
Abstract
Abstract
Background:
The purpose of our study was to determine prospectively relationships between plasma mitochondrial deoxyribonucleic acid (mtDNA) concentration and clinical outcome in patients with intra-abdominal infections (IAIs) induced by severe abdominal trauma.
Patients and Methods:
The DNA was isolated from serum samples taken from patients with IAIs at hospital days zero, one, and two. Plasma mtDNA concentration was assessed by real-time polymerase chain reaction (PCR). The study population's clinical and laboratory data were analyzed.
Results:
The mtDNA damage-associated molecular patterns were expressed as a PCR threshold cycle number using four selected sequences. The patients with IAIs had significant higher plasma mtDNA than healthy control subjects. Patients with IAIs with sepsis apparently had elevated mtDNA levels compared with non-septic patients with IAIs (30.9 ± 2.0 vs. 28.7 ± 2.4; 33.3 ± 2.6 vs. 28.9 ± 2.4; 32.9 ± 1.6 vs. 31.2 ± 2.2; 33.1 ± 3.6 vs. 28.1 ± 2.2, respectively). Patients with IAIs in whom multiple organ dysfunction syndrome (MODS) developed also had increased mtDNA concentration compared with those who did not (31.0 ± 1.8 vs. 27.9 ± 1.8; 32.9 ± 2.4 vs. 27.8 ± 1.7; 32.9 ± 1.5 vs. 29.8 ± 1.7; 32.0 ± 3.8 vs. 27.1 ± 2.1, respectively). Baseline mtDNA concentration had high effectiveness in predicting death for patients with IAIs who had severe trauma using receiver operating characteristic analysis. Furthermore, serum mtDNA levels on admission correlated with the lactate concentration, but no significant correlations were found between mtDNA levels and levels of white blood cells, C-reactive protein, and procalcitonin.
Conclusions:
Plasma mtDNA was associated with the occurrence of sepsis, MODS, and death in patients with IAIs caused by severe abdominal trauma.
I
Furthermore, victims of intra-abdominal trauma are at significant risk of incurring an infection because of peritoneal contamination by gastrointestinal contents [5]. Therefore, these patients commonly are admitted to the intensive care unit (ICU), especially those with severe abdominal trauma. The mortality rate secondary to IAI is high, ranging from 1% to 7%, and it can rise up to 50% if the diagnosis is delayed after development of MODS [6].
In the recent decade, accumulating evidence revealed that mitochondrial DNA (mtDNA) may act as an alarm or damage-associated molecular pattern (DAMPs) when released from injured cells into the circulation and result in functionally important immune consequences. Plasma mtDNA DAMPs levels were elevated in patients with a variety of critical conditions, including trauma, severe sepsis, and malignancy etc. [7–9]. Gu et al. research group demonstrated that plasma mtDNA increased soon after trauma and was positively correlated with the severity of injury [10]. In addition, a series of studies demonstrated that mtDNA could be recognized by pattern recognition receptors and triggered immune inflammatory responses [11–13].
Recently, newly discovered cyclic guanosine monophosphate-adenosine monophosphate synthase-stimulator of interferon genes (cGAS-STING) signaling is responsible for mtDNA recognition and potentially participates in the inflammatory process [14]. Considering the pro-inflammatory potential of circulating plasma mtDNA, we hypothesized that the circulating plasma mtDNA level was probably associated with the development of IAIs-related complications caused by abdominal trauma.
The MODS is a common and potentially fatal consequence of IAIs. Although mitochondrial and bioenergetic dysfunction have been incriminated in the pathogenesis of MODS for many years, involvement of mitochondria-derived DAMPs may be more dynamic than appreciated previously, and the association between mtDNA DAMPs and human MODS also remains largely speculative [15–17]. In addition, to date, there are still no studies investigating mtDNA levels and clinical outcomes specifically in patients with IAIs. Thus, the aim of the present study was to investigate the association between circulating plasma mtDNA levels and MODS, sepsis, and death in patients with IAIs induced by severe abdominal trauma.
Patients and Methods
Ethics statement
This study protocol was approved by the Institutional Review Board of Jinling Hospital, Nanjing. All patients and healthy adult volunteers provided written informed consent before any study-related procedure was performed.
Study population and definition
This prospective study cohort enrolled 36 consecutive severely injured patients who were admitted to the surgical intensive care unit (SICU) at Jinling Hospital from December 1, 2015 to June 1, 2016 (Supplementary Fig. 1; see online supplementary material at ftp.liebertpub.com/sur). Study enrollment criteria consisted of any patient with a diagnosis of IAI caused by severe abdominal trauma with an Injury Severity Score (ISS) greater than 15, age more than 18 years, and non-pregnant. The IAI in this study was defined according to the diagnostic criteria as described previously by our team [18]. For comparison, 10 age- or gender-matched healthy adult volunteers who received a physical examination and had no history of trauma or evidence of infection were recruited as healthy control subjects.
