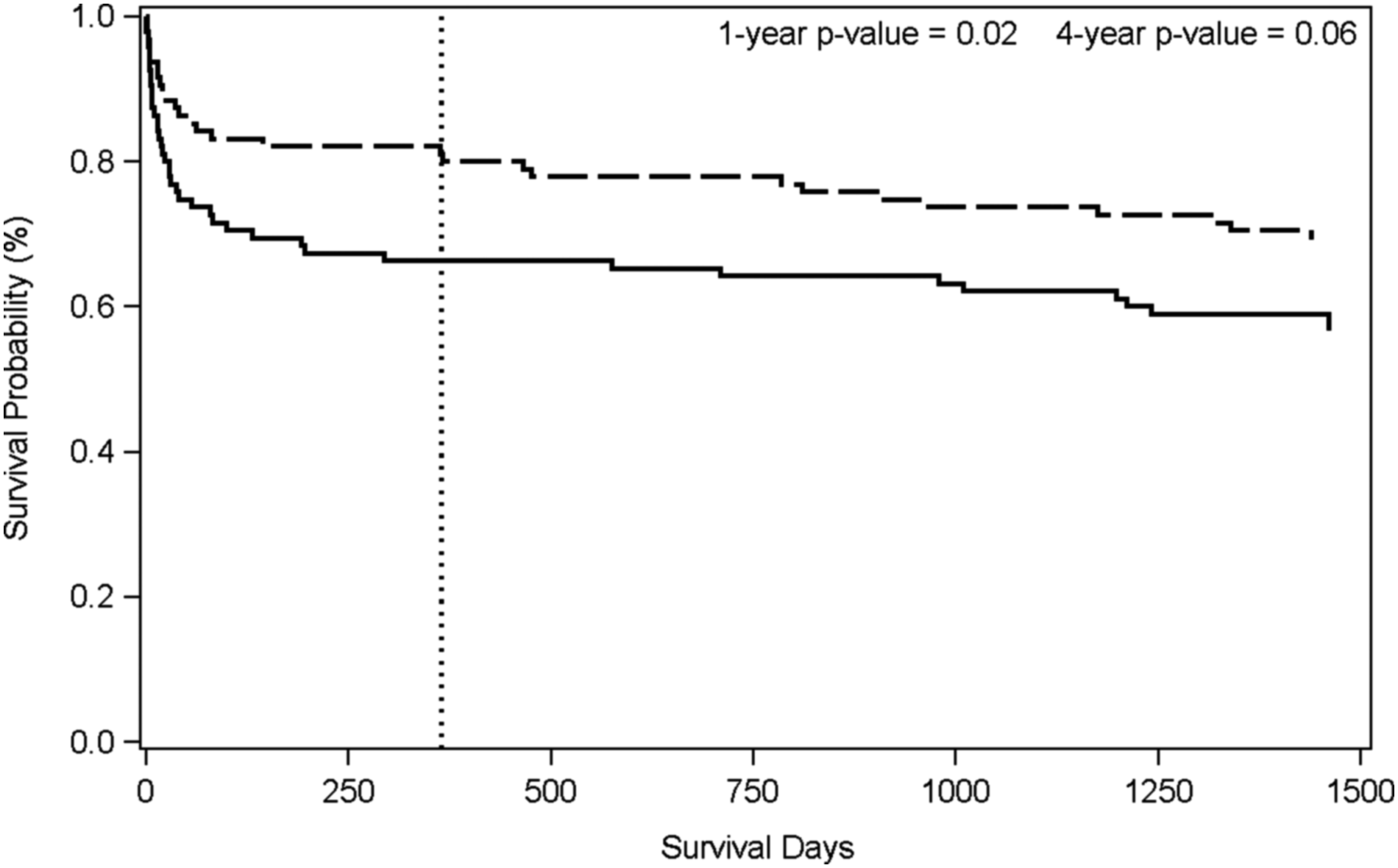
Unadjusted survival. Solid line = aggressive group; dashed line = conservative group; Vertical line = one-year survival.
The variables—patient gender, cerebrovascular disease, ventilator dependence, transfusion requirement, penicillin use, aminoglycoside use, and having appropriate initial empiric therapy in at least two-thirds of infectious episodes—did not meet the proportional hazards assumption and were therefore excluded from further modeling. The remaining variables were used in the Cox proportional hazards analysis and further limited using backward selection. The results of our proportional hazards model are listed in Table 4. Aggressive antimicrobial exposure was a significant predictor of death at both one and four years follow-up (hazard ratio [HR]: 2.26 and 1.70, respectively).
CI = confidence interval; APACHE = Age and Acute Physiology and Chronic Health Evaluation.
Defined as baseline creatine ≥2.0 mg/dL.
No significant association was identified at 1 year and therefore was not included in the model.
Refers to any renal replacement required at the time of diagnosis.
A post hoc proportional hazards analysis of only patients for whom two-thirds of their infectious episodes received appropriate initial antimicrobial therapy did not demonstrate an association between antimicrobial exposure group and four-year survival. There was a trend toward exposure group being a significant predictor (p = 0.054) but did not reach the threshold for inclusion in the model. Age 60–70 years (HR: 3.04; 95% confidence interval [CI]: 1.51–6.13) and malignancy (HR: 2.60; 95% CI: 1.09–6.18) were associated with poor survival, while trauma (HR: 0.37; 95% CI: 0.18–0.76) was associated with increased four-year survival.
Discussion
In this follow-up analysis of ICU patients who were treated according to different antimicrobial initiation thresholds, we observed a persistent and independent association between aggressive antimicrobial initiation and long-term deaths at one and four years. There is evidence to support the notion that differential antimicrobial exposures may influence outcomes beyond the immediate infectious episode or hospitalization.
