
Abstract
Abstract
Background:
Intra-abdominal infections represent a subgroup of septic syndromes with high death rates and the need for prompt and appropriate antimicrobial therapy. Conventional culture-based microbial identification has notable shortcomings in the diagnostics of polymicrobial infections. Modern culture-independent molecular methods may represent a new diagnostic approach. The current study aimed to compare the results obtained from the denaturing high-performance liquid chromatography WAVE® system as a culture-independent diagnostic tool with those obtained from standard culture-based microbiologic testing in the clinical setting of severe intra-abdominal sepsis.
Patients and Methods:
The study included 42 samples of pathologic intra-abdominal fluids, collected from 37 patients with intra-abdominal sepsis. Micro-organisms grown in culture and detected by the WAVE system were compared. Further, we recorded clinical data including baseline characteristics and the use of antibiotic agents.
Results:
In 38.1% of the analyzed samples, the classic, culture-based methods showed no bacterial growth on agar plates, in comparison with the microbiomic analysis in which the proportion of samples with negative signal was 31%. In about 40% of the patients, both methods detected one microbiologic agent, whereas in approximately one quarter of the samples, two or more agents were identified. The detection rate of certain bacteria such as Enterobacteriacae or Enterococcus faecium was significantly higher using the microbiomic analysis. Bacteria such as Haemophilus, Lactobacillus, Clostridium, Methylobacterium, Collinsella aerofaciens, and Solobacterium moorei were detected exclusively using microbiomic analysis.
Conclusion:
The culture independent molecular WAVE system provided additional information, especially concerning unusual, fastidious bacteria in patients with intra-abdominal infections. Further, it has a higher detection rate for polymicrobial infection and delivers results much sooner than conventional microbiologic methods.
E
Initially developed from the premises that large groups of micro-organisms in many environments cannot be cultured, the technique focuses on detecting 16S ribosomal ribonucleic acid (rRNA) encoding genomic sequences, which are conserved and specific within bacterial species. Early studies provided data that in natural environments only 1% of bacterial species are cultivable [1]. Applied to human microbial communities, microbiomic sequencing has so far provided valuable results in phylogenetic studies [5,6]. As a diagnostic tool, dHPLC has proven to reveal microbial diversity that often eludes conventional diagnostic methods [7]. Results can be obtained in approximately 6–24 hours, whereas traditional culture-based diagnosis often takes at least 48–72 hours to provide a result [2,3,8–10]. Therefore, this temporal advantage is of high clinical relevance when dealing with patients with sepsis by allowing an early adjustment of the antibiotic treatment [11].
Adequate antimicrobial therapy leads to significant reduction in deaths and is an essential part of sepsis management [12–15]. A delay in initiating adequate anti-infective treatment in patients with sepsis leads to an increase in death of up to 30% [16,17]. In cases of sepsis-induced hypotension, the survival rate of patients drops about 5% to 10% within every hour of delayed administration of an adequate anti-infective treatment [17]. Therefore, current international guidelines recommend that empiric intravenous antibiotic agents should be administered within the first hour after the clinical diagnosis of severe sepsis and septic shock, although studies revealed that this goal is difficult to achieve in everyday medicine [18,19].
When choosing an empiric antibiotic scheme, the site of infection as well as individual risk factors of the patient with sepsis are important variables. In any case, the initial anti-infective therapy will imply a broad-spectrum antibiotic or in the case of life-threatening infections, a combination of broad-spectrum antibiotic agents [20,21].
Another aspect to be considered is obtaining appropriate microbiologic samples before the first antibiotic dose is administered, because this could lead to rapid sterilization of the specimens and therefore limit conventional microbiologic diagnostic [18]. In case systemic spread of the causative organism is suspected, at least two sets of blood cultures have to be attained [18,19]. Once the source of infection has been localized by radiographic imaging, obtaining samples from these sites should also be sought (e.g., abscesses, fluid collections, ascites). Nevertheless, obtaining microbiologic samples should not delay the initiation of antibiotic therapy [18].
When the source of sepsis is situated in the abdominal cavity, microbial identification is based mostly on the specimen collected from the infection site during initial operation for source control [22,23]. According to current international guidelines for the diagnosis and management of complicated intra-abdominal infections, blood cultures do not provide additional clinically relevant information, except in determining the duration of antibiotic therapy [18]. Therefore, microbiologic evaluation should rely on cultures from the site of infection.