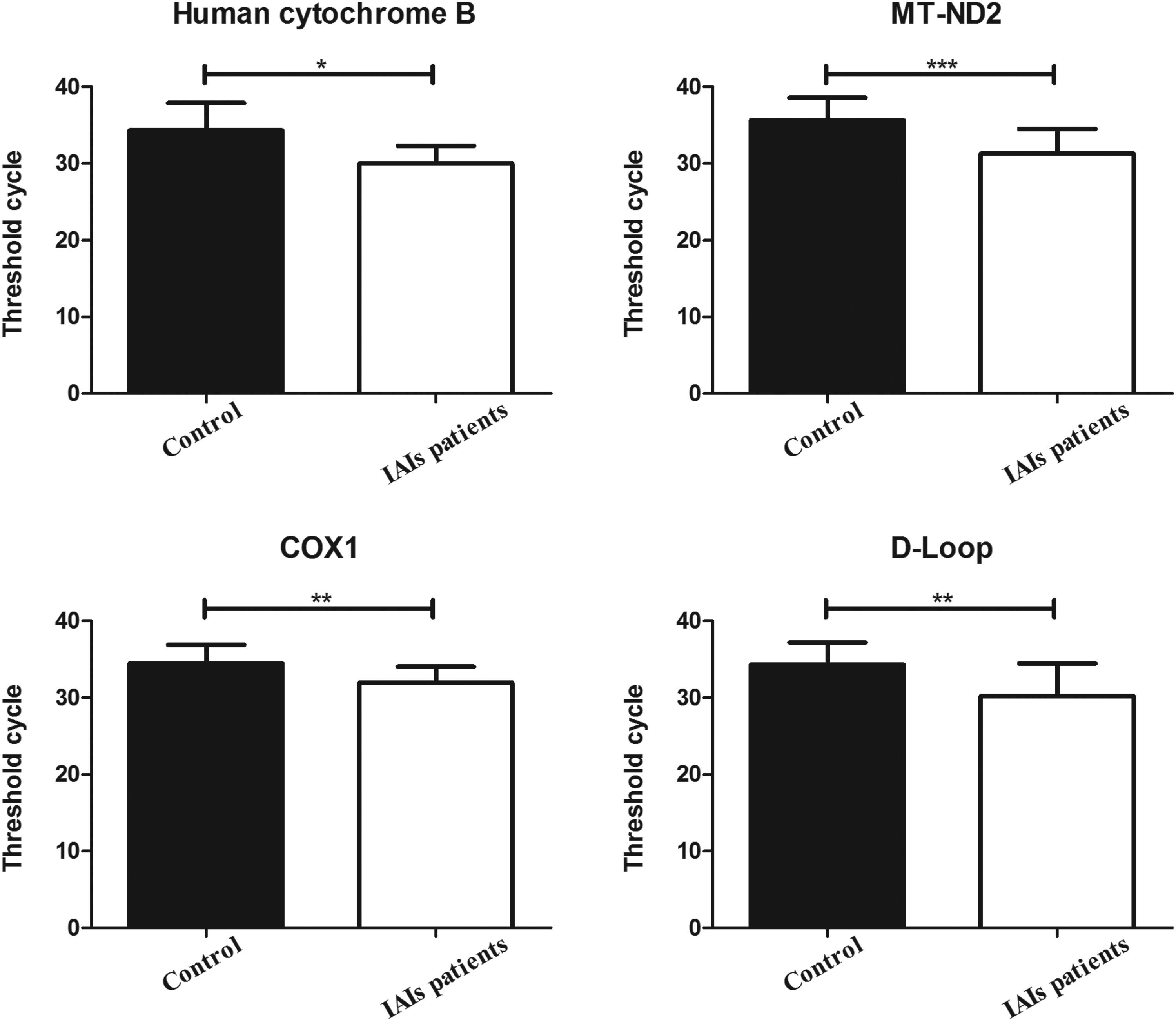
Box plots of the plasma mitochondrial deoxyribonucleic acid (mtDNA) concentration between the patients with intra-abdominal infections (IAIs) and healthy control subjects. Serum mtDNA concentrations are presented as mean ± standard deviation. *means p < 0.05; **means p < 0.01; ***means p < 0.001.
The primary outcome was death secondary to MODS or sepsis. Secondary outcomes included MODS and sepsis. The MODS was defined as a Denver Postinjury Multiple Organ Failure score of four or greater [19]. This scoring system rates the dysfunction of four organ systems (pulmonary, renal, hepatic, and cardiovascular), which is evaluated daily throughout the patient's SICU stay. Sepsis was defined by the American College of Chest Physicians (ACCP)/Society of Critical Care Medicine (SCCM) definition [20].
Blood sampling and assessment of plasma mtDNA
Blood samples were collected within two hours after admission to SICU and on days one and two after admission. Under minimal tourniquet pressure, a 3-mL blood sample was collected from the antecubital vein with a 19-gauge needle, and the patients were in a sitting position. These blood samples were collected into ethylenediaminetetraacetic acid (EDTA)-containing tubes and prepared for further mtDNA extraction. Clinical variables were recorded at the time of the blood draw; laboratory variables were obtained within four hours of blood sampling for mtDNA analyses.
