
Abstract
Abstract
Background:
Temporary intra-operative portocaval shunts (TPCS) are believed to improve outcomes after cava-sparing liver transplantation. We hypothesize that decompression of the portal venous system via a TPCS reduces gut congestion, thereby decreasing bacterial translocation. Thus, we sought to clarify whether transplantation with a TPCS alters rates of post-operative infections and survival.
Patients and Methods:
Patients undergoing liver transplantation (n = 189) were stratified by usage of a TPCS and the type of intra-operative antibiotic prophylaxis. Rates of post-operative infections were analyzed using the χ2 test. The log-rank test was used to compare 120-d survival.
Results:
The analysis of patients transplanted with a TPCS and meropenem revealed increased infection rates with gut-specific pathogens (Escherichia coli, Escherichia faecalis, Escherichia faecium; p = 0.04) and equal 120-d survival in comparison with patients transplanted without a TPCS. When vancomycin was added to meropenem infection rates did not differ and patients transplanted with a TPCS had better survival in comparison with patients transplanted without a TPCS (p = 0.02). Within the TPCS group, the administration of meropenem and vancomycin was associated with improved survival in comparison with meropenem only (p = 0.03).
Conclusion:
Survival of patients may be improved by usage of a TPCS when gut-specific pathogens are covered by intra-operative antibiotic prophylaxis.
C
Until now, the underlying mechanism for the beneficial effects of a TPCS had not been resolved in clinical or experimental studies. As a mechanism, the beneficial effects of a TPCS are believed to be mediated by prevention of release of endotoxins and pro-inflammatory mediators caused by intra-operative cross-clamping and release of the portal vein [5–10]. Additionally, the decompression of the portal vein via a TPCS may alleviate gut congestion, bacterial translocation [11–13], and thus post-operative infection rates. However, as demonstrated by studies on post-transjugular portosystemic shunt (TIPSS) bacteremia [14,15], artificial portosystemic shunts may also promote gut-derived infections. Therefore, the goal of this study was to clarify whether the use of a TPCS affects rates of post-operative infections in liver transplantation.
Currently, only general guidelines on this issue exist and no specific recommendations for antibiotic prophylaxis in liver transplantation are available. In this respect, antibiotic regimens vary between different liver transplantation centers in Europe [16].
At our institution the standard intra-operative antibiotic prophylaxis was modified recently, which allows for an analysis on the impact of different intra-operative antibiotic regimens. Survival 120 d after liver transplantation was chosen to investigate potential effects of antibiotic prophylaxis and post-operative infections on mid-term outcomes. Therefore, this retrospective clinical study analyses post-operative infections and patient survival with respect to the insertion of a shunt, taking into account intra-operative antibiotic prophylaxis as a potential confounder.
Patients and Methods
Data acquisition, patient characteristics, intra-operative, and post-operative parameters
All liver transplantations at our institution between 2004 and 2011 were analyzed using the liver transplant registry of our hospital. Pediatric patients and patients receiving split-liver transplantations were excluded from this analysis.
Patients were stratified by usage of a TPCS and the type of intra-operative antibiotic prophylaxis. For overall analyses patients were assigned to the groups “TPCS” and “no TPCS”. For sub-group analyses, the groups “TPCS and meropenem,” “TPCS and meropenem plus vancomycin,” and “no TPCS” were compared.
Recipient characteristics were analyzed as follows: age, indications for liver transplantation (alcoholic liver disease, acute liver failure, viral hepatitis, autoimmune hepatitis, malign disease, others), Lab-MELD Score (Model for End-Stage Liver Disease) [17], donor-risk-index (DRI), cold ischemia time, and high urgency-transplantation (HU). Furthermore, transfusion of packed red blood cells (PRBC), vasopressor use (norepinephrine), duration of surgery, portal venous blood flow, and flow of the hepatic artery were analyzed.
After screening of all parameters available in the database a consensus meeting (M.W., S.P., and M.K.A.) was held to select parameters of interest. The following parameters were defined as primary parameters of interest: rates of infections with gram-positive, gram-negative, gut-specific pathogens (Escherichia coli, Escherichia faecium, Escherichia faecalis), and the overall infection rate within the first post-operative week. Additionally, 120-d survival was defined as a primary parameter of interest.
The following parameters were selected as secondary parameters of interest: intensive care unit (ICU) stay, international normalized ratio (INR), creatinine, bilirubin, aspartate transaminase (AST), alanine transaminase (ALT), Lab-MELD score, and dialysis at the seventh post-operative day. All analyses were performed in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement [18].
