
Abstract
Abstract
Background:
Surgical site infections (SSIs) are one of the most common hospital-acquired infections. To reduce SSIs, prophylactic intra-operative wound irrigation (pIOWI) has been advocated, although the results to date are equivocal. To develop recommendations for the new World Health Organization (WHO) SSI prevention guidelines, a systematic literature review and a meta-analysis were conducted on the effectiveness of pIOWI using different agents as a means of reducing SSI.
Methods:
The PUBMED, Embase, CENTRAL, CINAHL, and WHO databases were searched. Randomized controlled trials (RCTs) comparing either pIOWI with no pIOWI or with pIOWI using different solutions and techniques were retrieved with SSI as the primary outcome. Meta-analyses were performed, and odds ratios (OR) and the mean difference with 95% confidence intervals (CI) were extracted and pooled with a random effects model.
Results:
Twenty-one studies were suitable for analysis, and a distinction was made between intra-peritoneal, mediastinal, and incisional wound irrigation. A low quality of evidence demonstrated a statistically significant benefit for incisional wound irrigation with an aqueous povidone–iodine (PVP-I) solution in clean and clean contaminated wounds (OR 0.31; 95% CI 0.13–0.73; p = 0.007); 50 fewer SSIs per 1,000 procedures (from 19 fewer to 64 fewer)). Antibiotic irrigation had no significant effect in reducing SSIs (OR 1.16; 95% CI 0.64–2.12; p = 0.63).
Conclusion:
Low-quality evidence suggests considering the use of prophylactic incisional wound irrigation to prevent SSI with an aqueous povidone–iodine solution. Antibiotic irrigation does not show a benefit and therefore is discouraged.
S
Many factors have been associated with the risk of SSI, and consequently, a range of preventive measures has been proposed. One of these is prophylactic intra-operative wound irrigation (pIOWI), a seemingly simple intervention defined by the flow of a solution across the surface of an open wound to achieve tissue hydration. It removes and dilutes body fluids, bacteria, and cellular debris and additionally may have a bactericidal effect when additives such as antibiotics or antiseptic agents are used (see Table 1 for an overview of the definitions used). As many as 97% of surgeons commonly practice IOWI [6,7]. Nonetheless, it is not part of general practice in every country or hospital. Moreover, methods differ depending on the patient population, surface of application, technique, and solutions used. Similar variations in methods and results can be observed in studies investigating the effect of IOWI [8].
Among the available guidelines on SSI prevention, few have addressed the topic of IOWI and give contradictory recommendations. The guidelines from the United Kingdom National Institute for Health and Care Excellence (NICE), issued in 2008 and updated in 2013, advised against IOWI and intra-peritoneal lavage [9]. In contrast, the 2014 guidelines of the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA) recommend using antiseptic incision lavage [10]. Many of the solutions commonly used for irrigation are not licensed for open incisions by the U.S. Food and Drug Administration [11].
In 2015, a meta-analysis has been published to determine the current state of knowledge on pIOWI [8]. However, that review does not take into account that (other) infection prevention measures among included studies have improved over decades. Therefore, the presented evidence may not be generalizable to current standard of care (i.e., no appropriate standard systemic antibiotic prophylaxis). Importantly, the previous review has included studies where pIOWI represents a therapeutic intervention for infection rather than a prophylactic measure. Also, a substantial heterogeneity between studies has not been accounted for as the previous review does not account for differences in irrigation solutions and in application methods. For the purpose of developing recommendations for the new World Health Organization (WHO) SSI prevention guidelines [12,13], a systematic literature review and meta-analysis were conducted. In present systematic review we aim to assess all available data reasonably applicable to current standard of care and clarify the effect of pIOWI on the incidence of surgical site infection in all surgical populations, while accounting for inter-study differences in application method and solution.
Patients and Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed [14].