To obtain cell-free plasma, EDTA blood was centrifuged initially for 10 minutes at 3,000 revolutions per minute (rpm), and the plasma was transferred into a clear polypropylene tube with great care not to disturb the buffy coat layer. Next, the newly separated plasma was centrifuged at 10,000 rpm for another 10 minutes, and the upper portion of the plasma was removed into another clear tube and stored at −80°C before DNA extraction. Double-centrifuged EDTA plasma was diluted 1:1 with phosphate buffered saline (PBS) after which DNA was isolated using the QIAamp DNA Blood Midi Kit (Qiagen, Valencia, CA), using the “Spin Protocol” as described by the manufacturer. Isolated DNA was stored at −20°C until further analysis.
Quantitative real-time polymerase chain reaction (qPCR), using USB VeriQuest Fast SYBR Green qPRC Master Mix (Affymetrix, Inc., Santa Clara) and the manufacturer's protocol were applied to quantify selected ∼200 bp sequences corresponding to the human cytochrome B: COX 1; MT-ND2; D-Loop mitochondrial genomic regions as described previously [21–23]. Primers for qPCR analyses of the indicated mtDNA sequences are listed in Table 1, and primer sequences have no significant homology with DNA found in any bacterial species published on Basic Local Alignment Search Tool.
MtDNA = mitochondrial deoxyribonucleic acid.
Samples that produced no PCR products after 40 cycles were considered “undetectable” and the Ct number was set to 40 for statistical purposes. The relative abundances of plasma mtDNA DAMPs were expressed as threshold cycles (Tc). Of note, higher Tc represent lower levels of mtDNA DAMPs. As negative controls, we verified that the selected mtDNA sequences were below detectable limits in solutions used in the assay and in plasma from control, non-injured human subjects, as reported previously [10.
Statistical analysis
Statistical analyses were performed using SPSS 19.0 statistical software (SPSS Inc. Chicago, IL). Several strategies were used to statistically evaluate the data in the present study. The mtDNA DAMPs level was expressed as a continuous variable and the occurrence of MODS, and sepsis, death as categoric variables. A receivers operating characteristic (ROC) curve was used to quantify the effectiveness of mtDNA DAMPs levels in predicting death for patients with IAIs. The optimal cutoff point was calculated by determining the index that provided the greatest sum of sensitivity and specificity. Correlation analysis was used to explore the relationships among plasma WBC, C-reactive protein (CRP), procalcitonin (PCT), lactate, and levels of serum mtDNA DAMPs on admission. Statistically significant differences (p < 0.05) were detected by non-parametric analyses.
Results
Clinical characteristics of the enrolled patients
There were 36 consecutive patients enrolled during the study period. Average age was 36.7 ± 11.7 years and ISS was 21.9 ± 5.2. Inducement of abdominal trauma in the present study consisted of 20 traffic accidents, eight fall injuries, five collision injuries and three sharp injury cases, and the major part of abdominal viscera and retroperitoneal trauma was gastrointestinal injuries (Table 2).
ISS = Injury Severity Score; MODS = multiple organ dysfunction syndrome.
Single organ injury, 32 cases; multiple organ injury, four cases.
A Denver Multiple Organ Failure score ≥4 at any time during the study was defined as MODS.
No statistically significant differences were found in age or ISS with regard to outcomes assessed in terms of sepsis (p = 0.21 and 0.13, respectively), MODS (p = 0.45 and 0.31, respectively) or death (p = 0.853 and 0.187, respectively). Furthermore, our results showed that the median serum mtDNA concentration, which quantified as PCR Tc for four selected sequences in patients with IAIs, was significantly higher than that of healthy control subjects (Fig. 1).
Association of mtDNA levels with MODS, sepsis, and death
There were 17 (47.2%) patients with a diagnosis of sepsis by the definition of ACCP/SCCM within 48 hours of presentation. In our cohort, MODS developed in 11(30.6%) patients with IAIs, and eight (22.2%) patients died during hospitalization. Patients with IAIs with sepsis had significantly higher plasma mtDNA levels than those non-septic patients with IAIs (Table 3). The mtDNA concentration in patients with IAIs and MODS were significantly elevated compared with those without (Fig. 2), and non-survivors had statistically higher mtDNA DAMPs than survivors (Fig. 4); Figure 3 had shown that there were intriguing trends relating maximum Denver Multiple Organ Failure scores and mtDNA concentration in our study. In addition, there were no statistical differences in age, ISS, types of trauma, transfused blood products, and rates of mechanical ventilation and renal replacement therapy between survivors and non-survivors for patients with IAIs (Table 4).