Surgical procedure
All patients underwent cava-sparing liver transplantation (i.e. piggy-back) as described previously [19,20]. The use of a TPCS was based on the transplant surgeons' assessment of the recipient's general condition and the presence of adequate portosystemic collaterals. The implantation of a TPCS was performed by all transplant surgeons following a standard operating procedure. Briefly, the femoral vein was cannulated with a 17F catheter (50 cm, CB 96535015; Medtronic Inc., Meerbusch, Germany) using the Seldinger technique. Subsequently, a 24F catheter was inserted in the portal vein by direct puncture and fixed by tourniquet ligation (35 cm, CB 66124, Medtronic Inc.). Both catheters were connected to allow portocaval blood flow following a pressure gradient from the portal vein to the inferior vena cava. No roller pumps or additional anti-coagulation are required for the establishment of this shunt (Fig. 1).
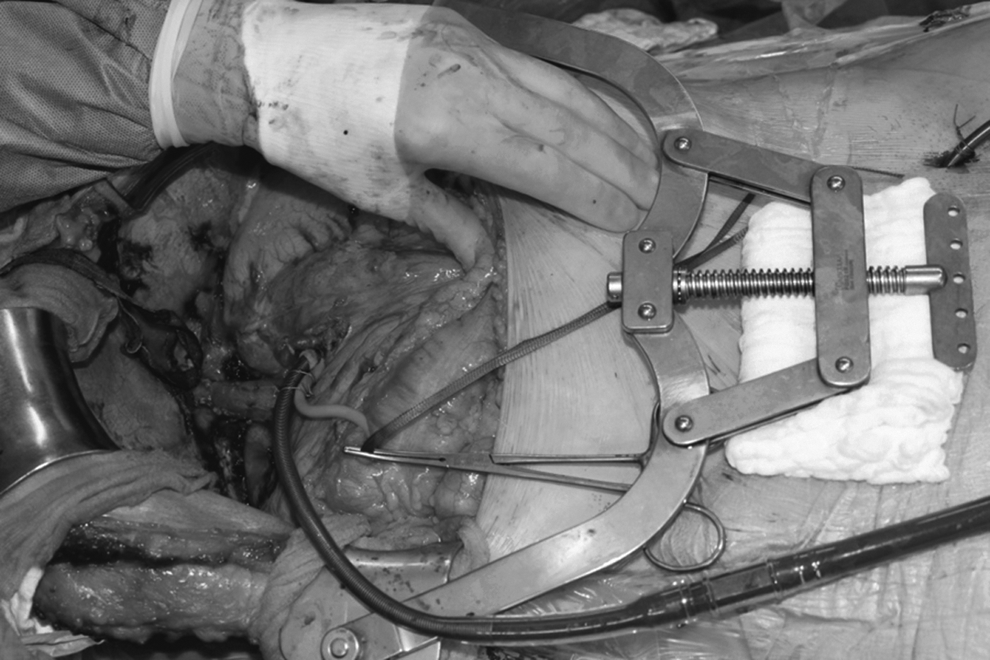
Fully established temporary intra-operative portocaval shunt (TPCS) shortly after hepatectomy.
Intra-operative antibiotic prophylaxis
From 2004 to 2007 the standard of care for antibiotic prophylaxis was the intra-operative administration of 1 g of meropenem. Since 2008 1 g of vancomycin was administered additionally.
Statistical analysis
Analyses were performed by two independent researchers (M.W. and S.P.) using GraphPad Prism version 6.00 for Windows (GraphPad Software, La Jolla, CA). For all analyses, a p value <0.05 was considered statistically significant. Categorical parameters were analyzed using the χ2 or Fisher exact test, as appropriate. Results are displayed as odds ratios (OR). Continuous parameters were analyzed using one-way analysis of variance (ANOVA) with Tukey test for multiple comparisons. Survival rates were compared using the log-rank test and results are displayed as hazard ratios (HR). For all comparisons two-sided p values are reported.
Results
Patient characteristics
One hundred eighty-nine patients were included in the analysis of post-operative infections (TPCS and meropenem: n = 17; TPCS and meropenem plus vancomycin: n = 64; no TPCS: n = 108). Patient characteristics did not show statistically significant differences between the groups with respect to median age, Lab-MELD Score, and the rate of HU-transplantations (Table 1). The analysis on indications for liver transplantation did not reveal statistically significant differences for any of the categories (alcoholic liver disease, acute liver failure, viral hepatitis, autoimmune disease, malignant disease, etc.). Furthermore, cold ischemia time was not different between all sub-groups.
A = TPCS and meropenem plus vancomycin (n = 64); B = TPCS and meropenem (n = 17); C = No TPCS (n = 108).