Further microbiologic diagnostic evaluation can be performed on drainage fluids or on samples collected during revision surgical procedures. This allows the detection of changes in the bacterial spectrum or bacterial antibiotic resistance with consequent adjustment of antibiotic therapy. Evaluating the relevance of microbial detection from these intra-abdominal fluid samples and determining whether it reflects a bacterial contamination, colonization, or an actual infection is again decisive for the conduct of adequate anti-infective therapy.
Patients with intra-abdominal sepsis usually present with peritonitis, which implies almost exclusively a polymicrobial infection, often involving a fungal component, usually Candida spp. [21,24]. The detection of Candida in a primarily sterile part of the organism is defined as a fungal infection, despite lacking proof of invasive fungal growth.
Certain bacteria that are normal constituents of the intestinal microbiota, such as Enterobacteriaceae and Enterococcus, are known to cause intra-abdominal infections and are usually identified using culture-based methods. In contrast, anaerobic bacteria, such as Bacteroides spp., Clostridium, or Fusobacterium, die very quickly after collection, and the isolation requires specific environmental growth conditions on standard culture plates. These particular bacterial species are, however, relevant in polymicrobial peritonitis and in the secondary formation of intra-abdominal abscess [21].
Exactly in these areas of constraint to conventional microbiologic diagnostics (identification of polymicrobial infections and difficult to culture pathogens as well as providing rapid diagnostic results), the application of new molecular techniques has proven useful, with an overall higher sensitivity level in microbial identification [11]. Nevertheless, these methods have so far only been evaluated in small studies. Thus, their clinical value is yet to be determined. The current study aimed to compare the results obtained from dHPLC using the WAVE® system (Transgenomic, Omaha, NE) as a culture-independent diagnostic tool with those obtained from standard culture-based microbiologic testing in the clinical setting of severe intra-abdominal sepsis.
Patients and Methods
This observational clinical study was performed in the surgical intensive care unit (ICU) of the University Hospital, Giessen, Germany, after approval by the local ethics committee (Ethics Committee of the Medical Faculty of the Justus-Liebig-University Giessen: Trial code 111/09). Informed consent was obtained from all patients or legal representative. Within two years, 37 patients with severe sepsis or septic shock triggered by an intra-abdominal infection were enrolled in this study. In addition, each patient was treated by abdominal operation or radiologic drainage placement. Severe sepsis or septic shock was defined according to the guidelines of the Surviving Sepsis Campaign [18]. Exclusion criteria were defined as age <18 or >80 years or pregnancy.
Fluid samples of ascites or purulent intra-abdominal material were obtained exclusively during surgical or radiologic therapeutic intervention.
Baseline parameters including patients' gender, age, height, weight, underlying clinical conditions, laboratory values, and intra-abdominal findings (e.g. Mannheim peritonitis score) were recorded. The severity of illness within the first 24 hours after admittance to the intensive care unit was calculated using the Acute Physiology and Chronic Health Evaluation II (APACHE II) score and the rate of organ failure using the Sequential Organ Failure Assessment (SOFA) scoring system. We also included antibiotic therapy, length of hospital stay, length of ICU stay, and hospital deaths.
Patients' treatment was performed according to internal guidelines and the actual guidelines of the Surviving Sepsis Campaign [18]. Adjustments to the antibiotic therapy were based on the results of the antibiotic sensitivity testing of the conventional microbiologic diagnostic.
Culture-based diagnostic methods
Culture-based diagnostic was performed at the Institute of Medical Microbiology, Justus-Liebig-University, Giessen, Germany. Collected specimens were streaked on MacConkey, blood, chocolate, Schaedler, and Sabouraud agar plates. The agar plates were incubated at 37°C and 5% CO2 for two days except for Schaedler and Sabouraud agar plates, which were incubated for two weeks. Bacteria grown on agar plates were identified by using Maldi-TOF MS (matrix-assisted laser desorption ionization time of flight mass spectrometry) as described [25]. Results were obtained from the local patient data management system.