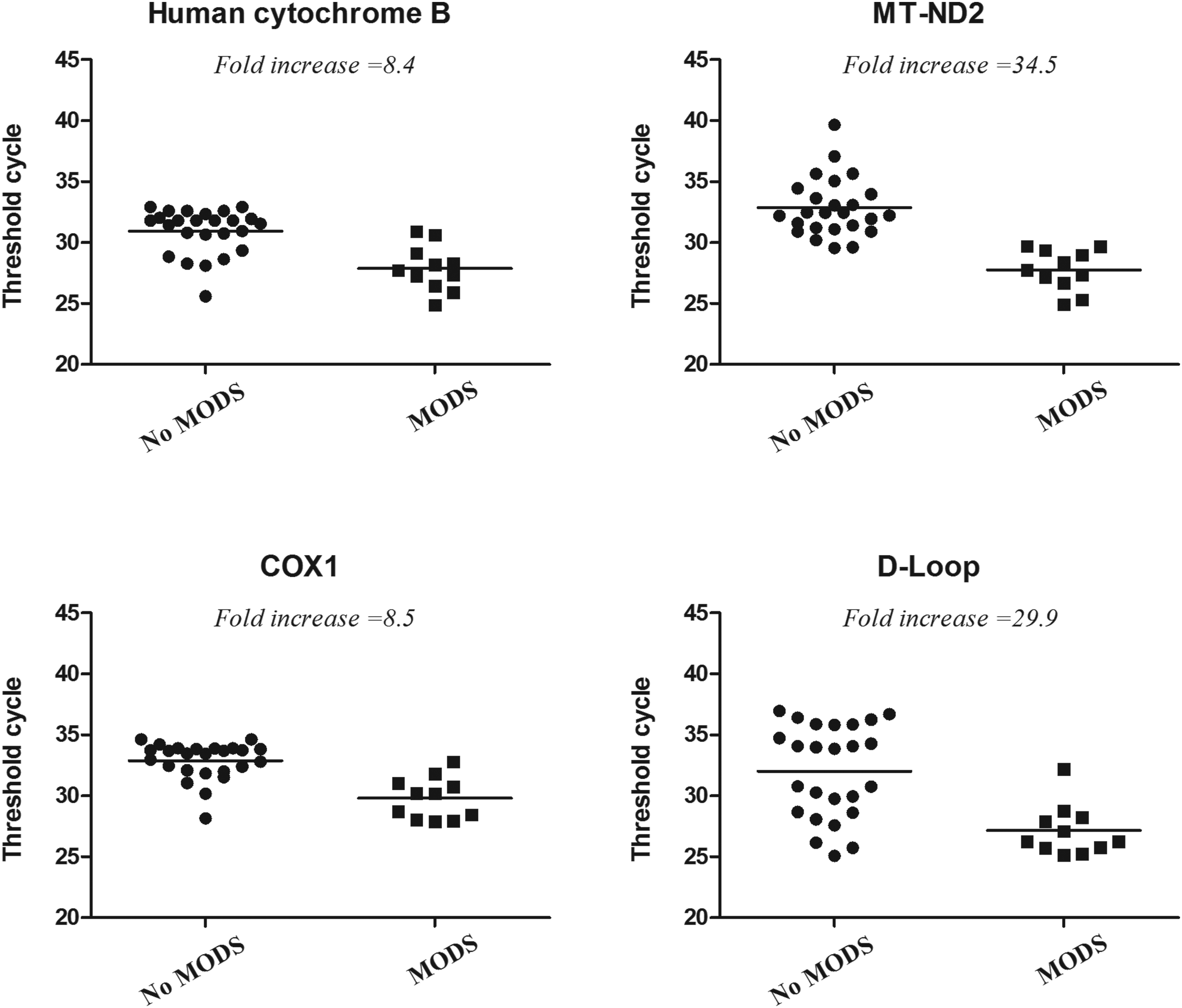
Associations between serum mitochondrial deoxyribonucleic acid (mtDNA) damage-associated molecular pattern levels with multiple organ dysfunction syndrome (MODS). The mtDNA levels were significantly increased in patients with intra-abdominal infections in whom MODS developed compared with patients without MODS. Four different sequences exhibited significant differences at p < 0.05 by non-parametric analyses. Lower threshold cycles number describes higher mtDNA concentration.
