
Abstract
Abstract
Background:
Nosocomial infections are the main adverse events during health care delivery. Hand hygiene is the fundamental strategy for the prevention of nosocomial infections. Microbial characteristics of nosocomial infections in the Asia–Pacific region have not been investigated fully. Correlation between the use of hand hygiene products and the incidence of nosocomial infections is still unknown. This study investigates the microbial characteristics of nosocomial infections in the Asia-Pacific region and analyzes the association between the utilization of hand hygiene products and the incidence of nosocomial infections.
Patients and Methods:
A total of 78,344 patients were recruited from a major tertiary hospital in China. Microbial characteristics of major types of nosocomial infections were described. The association between the utilization of hand hygiene products and the incidence of nosocomial infections was analyzed using correlation and regression models.
Results:
The overall incidence of nosocomial infections was 3.04%, in which the incidence of surgical site infection was 1%. Multi-drug resistance was found in 22.8% of all pathogens, in which multi-drug–resistant Acinetobacter baumannii and methicillin-resistant Staphylococcus aureus were 56.6% and 54.9%, respectively. The utilization of hand hygiene products (including hand sanitizer, soap and paper towel) was associated negatively with the incidence of surgical site infection in surgical departments and the incidence of nosocomial infections in non-intensive care unit (ICU) departments (especially in surgical departments). Regression analysis further identified that higher utilization of hand hygiene products correlated with decreased incidence of major types of nosocomial infections.
Conclusions:
Multi-drug–resistant organisms are emerging in Asia–Pacific health care facilities. Utilization of hand hygiene products is associated with the incidence of nosocomial infections.
N
Hand hygiene is the basic strategy for preventing HAI, because the hands of health care workers and hospital visitors are considered the most common vehicle for the spread of pathogens within the health care environment [5]. Hand hygiene products, including hand sanitizer and soap, are recommended and have been widely adopted for hand antisepsis in health care facilities. We hypothesize that the utilization of these hand hygiene products is associated with the occurrence of HAI.
In this study, we recruited patients hospital-wide from a major tertiary hospital in China during a one-year period, describe the incidence and microbial characteristics of all types of nosocomial infections, with emphasis on the profile and resource of multi-drug–resistant organisms (MDROs) in HAI. We investigated the association between the utilization of hand hygiene products and the incidence of HAI (especially SSI) using correlation and regression analysis models.
Patients and Methods
Nanjing Drum Tower Hospital is a tertiary general hospital located in southeastern China. This hospital has approximately 2,500 beds and receives patients from all over the country. All microbiologic data on hospitalized patients is under the surveillance of the Hospital-Infection Control Office (HICO) at the hospital. The HICO also receives reports from clinicians for suspicious health care-associated infections even when microbial evidence may be absent. The diagnosis of HAI (including SSI) is based on clinical symptoms, signs, and microbiologic evidence.
There are two types of hand antisepsis available for all health care workers and hospital visitors in our hospital. The first is hand sanitizer, which is an alcohol-containing (70% alcohol by weight) agent that does not require exogenous water (waterless). After applying such sanitizer, hands are rubbed together until dry. The second is soap and paper towels. Soap used in our hospital refers to detergents that contains antimicrobial agents and requires exogenous water. Sterilized disposable paper towels are provided.
Hand sanitizer is available at the patient's bedside, nurse's station, doctor's office, transfusion trolley, and in the corridors. Soap and paper towels are distributed at the nurse's station and doctor's office. Use of hand sanitizer for hand antisepsis before and after contact with patients or relevant environment and items, before performing aseptic procedure, and removing gloves is encouraged. Soap and paper towels are recommended when hands are visibly dirty with patients' blood or body fluids. Data on the utilization of these hand hygiene products of each department are collected by HICO as well.
All patients admitted into our hospital between January 2015 and December 2015 were entered into this study. The post-operative follow-up period was 30 d. The incisions of patients with short post-operative hospitalization (less than 30 d) and inadequate evidence of SSI before discharge would be evaluated at their follow-up visits or by telephone. The exclusion criteria were: patients from the Department of Emergency and Department of Infectious Disease because they exhibit heterogeneous clinical and microbial features and patients with incomplete incisional follow-up data (30 d after surgical procedures). Patients from nine surgical departments, nine medical departments, and one intensive care unit (ICU) were recruited into this study. Microbiologic data on all enrolled patients and the utilization of hand hygiene products of each department was collected from the HICO database for analysis.
The definition [4] and classification [6,7] of SSI is in accordance with previous literature. The definition of HAIs could be found in previous articles as well [8]. Multi-drug–resistant organisms are defined as micro-organisms that are resistant to more than one antimicrobial agent [9]. Five types of MDROs are under real-time surveillance in our hospital, including multi-drug–resistant Acinetobacter baumannii (MDR-AB), multi-drug–resistant Pseudomonas aeruginosa (MDR-PA), carbapenems-resistant Enterobacterium (CRE), including Escherichia coli and Klebsiella pneumoniae, vancomycin-resistant Enterococcus (VRE), including Enterococcus faecium and Enterococcus faecalis, and methicillin-resistant Staphylococcus aureus (MRSA).