Microbiomic analysis
The bacterial deoxyribonucleic acid (DNA) from the collected intra-abdominal specimens was isolated with an alkaline extraction method and with the use of Qiagen-Kits (QIAGEN, Hilden, Germany). A broad-range polymerase chain reaction (PCR) was performed from bacterial 16S rDNA using the forward primer 0933F and the reverse primer 1407R as follows: 5 mcL of template containing 50–100 ng of extracted chromosomal DNA and 95 mcL of a master mix containing 20 pmol of the forward primer 0933F and the reverse primer 1407R, 30 mM KCl, 10 mM Tris-HCl, pH 8.3, 2.5 mcg bovine serum albumin, 1.5 mM MgCl2, 0.4 mM deoxynucleoside triphosphates, and 1.5 units of AmpliTaq DNA polymerase were mixed for the partial amplification of the 16S rRNA and downstream WAVE system analysis.
The PCR products were analyzed using HPLC gradients for the separation of mixed amplicons with the WAVE 3500 DNA fragment analysis system (Transgenomic). DNA sequences of the 16S rRNA were aligned with the Clustal method from MegAlign (DNAStar Inc., Madison, WI). The obtained nucleic acid sequences were analyzed with the algorithm Blastn at the National Center for Biotechnology Information (www.ncbi.nlm.nih.gov/) and the GOLD genomes online database (wit.integratedgenomics.com /GOLD/) from Integrated Genomics.
Statistical data analysis
The collected data were recorded and processed using SPSS Statistics (Version 16-19, SPSS Inc., IBM), and SAS (Version 9.1, SAS Institute Inc.). Data were analyzed using mean and standard deviation or values and percentages, if appropriate.
Results
Study population
In total, the study included 42 samples of pathologic intra-abdominal fluids, collected from 37 patients. Demographic characteristics of the patients included in the study, as well as markers depicting acute infection are shown in Table 1. The calculated median age for our patient group was 60.4 ± 15.5 years. The study included 23 (62.2%) male subjects. The patients with sepsis with intra-abdominal infections had a calculated mortality rate of 40% equivalent to a median APACHE II score of 21.6 ± 6.2. This was also reflected by significant organ dysfunction, depicted by a median SOFA score of 6.24 ± 1.54. The severity of peritonitis calculated using the Mannheim score was of 24.57 ± 8.87. The mortality rate in the studied cohort was 27%.
COPD = chronic obstructive pulmonary disease; CRP = C-reactive protein; ICU = intensive care unit.
Values shown as numbers (%) or mean ± standard deviation.
Administered antibiotic therapy
At the time the samples were collected, 81% of the patients had already received an anti-infective therapy. When considering the performed adjustments to the antibiotic regimen before sampling, this fraction rises to 95.2%. Almost one third of these patients received a combined antibiotic treatment, whereas 14.3% also had an antifungal agent included in the therapeutic scheme. According to the results of the microbiologic investigations, the empiric antibiotic therapy proved to be inadequate in 12, whereas the adjusted antibiotic therapy was improper in three of the investigated cases. The empiric and adjusted antifungal therapy failed to cover the necessary spectrum in 8, respectively 4 of the investigated cases. Before time of sampling 8 cases failed to cover the necessary spectrum. After sampling 4 cases failed to cover the necessary spectrum. The anti-infective agents administered before and after microbiologic sampling are depicted in Table 2.