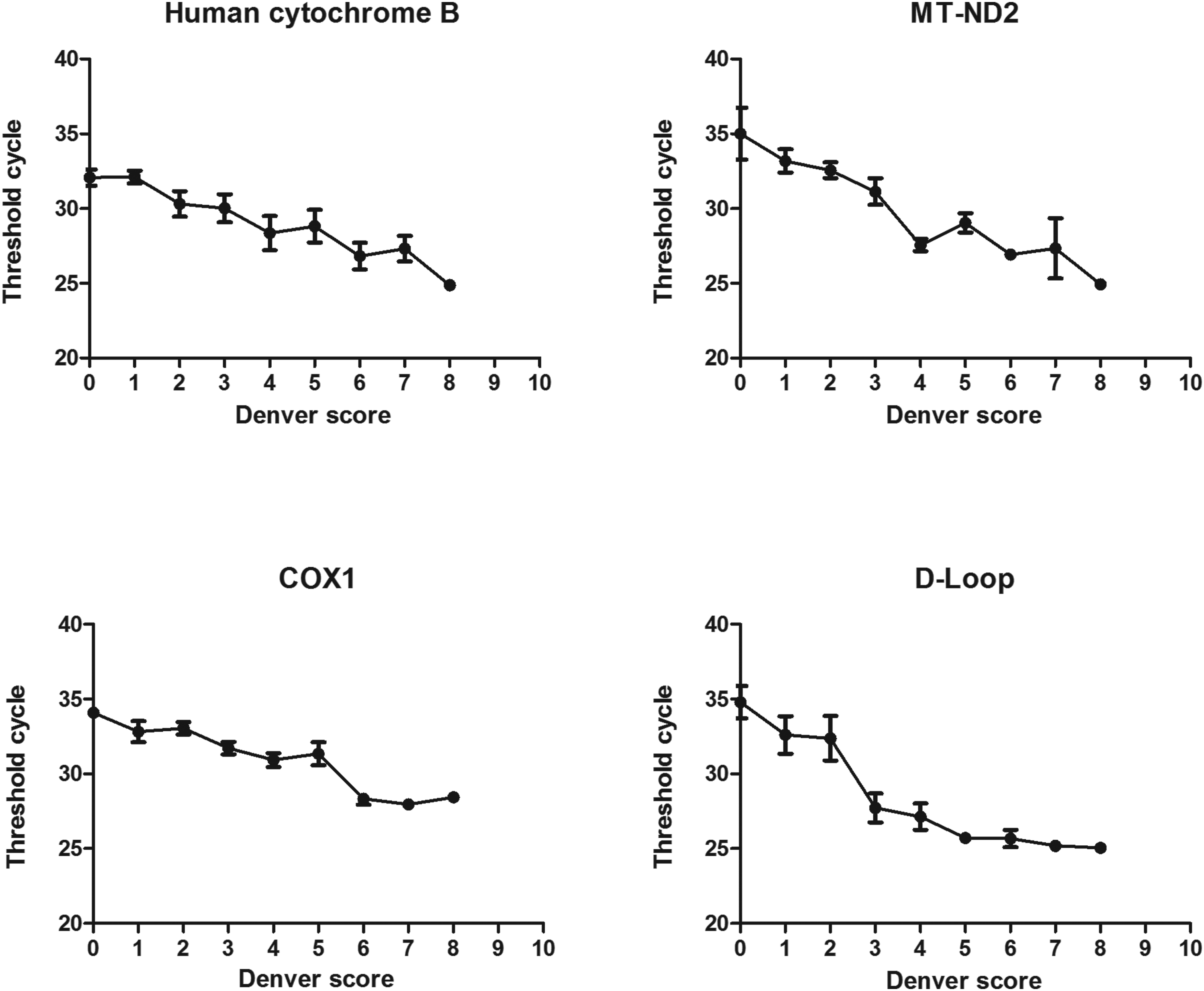
Plasma serum damage-associated molecular pattern levels expressed by threshold cycles represented as a function of the Denver Multiple Organ Failure Score.
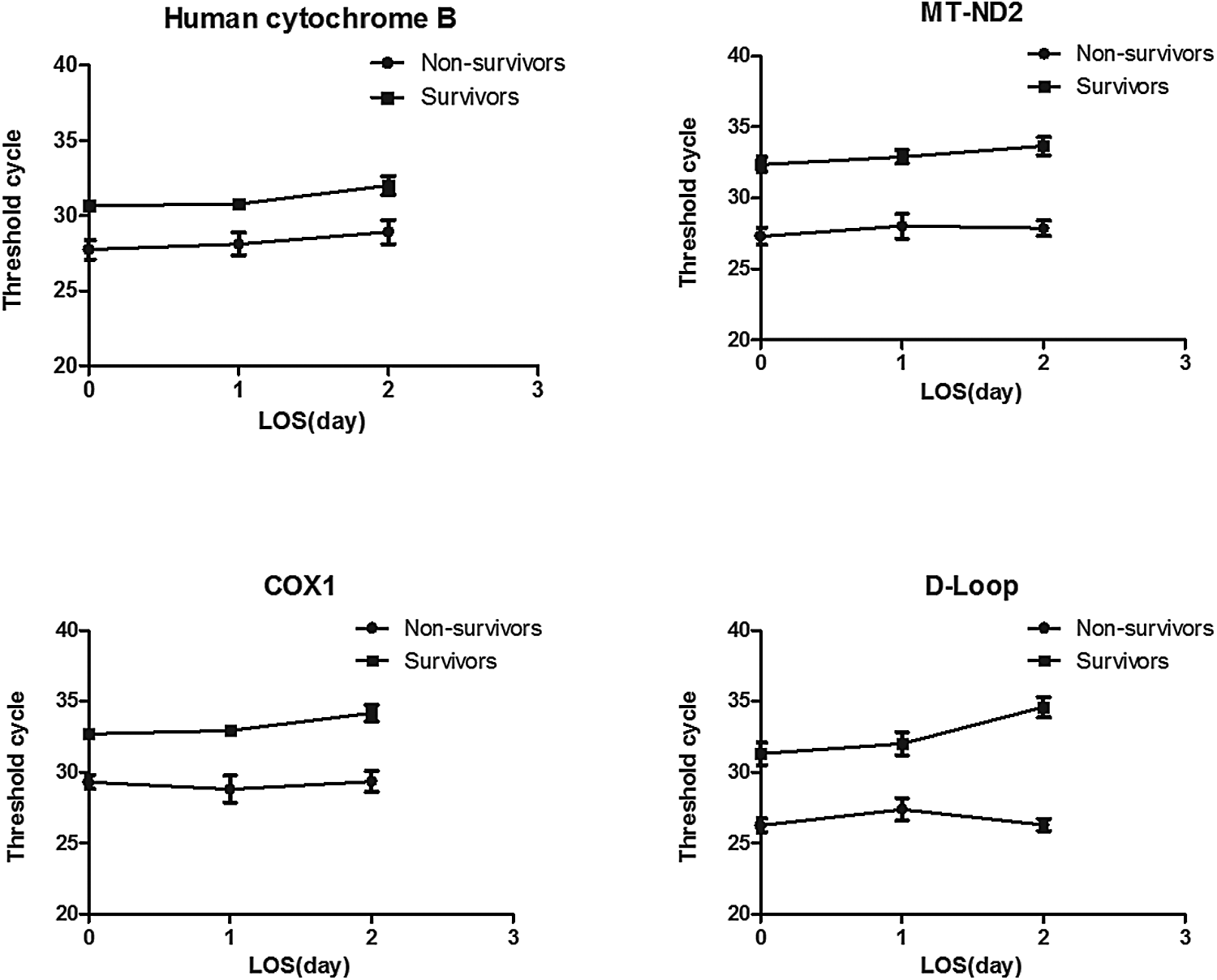
Plasma mitochondrial deoxyribonucleic acid (mtDNA) concentration was displayed at hospital admission and one and two days after admission. The mtDNA levels quantified by polymerase chair reaction threshold cycles did not significantly alter during hospital stays among four sequences for survivors and non-survivors in patients with intra-abdominal infections. LOS = length of stay.
mtDNA = mitochondrial deoxyribonucleic acid; DAMP = damage-associated molecular pattern; Tc = threshold cycles; MODS = multiple organ dysfunction syndrome.
p < 0.05.
Serum mtDNA DAMP levels for four different sequences were detected, segregating patients on the basis of the occurrence of sepsis and MODS, with statistical difference in every sequence. Each polymerase chain reaction cycle represents a doubling of DNA quantity, and fold increase describes the relative starting concentration of mtDNA in patients with intra-abdominal infections with adverse syndromes.
ISS = Injury Severity Score.
In the first 24 hours.
Transfusion requirements are described as total units of transfused products; all types include packed red blood cells, platelets, and fresh frozen plasma. No statistically significant differences were found in the group characteristics.
ROC cure analysis
Plasma mtDNA concentration was quantified as PCR Tc, with every cycle doubling DNA quantity until a detection threshold is achieved. A Tc 40 was considered as the limit of detection of template DNA, and all the Tc data for serum samples were below 40. Our result found that serum mtDNA levels did not significantly alter within two days in either survivors or non-survivors (Fig. 4). In the present study, ROC