Search strategy and selection criteria
The following databases were searched: Medline (PubMed); Excerpta Medica Database (EMBASE); Cumulative Index to Nursing and Allied Health Literature (CINAHL); Cochrane Central Register of Controlled Trials (CENTRAL); and WHO regional medical databases. No time limit was used because most studies were published before 1990. Language was restricted to English, French, German and Spanish. A comprehensive list of search terms was used, including Medical Subject Headings (MESH), the complete search is included in Appendix A (Appendices maybe found at www.liebertpub.com/sur).
Two independent reviewers screened titles and abstracts of retrieved references for potentially relevant studies. The full text of these articles was obtained and independently reviewed for eligibility based on inclusion criteria. Duplicate studies were excluded. Only randomized studies investigating pIOWI as described in Table 1 were included. Studies investigating the topical application of antibiotics and antiseptics (e.g., powder, gels, sponges) without the mechanical effect of irrigation, physically rinsing and diluting the bacterial load, were not included. To ensure that only evidence reasonably relevant to the current standard of care was included in our analyses, description of appropriate administration of preoperative antibiotic prophylaxis (i.e., before incision and intravenous) was a minimum requirement for inclusion. In addition, studies where the irrigated field was infected prior to the start of surgery and wound irrigation, represented a therapeutic intervention rather than a prophylactic measure and were also excluded. Wound contamination was ranked according to the US Centers for Disease Control and Prevention (CDC) wound classification [15]. As described in table 1, wound class I-III were considered not infected and therefore irrigation of the contaminated field a prophylactic measure, whereas CDC Wound class IV was considered a pre-existent infection and therefore irrigation of the contaminated field represented a therapeutic intervention. Irrigation of the newly made incisional wound was always considered prophylactic, regardless of the wound classification, as the incisional wound did not exist prior to the procedure and pre-existent infection would be impossible. For example, peritoneal cavity irrigation of a dirty, infected abdomen (CDC Wound class IV) represents a therapeutic intervention. In contrast, in the same procedure incisional wound irrigation was considered a prophylactic measure.
Data extraction and assessment of study quality
Data were extracted from the text, according to a pre specified data abstraction form including design, publication date, scope, number of patients, contamination according to the US CDC wound classification [15], irrigation surface, type of intervention (solution, application, volume), type of control, Follow-up, primary outcome, results and adverse events (AE) (Appendix B). The Cochrane Collaboration's tool [16] for assessing risk of bias was assessed for the quality of the studies. Any disagreements were resolved through discussion or after consultation with the senior author, when necessary. Publication bias was assessed using a funnel plot [17]. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology (GRADE Pro software, http://gradepro.org/) [18] was used to assess the quality of the body of retrieved evidence.
Synthesis of results
Trials were grouped in comparisons according to irrigation location and their intervention and control arm. Of each comparison meta-analysis were performed using Review Manager (RevMan, Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014) as appropriate. If there was only one study no data could be pooled, but data were plotted as forest plot for illustrative purposes. Odds ratios (OR) and the mean difference with 95% confidence intervals (CI) were extracted and pooled for each comparison with a random effects model (Mantel-Haenszel method) to account for potential heterogeneity [19]. Forest plots were constructed and P < 0.05 was considered to be statistically significant. Heterogeneity was assessed using the I2 statistic. I2 of >60% was assessed as serious inconsistency. When inconsistency was detected stratified subgroup analysis where made for wound contamination and for irrigation solution.
Results
Study selection
We identified 955 studies, of which 113 were assessed for full review. Twenty-one randomized controlled trials (RCTs) were found eligible for full critical appraisal. The process of selection is summarized in Figure 1. The reasons for exclusion after full text assessment are described in Appendix C.