TPCS = temporary intra-operative portocaval shunts; DRI = donor-risk-index; HU = high urgency; MELD = Model for End-Stage Liver Disease; PRBC = packed red blood cells (PRBC).
Intra-operative parameters
No statistically significant differences were evident between the three sub-groups with respect to transfusion of PRBCs, norepinephrine use, and portal venous and hepatic arterial blood flow. The length of surgery was significantly shorter in the no TPCS group in comparison to the TPCS and meropenem group. Additionally, the overall time of surgery (301 min; interquartile range: 260–360 min) did not correlate with the incidence of post-operative infections (p = 0.11; Table 1).
Intensive care unit stay
The comparison of all sub-groups did not reveal statistically significant differences with respect to ICU stay (Table 2).
A = TPCS and meropenem plus vancomycin (n = 64); B = TPCS and meropenem (n = 17); C = No TPCS (n = 108).
ICU = intensive care unit; INR = international normalized ratio; AST = aspartate transaminase; ALT = alanine transaminase; MELD = model for end-stage liver disease (MELD); TPCS = temporary intra-operative portocaval shunts.
Post-operative course: Liver and kidney function
The comparison of the three subgroups did not reveal statistically significant differences of creatinine, bilirubin, AST, ALT, and dialysis at the seventh post-operative day (Table 2). Patients transplanted with a TPCS and meropenem plus vancomycin displayed lower INR values than patients transplanted without a TPCS (1.14 versus 1.27; p = 0.003). Statistically significant differences were not evident when patients transplanted with a TPCS and meropenem were compared with patients transplanted without a TPCS (1.35 versus 1.27; p = 0.72). Additionally, INR values of the TPCS and meropenem plus vancomycin group did not show statistically significant differences from INR values of the TPCS and meropenem group (1.14 versus 1.35; p = 0.10). No statistically significant differences were evident between all sub-groups with respect to the post-operative MELD score at the seventh post-operative day.
Post-operative infections: TPCS versus no TPCS
The overall analysis did not show statistically significant differences with respect to the overall infection rate (OR: 1.06; p = 0.85), infections with gut-specific pathogens (OR: 1.87; p = 0.16), gram-positive (OR: 1.06; p = 0.88), and gram-negative infections (OR: 0.88; p = 0.85) within the first post-operative week (Table 3 and Fig. 2).

Post-operative infections after liver transplantation with stratification by temporary intra-operative portocaval shunt (TPCS) usage and antibiotic prophylaxis.
As measured by log-rank testing.
A = TPCS and meropenem plus vancomycin (n = 64); B = TPCS and meropenem (n = 17); C = No TPCS (n = 108).
TPCS = temporary intra-operative portocaval shunts; OR = odds ratio; HR = hazard ratio; CI = confidence interval.
Post-operative infections: TPCS and meropenem versus no TPCS
Statistically significant differences were not evident with respect to the overall infection rate (OR: 2.11; p = 0.15) and gram-negative infections (OR: 0.45; p = 0.32). Patients that were assigned to the TPCS and meropenem group displayed significantly more infections with gut-specific pathogens than patients transplanted without a TPCS (OR: 4.08; p = 0.02; Table 3 and Fig. 2). Additionally, a trend toward more infections with gram-positive pathogens in the TPCS and meropenem group was found (OR: 2.59; p = 0.07).
(
Post-operative infections: TPCS and meropenem plus vancomycin versus no TPCS
The TPCS and meropenem plus vancomycin group did not display statistically significant differences from the no TPCS group with respect to overall infection rate (OR: 1.52; p = 0.20) and infections with gram-positive (OR: 0.77; p = 0.51), gram-negative (OR: 1.13; p = 0.85), and gut-specific pathogens (OR: 1.40; p = 0.50; Table 3 and Fig. 2).
Post-operative infections: TPCS and meropenem plus vancomycin versus TPCS and meropenem
The overall infection rate (OR: 0.72; p = 0.55) and infections with gram-negative pathogens (OR: 2.60; p = 0.29) did not show statistically significant differences. Furthermore, a significantly reduced incidence of infections with gram-positive pathogens (OR: 0.30; p = 0.03) and a trend towards a reduced incidence of infections with gut-specific pathogens (OR: 0.34; p = 0.09) was evident in the TPCS and meropenem plus vancomycin group (Table 3 and Fig. 2).