analysis was performed to evaluate the performance of serum mtDNA DAMPs levels at admission in discriminating survivors and non-survivors for patients with IAIs with severe abdominal trauma. The area under the ROC curves (AUC) of baseline mtDNA concentration using four mtDNA sequences in predicting death were 0.884, 0.826, 0.804, and 0.875, respectively (Fig. 5).
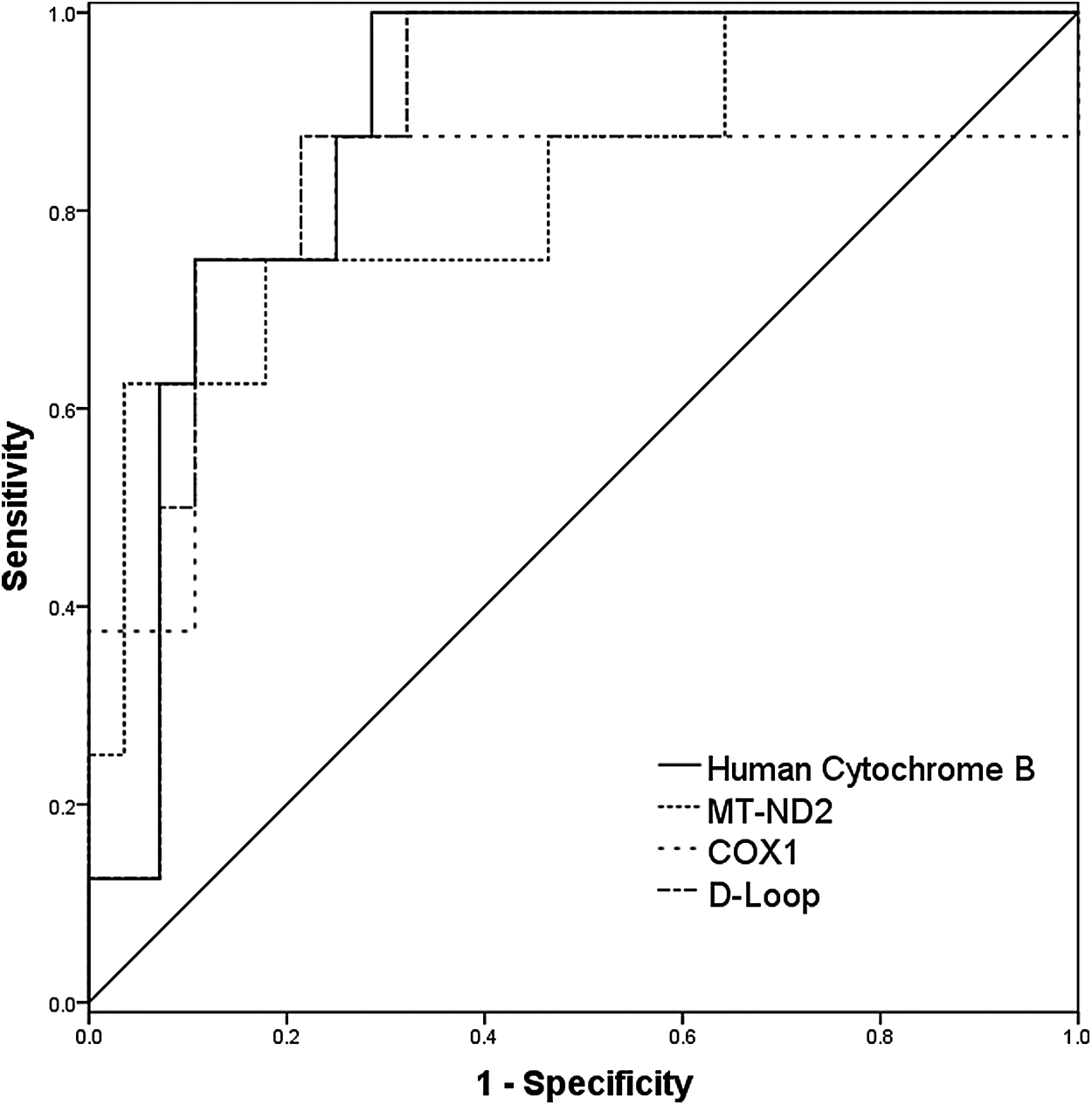
The receiver operating characteristic (ROC) curve for serum mitochondrial deoxyribonucleic acid damage-associated molecular pattern levels (quantified by threshold cycles) on hospital admission in predicting death in patients with intra-abdominal infections caused by severe abdominal trauma.
Correlation between plasma DNA and inflammatory biomarkers
By correlation analysis, the serum mtDNA DAMPs levels expressed as PCR Tc number on admission significantly correlated with the lactate concentration for four selected sequences (γ = −0.45, p = 0.0006; γ = −0.58, p = 0.0002; γ = −0.51, p = 0.002; γ = −0.49, p = 0.003, respectively) (Fig. 6). There were no significant correlations, however, between plasma mtDNA concentration and serum white blood cells (WBC), CRP, and PCT (data no shown).

Correlations between baseline mitochondrial deoxyribonucleic acid damage-associated molecular pattern levels and admission lactate concentration.
Discussion
To the best of our knowledge, our study is the first to explore the potential relationship between serum mtDNA DAMP levels and patients with IAIs induced by severe trauma. Infection after severe injury is common and has a huge impact on clinical outcomes, and nearly half of all initial survivors experience an infection during their hospital admission [24. Developing an infection is associated with increased critical care use, hospital stays, and death, and despite this, infection remains an underreported and underrecognized cause of morbidity in patients with trauma [25.