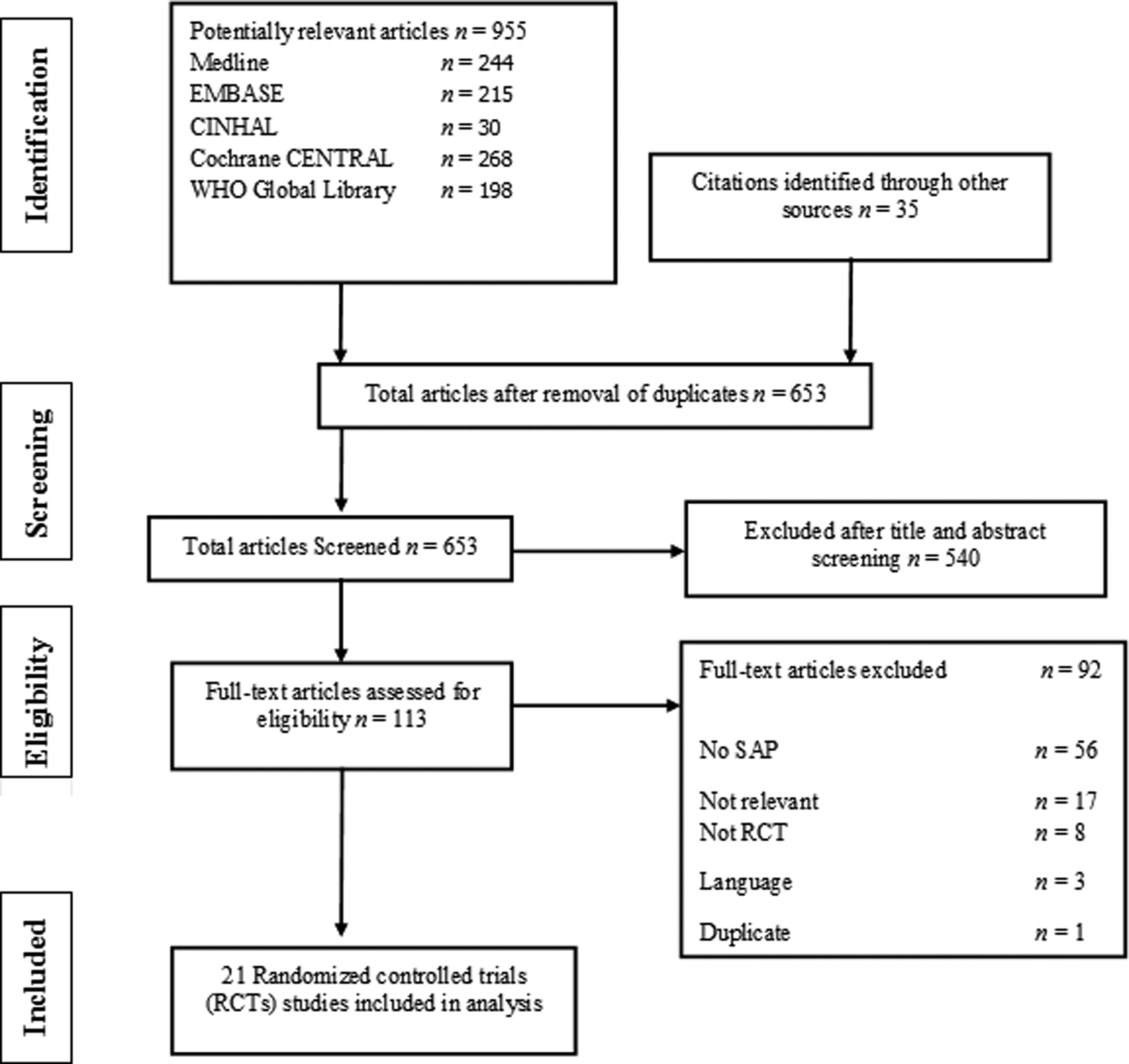
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart of the systematic review.