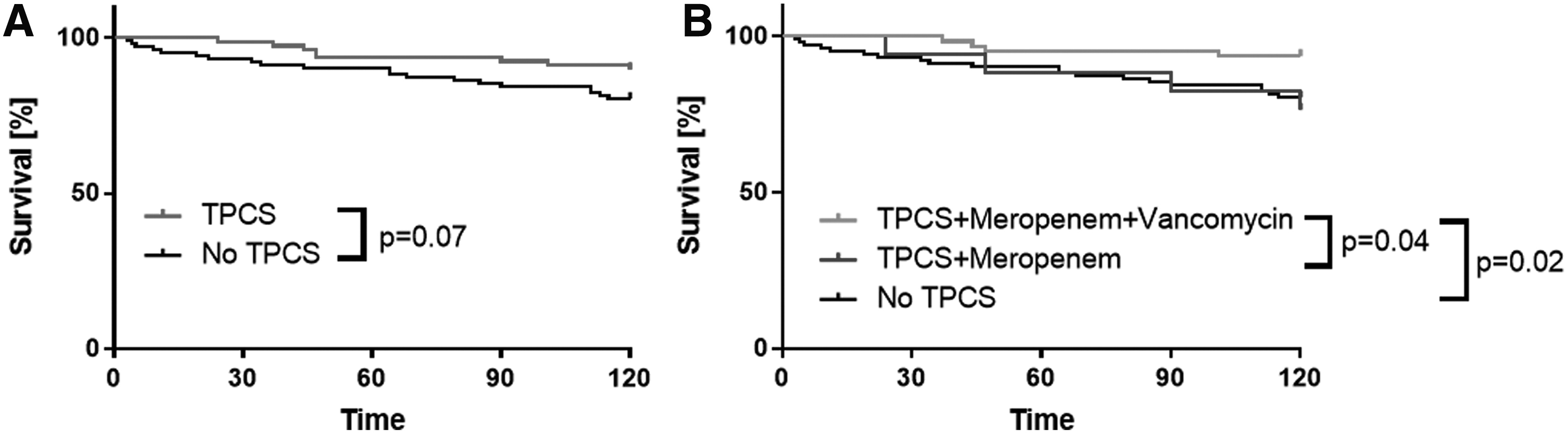
One-hundred–day survival
The overall analysis (TPCS versus no TPCS) did not reveal statistically significant differences (Table 3 and Fig. 2). However, a trend toward improved survival in the TPCS group was seen (HR: 0.48; p = 0.07). Median survival time could not be estimated because of the low number of deaths. Comparison of the TPCS and meropenem plus vancomycin and the no TPCS group revealed an improved survival in the TPCS and meropenem plus vancomycin group (HR: 0.30; p = 0.02). No statistically significant differences were evident between the TPCS and meropenem and the no TPCS group (HR: 1.18; p = 0.76). Additionally, 120-day survival was significantly improved in the TPCS and meropenem plus vancomycin group in comparison to the TPCS and meropenem group (HR: 0.25; p = 0.04).
Causes of death were stratified by death from infection/infection-induced multi-organ failure (MOF) and other causes of death. In the TPCS and meropenem group, two of four; in the TPCS and meropenem plus vancomycin group, three of four; and in the no TPCS group, eight of 20 patients died from infection/infection-induced MOF. Statistically significant differences were not detected (p = 0.43).
Discussion
In cava-sparing liver transplantation, the use of a TPCS has been shown to reduce venous stasis and blood loss [2,4,21,22] and to ameliorate post-operative kidney function [4,21] as well as ischemia-reperfusion injury [3]. As a central mechanism of a TPCS, decompression of the splanchnic circulation is believed to reduce gut congestion and bacterial translocation [13]. Therefore, the hypothesis of this study was that usage of a TPCS results in reduced rates of post-operative infections. Furthermore, 120-d survival was analyzed to investigate the effects of this technique and different forms of intra-operative antibiotic prophylaxis on patient outcomes.
The effects of the intra-operative clamping of the portal vein, however, and its decompression via a TPCS on post-operative infections are discussed controversially. In this respect, an intra-operative TPCS may bypass the hepatic antimicrobial barrier [5] thereby releasing pathogens into the systemic circulation and allowing blood from the portal venous system to bypass the liver sinusoids and Kupffer cells, which play a key role in the clearance of bacteria from the blood circulation [23]. In the present analysis, this could explain why patients treated with a shunt and meropenem only show increased rates of post-operative infections. These results are consistent with data on infections in patients receiving a TIPSS. After the insertion of a TIPSS, up to 35% of patients show bacteremia from mainly gut-derived pathogens [14,15]. Accordingly, these results suggest that TPCS usage increases the risk of gut-derived post-operative infections.