In addition, IAIs induced by abdominal trauma constitute one of the most frequent infectious problems and pose a substantial challenge to trauma specialists or general surgeons [6. Previous studies have demonstrated that plasma mtDNA DAMP concentration was increased significantly after trauma and that plasma mtDNA may be a promising marker for the prediction of trauma-related death [10. The relationship between the plasma mtDNA concentration and post-traumatic IAIs remains largely unknown, however. Thus, in this study, we investigated the significance of plasma mtDNA in IAIs caused by severe abdominal trauma.
In the present study, mtDNA concentration was defined as the mtDNA fragments that can be detected in circulating plasma, and especially in patients with IAIs, mtDNA levels had significantly elevated compared with those of healthy control subjects. Emerging evidence revealed that mtDNA fragments were derived from damaged mitochondria and released into the circulation after traumatic injury, which contributed to the development of sepsis and MODS [26.
Given the widespread recognition that oxidant stress is considered as a vital pathophysiologic component of severe trauma and post-traumatic infections, it is worth noting that serum mtDNA DAMPs are considerably more sensitive to oxidative damage than nuclear DNA [27. In addition, it is reported that mtDNA DAMPs increase permeability of cultured endothelial cells [28, thus imitating another important pathophysiologic process in MODS. Consistent with these results, our study demonstrated that median concentration of serum mtDNA DAMPs in sepsis and MODS group was significantly higher than in the patients without these syndromes. Furthermore, as shown in Figure 3, the trends of mtDNA concentration raised along with the increase of Denver Multiple Organ Failure scores for all selected mtDNA sequences.