Study characteristics
In total we identified 21 RCTs [20-40] (6,224 patients) comparing pIOWI to no pIOWI or to pIOWI using different solutions and techniques, in patients undergoing various surgical procedures with SSI as an outcome. All but two [27,28] were single center RCTs. There was substantial heterogeneity in the study protocols. A distinction was made between peritoneal cavity, mediastinal cavity and incisional wound irrigation. Other main differences were the composition of the irrigation fluid, and the type of surgery with associated contamination. Due to this heterogeneity of the evidence, nine separate comparisons were composed. Five studies describing intraoperative peritoneal cavity irrigation [20–24] comparing saline vs. no irrigation [20], taurolidine vs. saline [21], and antibiotic irrigation vs. saline or no irrigation [22-24]; fifteen describing incisional wound irrigation [25-39] comparing saline solution vs. no irrigation [25], syringe pressure irrigation with saline solution vs. no irrigation [26], pulse pressure irrigation with saline solution vs. normal saline solution [27,28], aqueous povidone iodine (PVP-I) vs. saline [29-35] and antibiotic vs. saline solution or no irrigation [22,36-39]; and one study describing intra-operative mediastinal cavity irrigation [40] comparing aqueous PVP-I vs. saline solution. Most studies were conducted in patients undergoing abdominal surgery [20-24,26,28,31,32,36,37] but spine [33,34], orthopedic [27,35,39], gynecologic [25], vascular [38], thoracic [40], and general surgery [29,30] also were included. Of the included studies, three RCTs [20, 23, 31] described sterility of the irrigation fluid. The other studies did not report whether the irrigation fluid was sterile. The data on study characteristics are summarized in Table 2 and entirely presented in Appendix B.
This study described peritoneal as well as incisional irrigation. However, intra-abdominal infections were not included in the analyses because infection of this field was established.
C = control; CDC = Centers for Disease Control and Prevention; I = intervention; IW = incisional wound; LMW = low molecular weight; NA = not applicable; NR = not reported; PC = peritoneal cavity; PVP-I = aqueous povidone–iodine; SSI = surgical site infection; MC = mediastinal cavity.
Risk of bias
The results of the risk of bias evaluation are presented in Table 3. Overall, there was a serious risk of bias, predominantly attributable to unclear or high risk of selection and performance bias. Publication bias could not be detected or excluded. There was an insufficient number of studies included in the separate meta-analyses for appropriate interpretation of the funnel plots.
Data and analyses
A summary of the meta-analyses is presented in Table 4. For an extensive overview of all nine comparisons, corresponding data, and meta-analyses, we refer you to Appendix D.
No effective strategy for the reduction of SSIs with prophylactic peritoneal cavity irrigation was identified. Regarding incisional wound irrigation, mere saline was not effective in reducing SSIs [25]. However, when the saline was applied with a syringe to generate some pressure [26], a reduction in the risk of SSI compared with no irrigation was shown in one study (OR 0.35; 95% CI 0.19–0.65; P = 0.0009). This benefit also was demonstrated when pulse pressure irrigation with saline was compared with normal saline irrigation in a meta-analysis of two RCTs [27,28] (OR 0.30; 95% CI 0.08–0.86; p = 0.0003).
Irrigation with aqueous povidone–iodine demonstrated a significant benefit compared with saline irrigation in a meta-analysis of seven RCTs [29-35] (OR 0.31; 95% CI 0.13–0.73; p = 0.007; Fig. 2A–C). This effect equals 50 fewer SSIs per 1,000 procedures (from 19 fewer to 64 fewer) (Appendices D and E comparison 7). The results where stratified according to subgroups based on the extent of wound contamination (Fig. 2B) and povidone–iodine concentration (Fig. 2C) to account for heterogeneity in the pooled analysis (I2 = 63%). With this measure, heterogeneity decreased to an I2 of 43%. The effect of irrigation with aqueous povidone–iodine on SSIs was attributable to incisional wound irrigation in clean and clean-contaminated procedures with PVP-I 10% and PVP-I 0.35%, respectively. No dose–response effect was seen.

Forest plot of incisional irrigation with various solutions.
Antibiotic irrigation of the incisional wound showed no effect on SSI rate compared with no irrigation or saline irrigation in a meta-analysis of five RCTs [22,36-39] (OR 1.16; 95% CI 0.64–2.12; p = 0.63) (Fig. 3). This lack of effect equals 12 more SSIs per 1,000 (from 27 fewer to 76 more) (Appendices D and E comparison 8). Only one study reported on mediastinal irrigation with aqueous povidone–iodine compared with saline and showed no benefit of the former [40].