Values shown as numbers (%)
Microbiologic evaluation
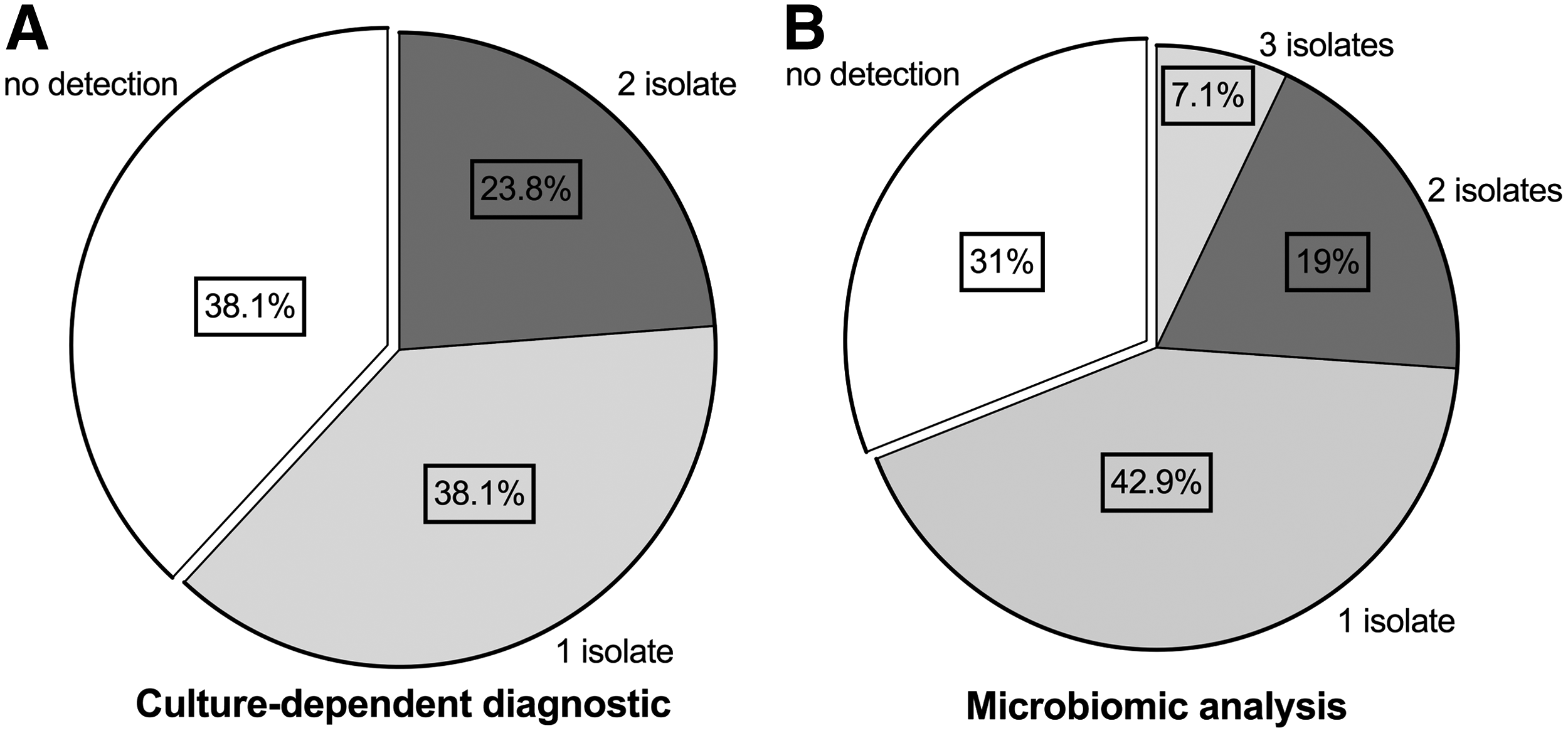
In 38.1% of the analyzed samples, the classic, culture-based methods showed no bacterial growth on agar plates, in comparison with the microbiomic analysis in which the proportion of samples with a negative PCR-signal was 31% (Fig. 1). In approximately 40% of the patients, both methods detected one microbiologic agent, whereas in approximately one quarter of the samples, two or more agents were identified. The detection rate of certain bacterial agents such as Enterobacteriacae or E. faecium was significantly higher using the microbiomic analysis. Species such as Haemophilus, Lactobacillus, Clostridium, Methylobacterium, Collinsella aerofaciens, and Solobacterium moorei were exclusively detected using microbiomic analysis.
Comparison of microbiologic isolates in culture-dependent diagnostic (
The compared methods provided coinciding results in 26.2%, and similar results in 16.7% of the analyzed samples, whereas in 7.1% of the cases, the methods generated completely different results (Table 3).
ESBL = extended spectrum beta-lactamases.
Percentage of numbers of positive bacterial (a): n = 26 or fungal (b): n = 11 detections using culture-dependent diagnostic evaluation. Percentage of numbers of positive bacterial (c): n = 29 detections using microbiomic analysis. Values shown as numbers (%).