The increased incidence of infections with gut-derived pathogens in the TPCS group raises the questions whether patients would benefit from peri-operative bowel decontamination. It must be stated that current guidelines do not recommend such a treatment, which therefore is not performed at our institution. Furthermore, the results of the present study suggest that a potential survival benefit of a TPCS may be dependent on intra-operative antibiotic prophylaxis. Patients transplanted with a TPCS and meropenem plus vancomycin showed improved survival in comparison with patients transplanted with a TPCS and meropenem only and patients transplanted without a TPCS. These findings are confirmed by the fact that the incidence of post-operative infections was not increased when patients transplanted with a TPCS received meropenem and vancomycin. Furthermore, the beneficial effects of additional vancomycin in the TPCS group demonstrate the influence of a TPCS on bacterial translocation. By contrast, the no TPCS and meropenem plus vancomycin group did not have an improved survival in comparison to the no TPCS and meropenem group (p > 0.05). Interestingly, the analysis of causes of death did not reveal an increased mortality caused by infection or infection-induced MOF. This may be the result of small absolute numbers of patients but could also suggest further mechanisms triggered by post-operative infections that were not captured in the present data. One might also speculate that pre-operative colonization with methicillin-resistant Staphylococcus aureus (MRSA) plays a role in mediating the beneficial effect of additional vancomycin. However, pre-transplant MRSA screening is not mandatory in Germany, which is why MRSA colonization could not be accounted for.
In the present study, survival rates were analyzed revealing differences only in certain sub-groups with respect to the insertion of a shunt. In contrast, a previous study by Pratschke et al. [3] demonstrated an improved survival of all patients operated on with a TPCS, which was especially pronounced in recipients of marginal liver grafts with a DRI ≥1.25. In this respect, it must be stated that the populations analyzed in both studies overlap [3] but are not identical. For the current study, data on post-operative infections were available for a shorter period of time and thus patient numbers were lower.
To exclude a potential bias within this retrospective study, potential confounders have been taken into account. Interestingly, none of the pre-, intra-, or post-operative characteristics show relevant differences between the three investigated sub-groups. Especially the post-operative MELD score did not show differences between the sub-groups. This finding indicates that a TPCS does not affect liver function immediately after transplantation, but rather mid-term and long-term tissue injury. Furthermore, the results on post-operative infections indicate that the survival benefit generated by a TPCS is not based on a reduction of post-operative infectious complications. Because none of the parameters in the phase shortly after transplantation shows a relevant difference between the groups, we hypothesize that mechanisms triggered by acute phase bacterial translocation that were not captured by clinical monitoring are responsible for the effects seen in mid-term survival. One may speculate that use of a TPCS affects important post-transplant immunologic mechanisms, such as formation of de novo donor-specific human leukocyte antigen (HLA) antibodies [24].
In the present patient collective, the indication for usage of a TPCS was not standardized, which represents an obvious limitation of this retrospective study. Furthermore, potential changes of the general pathogen spectrum at our institution cannot be ruled out. In this respect, a randomized trial is required to determine the effects of a TPCS. Moreover, the post-operative antibiotic treatment could not be accounted for, because post-operative antibiotic treatment was not standardized.
Despite these limitations the results of the present study indicate that use of a TPCS may alter the spectrum of post-operative infections and thus requires an adapted intra-operative antibiotic prophylaxis. Furthermore, mid-term survival (120 d) may be associated with the type of intra-operative antibiotic prophylaxis when using a TPCS in cava-sparing liver transplantation.
Conclusion
A TPCS improves survival after cava sparing liver transplantation. This effect, however, is attenuated when infections with gut-derived infections are not considered. Thus, an antibiotic prophylaxis covering gut-specific pathogens is needed so that a TPCS can be fully effective. Prospective trials are required to clarify the effects of a TPCS in cava-sparing liver transplantation.
Footnotes
Acknowledgments
The authors contributed as follows. Study conception and design: M. Weniger, J. Andrassy, B. Grabein, M. Rentsch, A. Bazhin, J.G. D'Haese, W. Hartwig, J. Werner, M. Guba, S. Pratschke, M.K. Angele; acquisition of data: M. Weniger, T. Weig, C. Siebers; analysis and interpretation of data: Analysis and interpretation of data: M. Weniger, A. Crispin, S. Pratschke, M.K. Angele; drafting of manuscript: M. Weniger; critical revision of the manuscript: Critical revision of the manuscript: A. Crispin, T. Weig, C. Siebers, J. Andrassy, B. Grabein, M. Rentsch, A. Bazhin, J.G. D'Haese, W. Hartwig, J. Werner, M. Guba, S. Pratschke, M.K. Angel. S. Pratschke and M.K. Angele contributed equally to the manuscript. All authors read and approved the submitted version of the manuscript.
Author Disclosure Statement
No competing financial interests exist.