The present study shows that the baseline plasma mtDNA concentration at admission had high effectiveness in predicting death for patients with IAIs with severe abdominal trauma using ROC analysis. Our findings should be considered in light of the fact that mtDNA is one of an extending number of biomarkers related to clinical outcome in patients with sepsis, and it is still yet to be identified how mtDNA compares with other serum markers. Recently, expression profiling has been applied in describing the clinical course of patients with sepsis [29,30; thus, the relative validity of serum mtDNA assessment could be questioned. It is noteworthy, though, that the measurements of serum mtDNA concentration are cheaper and convenient than expression profiling where the prognostic contribution of the transcriptional abnormalities is obvious only after an extended time of observation.
One of the interesting observations reported herein was that there were no statistical correlations between serum mtDNA DAMPs levels and WBC, CRP, as well as PCT, which may reveal that the necessary mechanisms or the original source participating in the release of mtDNA DAMPs is different from those in the inflammatory biochemical index. Thus, the assessment of plasma mtDNA DAMPs levels may help to complement CRP and PCT in the prediction of infectious complications related to post-traumatic IAIs. Different patterns of sepsis-induced host cell necrosis or apoptosis have been described during infection, which mainly relied on the specificity of pathogens, pathogen load, and location of infection. Pryroptosis, oncosis, pyronecrosis, and autophagy would contribute to the death of host cells [31. Therefore, the co-existence of several potential cell death mechanisms of mtDNA release may participate in the original source of free serum mtDNA DAMPs. Further prospective studies are needed to illuminate this relationship.
Another interesting observation in this study pertained to the positive correlation between plasma mtDNA DAMPs levels on admission and lactate concentration. Both assessments revealed significant differences from survivors to non-survivors, which probably indicated analogic mechanisms of sepsis-induced tissue hypoxia on apoptotic or necrotic cell death. Previous studies have reported that acute and prolonged exposures to hypoxia are known to independently increase oxidative stress [32–34, and the mechanisms underlying this hypoxia-related reactive oxidative stress excess production include decreased mitochondria redox potential [33. Recently, Balliet et al. [35 reported that mitochondrial oxidative stress in cancer-associated fibroblasts drives lactate production, promoting tumor growth.
As mentioned before, oxidant stress is considered an important pathophysiologic component of trauma and infections. Oxidative stress can result in the loss of damaged mtDNA molecules leading to mtDNA “degradation,” for which the understanding of degraded DNA remains largely unknown. Although the mechanisms underlying cell death in sepsis and MODS remain elusive, imbalance between oxygen delivery and consumption resulting in anaerobic glycolysis and lactate production are central features of severe infection.
This present study exhibits an interim analysis of the association between mtDNA concentration and clinical outcome of patients with IAIs induced by severe trauma. Even in such a small cohort, we found that serum levels of four selected primers, corresponding to mtDNA-encoded human cytochrome B, MT-ND2, COX1 and D-Loop transcriptional regulatory region, were increased in patients with IAIs with sepsis and MODS compared with those patients without these syndromes. We also found that serum mtDNA DAMPs levels have high effectiveness (all AUC >0.8) in predicting death secondary to MODS for these four mtDNA sequences.
This study was the first to demonstrate the relationship between plasma circulating mtDNA DAMPs and adverse outcome in patients with IAIs with severe abdominal trauma. In addition, it has been reported that severe trauma induces massive accidental necrosis of cells and surrounding tissues, which is probably accompanied by a passive release of mtDNA DAMPs into the blood circulation [26. Our results were thus also in support of the viewpoint that mitochondrial DAMPs can propagate injury from the site of trauma and infection to distant organ injury that resembles the multiple organ failure by blood circulation in severely injured patients.
Although the present study revealed that an increased serum mtDNA DAMPs levels were related to infectious complication of post-traumatic IAIs, our study still has limitations. First, the number of patients enrolled in this present preliminary study was limited, specifically in the sepsis and MODS subgroup. Second, we only collected blood samples for plasma mtDNA assessment in patients with IAIs within two days after admission, and we should assess the plasma mtDNA concentration for an extended period to review the dynamic changes of mtDNA. Therefore, further large-scale prospective studies with a greater number of patients are necessary for a better understanding of the clinical significance of plasma mtDNA in patients with IAIs induced by severe abdominal trauma.
Conclusions
These finding comprise the first evidence that serum plasma mtDNA levels are associated with the evolution of sepsis and MODS in patients with IAIs caused by severe abdominal trauma. In addition, the plasma mtDNA for selected four sequences on admission has strong power to distinguish between survivors and non-survivors among patients with IAIs. Further large-scale prospective studies with more patients are required, however, to demonstrate the reliability and reproducibility of plasma mtDNA in predicting clinical outcome for post-traumatic patients with IAIs.
Footnotes
Acknowledgment
This study was supported by grants from National Natural Science Foundation of China (81571881 and 81602103), Natural Science Foundation of Jiangsu Province (BK20160114), and Jie-shou Li Gut Barrier Foundation (S. Liu).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.