Antimicrobial exposure is a known risk factor for the development of Clostridium difficile for several months after administration [13–15]. In addition, antimicrobial exposure has been associated with not only an increased risk of subsequent infection, but also increased deaths, hospital length of stay, re-admissions, and costs after subsequent infectious episodes [7–10]. These outcome differences were observed with antimicrobial exposures up to 90 days before the index infection [8–10]. Given these observations, the standard convention of evaluating 30-day or in-hospital outcomes for surgical infections may be somewhat shortsighted.
We observed a significant and surprising duration of effect from what would otherwise be considered a small variation in exposure. What factors could be driving this observation? We suggest that variations in the response of the host microbiome to the timing and duration of antimicrobial therapy may play a role. We are only just beginning to understand the role of normal host flora on homeostasis. In particular, commensal microbes play an important immunomodulatory role in response to stress, not only affecting the host's stress response, but also modulating the responses of other local flora [16]. Gut diversity can diminish in as little as six hours after the onset of an acute illness, setting the stage for opportunistic pathogens to proliferate and transition to a more lethal phenotype [16,17].
The addition of unnecessary antimicrobial pressure may be enough to hasten this process, or exacerbate it in persons who otherwise might have had enough microbiologic reserve to survive their insult. In other words, unnecessary antimicrobial exposure, particularly early in a disease process, may select out a group of patients who were more reliant on the immunomodulatory properties of their commensal gut flora, thereby increasing deaths in this group.
This process may explain why recent studies of antimicrobial duration in the convalescent phase fail to identify the same death difference observed in our study [3,18]. Re-colonization after injury can be variable and may have significant impacts on the host's subsequent metabolic profile, potentially resulting in a permanent alteration in microbiome diversity [19]. These changes may affect patient outcomes for years into the future and in ways we have not yet begun to evaluate [4–6,20].
Recent studies, including a large meta-analysis, have found no association between the timing of antibiotic agents and death in patients with severe sepsis and septic shock [2,21]. The majority of the studies included in the meta-analysis were either prospective observational or retrospective suggesting that observed delays in antimicrobial administration might be representative of underlying delays in other aspects of care such as resuscitation and source control. For surgical patients in particular, the timing of antimicrobial agents may not be as important as source control [22].
The heterogeneity in these observational studies may limit the ability to detect significant differences in outcomes based solely on variations in antimicrobial exposure. In our analysis, patients from both groups received resuscitation and source control in a timely manner [3]. The “delay” in antimicrobial therapy was intentional and was the primary difference between groups. Interestingly, while not statistically significant, Puskarich et al. [23] demonstrate a trend toward improved survival with increasing delays in antimicrobial administration for patients undergoing active resuscitation. Our study suggests that thoughtful withholding of antimicrobial agents in the setting of otherwise appropriate management may be beneficial or at least not harmful.
The appropriateness of initial therapy has also been called into question. Several studies have suggested that the appropriateness of empiric antimicrobial therapy has no impact on deaths, while others observe increased risk with inappropriate therapy [8,23–25]. In our original analysis, infectious episodes in the conservative group were more likely to receive appropriate initial antimicrobial therapy, which may also have impacted survival [3]. In this analysis, however, when analyzed on a per patient basis, the previously observed difference is absent. Individual patients with multiple infectious episodes will have some variability in the appropriateness of empiric therapy for each episode. The effect of a single episode of inappropriate initial antimicrobial agents is therefore diluted over the course of an entire hospitalization.
It is therefore not surprising that we found no difference on our univariable analysis. When we limited our survival analysis only to patients who mostly received appropriate initial therapy, the timing of antimicrobial agents was not a significant predictor of survival. There was, however, a trend toward significance despite the much lower sample size. It would be reasonable to assume that the effect of inappropriate antimicrobial therapy would blunt or trump the effect of antimicrobial timing, but we have no strong evidence either way at this time. This analysis should be repeated with a larger data set to see if this finding persists. It is interesting to consider what impact antimicrobial exposure has on the host microbiome, appropriate or otherwise, and what role the microbiome may play in the observed heterogeneity in antimicrobial appropriateness studies.
This study has several important limitations. First, as a retrospective follow-up analysis of a single institution study, our results may not be broadly generalizable and could suffer observation bias inherent to this type of study. Second, while we had survival data on 94.5% of the original cohort, there remains a possibility that our data may not reflect our true deaths, particularly for patients who reside, or moved, out of state. Also, our vital statistics data available through the CDR do not include cause of death, which would be informative in this cohort. Third, there may be additional differences, which we are unable to assess given our small sample size. In addition, while we suspect that variations in the microbiome-dependent immunomodulation may play an important role in these findings, we are not yet able to obtain microbiome-specific data. Additional data are needed to test the validity of this hypothesis. Finally, there remains the possibility of a type I error caused by unknown variables not included in this analysis. We recommend a larger multi-center trial to further evaluate this phenomenon.
Conclusion
In this follow-up analysis of a prospective study aimed at modulating antimicrobial initiation in critically ill patients with suspected infection, we demonstrate that aggressive antimicrobial administration remained an independent risk factor for death at both one-year and four-year periods. These data suggest that unnecessarily aggressive antimicrobial administration may have substantial negative side effects, which persist for a longer period than expected initially. Exact mechanisms for these findings remain unclear, although microbiome-related processes are suspected. Further study is needed into the interaction between timing and appropriateness of antimicrobial therapy in critical illness.
Footnotes
Author Disclosure Statement
“No competing financial interests exist.