Discussion
Sepsis is the most common cause of death among patients in the surgical ICUs. In particular, intra-abdominal infections represent a subgroup of septic syndromes with high number of deaths and the need for prompt and appropriate antimicrobial therapy. Therefore, fast and reliable microbiologic diagnostic evaluation is essential to reduce sepsis-associated deaths [17]. The current study aimed to determine the diagnostic value of dHPLC using the WAVE system as a molecular microbiologic diagnostic method in patients with sepsis with an intra-abdominal infection source. To our knowledge, this study included the largest cohort of patients with intra-abdominal infection that evaluates PCR/electrospray ionization mass spectrometry (ESI-MS) as a molecular microbiologic diagnostic method analyzing pathologic intra-abdominal fluids.
Following this approach, we examined 42 samples of pathologic intra-abdominal fluids, collected from 37 critically ill patients using both conventional culture-dependent methods and 16S rDNA PCR. The PCR-based method identified one bacterial species in 29 and two species in 11 of the investigated samples, whereas by cultivation on agar plates, the detection rate was slightly lower, with one identified bacterial species in 26 and two bacterial species in 10 of the examined samples. While culture-based methods provided a maximum of two bacterial isolates per sample, three bacterial species per sample were identified in three cases by using the WAVE system. In about one fourth of the samples, both methods showed completely coinciding results and similar results in 16.7% of the cases, while in three of the 42 examined samples, the results provided by the two methods were completely different. The clinical relevance of these little differences in our cohort remains unclear.
Because intra-abdominal infections are most often polymicrobial, it is to be expected for more than one isolate to be identified by microbiologic diagnostic evaluation [15,18]. Consistent with recent literature, fewer than half of the examined samples in the present study were positive for more than one bacterial species. This, however, is consistent with everyday clinical practice in which negative microbiologic results are not unlikely, especially under the circumstance of applied anti-infective therapy before microbiologic sampling [12]. The time to initiation of antibiotic treatment might also explain the higher microbial identification rate of the PCR-based method that, as opposed to conventional culture, can detect even residual DNA from already dead or lysed bacteria. In our study, 21.4% of all detected bacteria were exclusively detected by the WAVE system. In contrast, only 5% of all microbial detections were obtained exclusively by established culture-based diagnostic evaluation.
The lower polymicrobial detection rate of bacterial culture might also partially be because of fastidious, slow-growing bacteria that can elude or delay conventional diagnostic evaluation by requiring special environmental conditions or growing media. This proposition has already been proven valid in studies using metagenomic analysis in examining genitourinary tract infections [5,19]. In one of these studies in which the WAVE system had been applied, more than 10 bacterial species that showed no growth on agar plates were detected via the PCR-based method. Most of these species were anaerobes; others required long incubation times or selective media for cultivation, but nonetheless possessed clinical relevance as known pathogens to cause urinary tract infections [5].
In a similar manner, our study, while examining samples of patients with intra-abdominal infection, turned up six bacterial species as well as certain strains of Enterobacteriaceae solely by using the PCR-based method. These bacterial species (Haemophilus spp., Lactobacillus, Clostridium spp., Methylobacterium spp, C. aerofaciens, S. moorei) have only seldom been identified as causative micro-organisms for intra-abdominal infections. In detail, Haemophilus has been detected in our study in samples belonging to three different patients, but in the literature has been reported only in very few cases as a microbiologic isolate in patients with peritonitis, mostly related to severe cases of cholangitis or intra-abdominal infections in patients undergoing peritoneal dialysis [20–23]. On the other hand, it is well known that Haemophilus colonizes the gastrointestinal tract of children and adults [24,25]. Thus the discrepancy in the turnover rate of this bacterial species between our study and previous literature reports might suggest a lower sensitivity of culture-based methods.
In contrast, in four of our investigated samples, the WAVE system microbiomic analysis even detected Lactobacillus, which is known as a normal constituent of the intestinal flora. The relevance of isolating this bacterial strain from the peritoneal cavity thus can be disputed, because it might reflect just colonization after bowel perforation. On the other hand, a growing number of publications have reported infections varying from bacteremia to endocarditis and intra-abdominal abscess, where the main culprit has been identified as Lactobacillus spp. [26–28]. Therefore, a significant Lactobacillus infection also cannot be excluded.