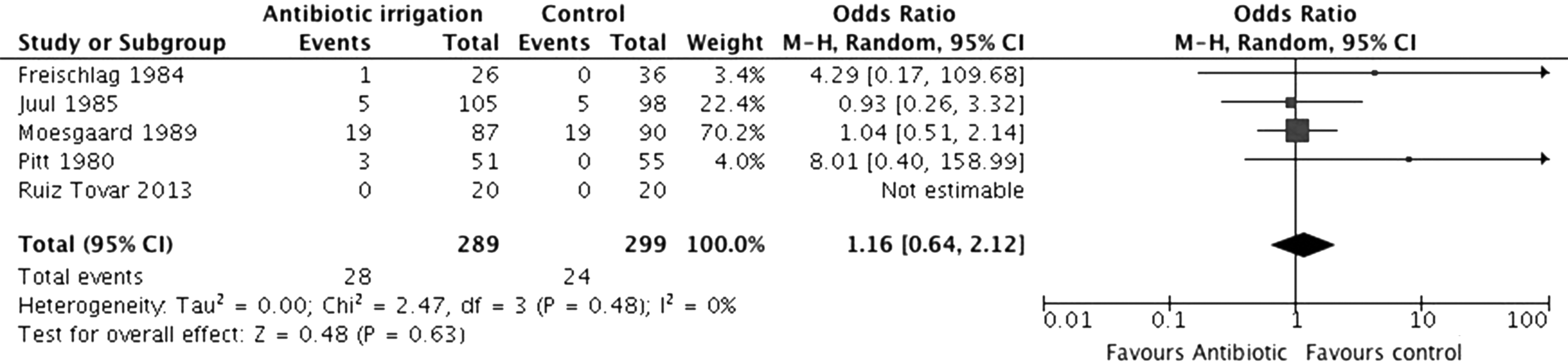
Forest plot of incisional wound irrigation with antibiotic vs. saline irrigation or no irrigation.
Adverse events
Among the included studies, six [29,31,33,34,36,41] reported no adverse events attributable to the intervention. Among these, two studies [33,34] investigating PVP-I incision irrigation in spinal surgery specifically reported no difference in fusion time or bone quality. One study [31] investigating PVP-I incision irrigation in abdominal surgery specifically reports a transient nine-fold serum iodine elevation (median 162 mcg/dL; range 27–1170 mcg/dL) but no signs of toxicity. After seven days, serum iodine concentrations had returned to the pre-operative range.
GRADE
GRADE tables with full assessment of the individual comparisons are presented in Appendix E. Overall, the quality of evidence was assessed as moderate to very low because of the serious risk of bias and serious imprecision.
Discussion
Evidence of low quality shows that prophylactic incisional irrigation with aqueous PVP-I solution has a significant benefit on the SSI rate, particularly in clean and clean-contaminated wounds. No dose–response effect was detected. With respect to incisional irrigation with saline, evidence of moderate to very low quality shows a significant effect on SSI rate when applied with force or using pulse pressure, but not with regular irrigation. There is no significant benefit to the use of antibiotic solutions for prophylactic incisional wound irrigation or for the use of pIOWI in the abdomen or mediastinum.
Although recommendations from existing guidelines are conflicting [9,10] and recent well-designed RCTs are lacking, as many as 97% of surgeons irrigate wounds in an effort to reduce the risk of SSI [6,7]. The most commonly used irrigation solution is saline followed by aqueous PVP-I or antibiotic solutions [6,42,43]. The efficacy and clinical safety of irrigation with these solutions has been the subject of debate [11, 44]. Various concentrations of PVP-I are effective rapidly against a broad spectrum of pathogens, methicillin-resistant Staphylococcus aureus (MRSA) included [45,46]. However, some in vitro studies [47-49] have reported a negative effect of PVP-I on tissue regeneration, and older case studies describe serum iodine toxicity as a result of irrigation [50-52]. However, these adverse effects could not be substantiated in clinical trials [29-35;41]. When considering antibiotics, the bactericidal effect of most agents requires a substantial duration of contact time. It is unlikely that pIOWI with antibiotic solutions is performed with sufficient time to achieve clinical efficacy, and anaphylactic reactions have been reported [53]. In addition, the misuse of antibiotics is considered to be a major driving force in the emergence of antimicrobial resistance [54-56]. In contrast, resistance of organisms to antiseptics is suggested to be low, possibly because of their multiple pharmacological targets [57,58]. Wound irrigation using aqueous chlorhexidine (CHX) may be an alternative when extrapolating the favourable results from alcohol-based CHX used for pre-operative skin preparation, but clinical data are lacking. The results of aqueous 0.05% chlorhexidine gluconate as a wound irrigation fluid in the laboratory and animal studies are promising [59,60].
Previous meta-analyses have assessed the effect of pIOWI but with serious limitations in their study selection, impeding extrapolation to current clinical practice. Fournel et al. [61] performed a systematic review of PVP-I in various applications and found a reduction of the incidence of SSI after aqueous PVP-I irrigation. Mueller et al. [8] assessed pIOWI systematically with saline, PVP-I, and antibiotic solutions and concluded that both PVP-I and antibiotic irrigation are effective in the reduction of SSI. However, both these reviews included studies investigating IOWI as a therapeutic measure for existing infections rather than as a preventive measure, and studies investigating IOWI did not meet current standards of systemic antibiotic prophylaxis. Fournel et al. [61] conducted a subgroup analysis of studies involving standard systemic antibiotic prophylaxis but left relevant studies out [29,30,35]. Mueller et al. included PVP-I powder (spray) application among IOWI studies using an irrigation solution, but the mechanical effect of removal and dilution of the bacterial load is not achieved by powder application. Present systematic review specifically investigates the prophylactic effect of IOWI on the incidence of SSI against the background of current standard of care.
The limitations of the present study are generally the result of deficiencies of the individual studies. The samples are small, resulting in little power per study and a high risk of failing to detect a true effect (β or Type two error). By conducting a meta-analysis, the power is increased and the risk of failing to detect a true effect reduced. Published studies on pIOWI were conducted mostly in the 1980s, which may represent a limitation, as infection prevention and control measures have changed substantially since that time. Similarly, standards for the conduct and reporting of clinical trials have changed, resulting in a stringent assessment of the quality of evidence. Strict inclusion criteria have limited the total number of appropriate studies to 21 RCTs. Variation is seen in the definition of SSI and followup duration (Appendix B), as the widely accepted definition of the CDC was first published in 1999 [15]. Therefore, SSIs may be overdiagnosed or underreported. And finally, the exposure times and application methods were heterogeneous.
In the absence of a proved effect of antibiotic irrigation and based on the risk of emerging antimicrobial resistance associated with the unnecessary use of antibiotics, irrigation with antibiotic solution should be avoided. Low-quality evidence suggests benefit from incisional wound irrigation with aqueous povidone–iodine. New high-quality RCTs are needed but might not have priority, considering the relatively large effect of prophylactic incisional wound irrigation using aqueous povidone–iodine. A combined approach of several interventions to reduce SSIs may be more favorable because it has become apparent that a bundle approach has been successful in some studies [62-64].
Footnotes
Acknowledgments
This review was conducted in line with the development of the Global Guidelines for Prevention of Surgical Site Infections commissioned by the World Health Organisation (WHO) in Geneva. We received no funding to perform this research.
S.W. de Jonge, Q.J.J. Boldingh, J.S. Solomkin, B. Allegranzi, and M. Egger declare no conflicts of interest.
E.P. Dellinger reports personal fees from Merck, Ortho-McNeil, Targanta, Schering-Plough, Astellas, Allergan, Care Fusion, Durata, Pfizer, Applied Medical, Rib-X, Affinium, Tetraphase, Televancin, R-Pharm, Cubist, Melinta, and 3M and grants from Motif for research outside the submitted work.
M.A. Boermeester reports institutional grants from J&J/Ethicon, Acelity/KCI, Allergan/LifeCell, Ipsen, Baxter, Mylan, Bard, advisory board member of J&J/Ethicon, Acelity/KCI, and Allergan/LifeCell for research outside the submitted work.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.