When regarding the major constituents of the bacterial spectrum in our study, differences to key pathogens involved in bacterial peritonitis as reported by literature reviews also occur. The microbial strains that are most often known to be involved in community acquired intra-abdominal infections are coliforms (Enterobacteriaceae, especially Escherichia coli) and anaerobes (especially B. fragilis). Health-care–associated or nosocomial peritonitis, on the other hand, involves more resistant microbial species such as the nonfermenting gram-negative Pseudomonas aeruginosa and Acinetobacter species, extended spectrum β-lactamase–producing Klebsiella and E. coli, Enterobacter species, Proteus spp., methicillin-resistant Staphylococcus aureus, enterococci, and Candida spp. [5,29,30].
In our study, regardless of the methods used, either culture or PCR-based, the most often detected pathogens were enteroccocci (34.6% in culture and 37.9% using microbiomic analysis), Enterobacteriaceae (23.1% in culture and 27.6% using metagenomic analysis), and Bacteroides (7.7% in culture and 3.4% using metagenomic analysis). The observed tendency is toward more resistant bacterial specimens, with a relatively low rate of detected Enterobacteriaceae in comparison with a high detection rate for E. faecium, which reflects clearly the high percentage of patients with nosocomial peritonitis included in the study (75.7%) as well as the high rate of antibiotic therapy applied before microbiologic sampling (81%). Our findings are in line with the results from several studies that evaluated different PCR/ESI-MS systems during bloodstream infections, pneumonia, and sterile site infections [8,26–28].
Besides the higher bacterial detection rate, albeit a previous antibiotic treatment, another essential benefit that microbiomic analysis provides is a timely result deliverance that might prove crucial in the context of treating a patient with sepsis [10,11]. As mentioned, an inadequate antimicrobial therapy leads to a significant increase in sepsis-associated death. In our study, we found an inadequate anti-infective regimen in 22 (52.4%) patients who had been escalated to a broader-spectrum antibiotic after microbiologic examination of the intra-abdominal samples. Adapting antibiotic treatment is usually performed based on antibiotic resistance testing generated during bacterial culture. Our findings are in line with the results obtained from alternative PCR/ESI-MS systems. Also studies performed with the IRIDICA PCR/ESI-MS system (Abbott Molecular, Des Plaines, IL) demonstrated reliable results in the diagnosis of bloodstream infections, pneumonia, and sterile site infections [26,29–32].
Therefore, the lack of information about antibiotic resistance represents the major disadvantages of microbiomic analysis, because it cannot provide additional information regarding bacterial sensitivity to antibiotic agents. Therefore, the knowledge of regional resistance patterns of specific bacterial strains to antibiotics is needed, and, according to the results of conventional methods, clinical physicians should interpret the results regarding clinical symptoms. Another relevant question that cannot be clarified when using microbiomic analysis is whether the detection of bacterial strains signifies a contamination, colonization, or true infection.
This study has several limitations. First, our study included only a small group of patients, but to our knowledge, it is still the largest cohort of patients with intra-abdominal infection that evaluates dHPLC as a molecular microbiologic diagnostic method analyzing pathologic intra-abdominal fluids. Second, dHPLC can only provide antimicrobial susceptibility information about currently identified resistance genes. Therefore, conventional culture-based methods are needed currently to supply additional information. Third, our recent study does not provide any information about the impact of this approach on clinical and economic outcomes. Further studies are needed to investigate the impact of molecular microbiologic diagnostic evaluation on clinical outcome parameters.
Conclusion
Using the WAVE system to analyze samples originating from patients with sepsis with an intra-abdominal infection source does provide additional information, especially concerning unusual, fastidious bacteria. Further, it has a higher detection rate for polymicrobial infection and delivers results much sooner than conventional methods. Given the broad bacterial spectrum covered by empiric antibiotic regimens, most patients with community-acquired intra-abdominal infections resulting in sepsis do already receive adequate treatment. Therefore, further studies are needed to prove the clinical relevance of higher detection rates for polymicrobial infections and shorter analytic durations of culture independent microbiologic diagnostic evaluation in patients with severe intra-abdominal infections.
Footnotes
Acknowledgments
The authors thank the staff of the surgical ICU at the University Hospital of Giessen for their assistance in identifying study members, for clinical advice, and Silke-Zechel-Gran from the Institute of Medical Microbiology for excellent technical assistance.
Author Disclosure Statement
No competing financial interests exist.