Statistical analysis
All statistical tests were performed with SPSS software (SPSS for Windows, version 13.0, SPSS, Chicago, IL). All analyses were two-tailed and differences were considered statistically significant when p values <0.05. Spearman correlation analysis was performed to investigate the association between SSI/HAI rate and utilization of hand hygiene products. Correlation illustrations are generated by GraphPad Prism (version 5.01, GraphPad, San Diego, CA). Multiple linear regression analysis with forward stepwise methods was performed to analyze the correlation between the utilization of hand sanitizer and soap and paper towel use with the incidence of SSI or HAI. This study was approved by the Medical Ethics Committee of Nanjing Drum Towel Hospital, the Affiliated Hospital of Nanjing University Medical School.
Results
Surgical site infection
Between January 2015 and December 2015, 84,458 patients were admitted into our hospital. A total of 2,093 patients from the Department of Emergency and Department of Infectious Disease were excluded and 4,021 patients with incomplete follow-up data were also excluded. The remaining 78,344 patients including 46,589 patients (59.5%) from surgical departments, 31,290 patients (39.9%) from medical departments, and 465 patients (0.60%) from ICUs qualified for inclusion (Fig. 1).

Flow chart of participants in current study. A total of 80,437 patients were admitted to our hospital during 2015. After excluding 2,093 patients from the Department of Emergency and the Department of Infectious Disease, 78,344 patients qualified for inclusion. Among them, 31,920 patients were from departments of medicine, 465 patients were from intensive care units (ICUs), and the other 46,589 patients were from departments of surgery. Of the 46589 surgical patients, 16,937 patients received conservative therapy (without surgery) and the other 29,652 patients underwent surgical procedures, including 26,063 patients with single operation and 3,589 patients with re-operations.
A total of 30,678 surgical procedures were performed. The overall incidence of SSI was 1% (307/30,678), which varied from departments and types of incisions. Specifically, general surgery exhibited the highest incidence of SSI (2.14%), followed by gynecology and obstetrics (1.94%). Incidence of SSI in the other surgical departments was lower than 1% (Table 1).
HAI = hospital-acquired infection; SSIs = surgical site infections.
Table 2 compares the incidence of three types of SSI in different types of incisions. Notably, deep incisional SSI occurred most frequently in contaminated incisions. Figure 2 illustrates the fluctuation of SSI incidence of each month. Autumn (July to September) exhibited higher incidence of SSI, whereas winter (October to December) exhibited lower incidence of SSI.

Incidence and type of surgical site infections (SSIs) in each month for 2015. A total number of 307 SSIs happened in 30,678 surgeries. Different types of SSI including superficial, deep incisional, and organ/space infection (gray bar) were calculated in each month. The corresponding SSI rate (♦) for each month was demonstrated as well.
SSI = surgical site infections.
Positive microbial evidence was obtained in 204 of the 307 cases, resulting in a positive culture rate of 66.4%. The most common pathogens of SSI were Escherichia coli (35.8%), Staphylococcus aureus (13.2%), Enterococcus faecalis (7.84%), Pseudomonas aeruginosa (5.89%), and Klebsiella pneumonia (4.9%; Table 3). Drug resistance was detected in 27 of 204 species, resulting in a drug-resistant rate of 13.2% in SSI (Table 3).
Others include Citrobacter freudii, Candida albicans, Proteus mirabilis, Morganella morganii, Staphylococcus epidermidis, Streptococcus hemolyticus, Candida glabrata, Enterobacter aerogenes, Brinell lemon bacillus.
Hospital-acquired infections
A total of 2,384 HAIs were observed in 78,344 hospitalized patients within the whole year. The overall incidence of HAI was 3.04%. Specifically, the HAI incidence was the highest in ICUs (28.0%), whereas it was moderate in surgical departments (3.67%), and lowest in medical departments (1.74%; Table 1).
The most common types of HAI were respiratory tract infection (1,122 events; 47.1%), urinary tract infection (377 events; 15.8%), blood stream infection (375 events; 15.7%), SSI (307 events; 12.9%), and gastrointestinal tract infection (81 events; 3.4%).
The overall MDR incidence was 22.8% (1,091/4,784). Specifically, MDR-AB was 56.6%; MRSA, 54.9%; MDR-PA, 12.3%; CRE, 2.76%; and VRE, 2.43% (Table 4). The most common sources of MDROs were sputum (58.9%), incisional discharge (11.0%), urine (7.98%), blood (6.97%), catheter tip (including both central venous catheter and urethral catheter) (5.96%), and feces (2.02%; Table 5).
CRE includes carbapenems-resistant Escherichia coli and Klebsiella pneumonia.
VRE includes vancomycin-resistant Enterococcus faecium and Enterococcus faecalis.
MDROs = multidrug-resistant organisms.
The catheter tip includes both central venous catheter tip and urethral catheter tip.
Utilization of hand hygiene products correlates with the incidence of HAI
The utilization of hand hygiene products was the highest in ICUs (Table 1). Figure 3 illustrates a negative correlation between SSI incidence of surgical patients and the utilization of either hand sanitizer (r = −0.85, p = 0.0061), soap (r = −0.88, p = 0.0031) or paper towels (r = −0.83, p = 0.0083). Nevertheless, no statistical association of hand hygiene products utilization and HAI incidence was found in enrolled patients (Table 6). Sub-group analysis revealed significant negative correlation in non-ICU patients (r = −0.52 to −0.65, p = 0.0032–0.029). The correlation became more significant in patients from departments of surgery (r = −0.75 to −0.90, p = 0.0020 ∼ 0.026; Fig. 4).
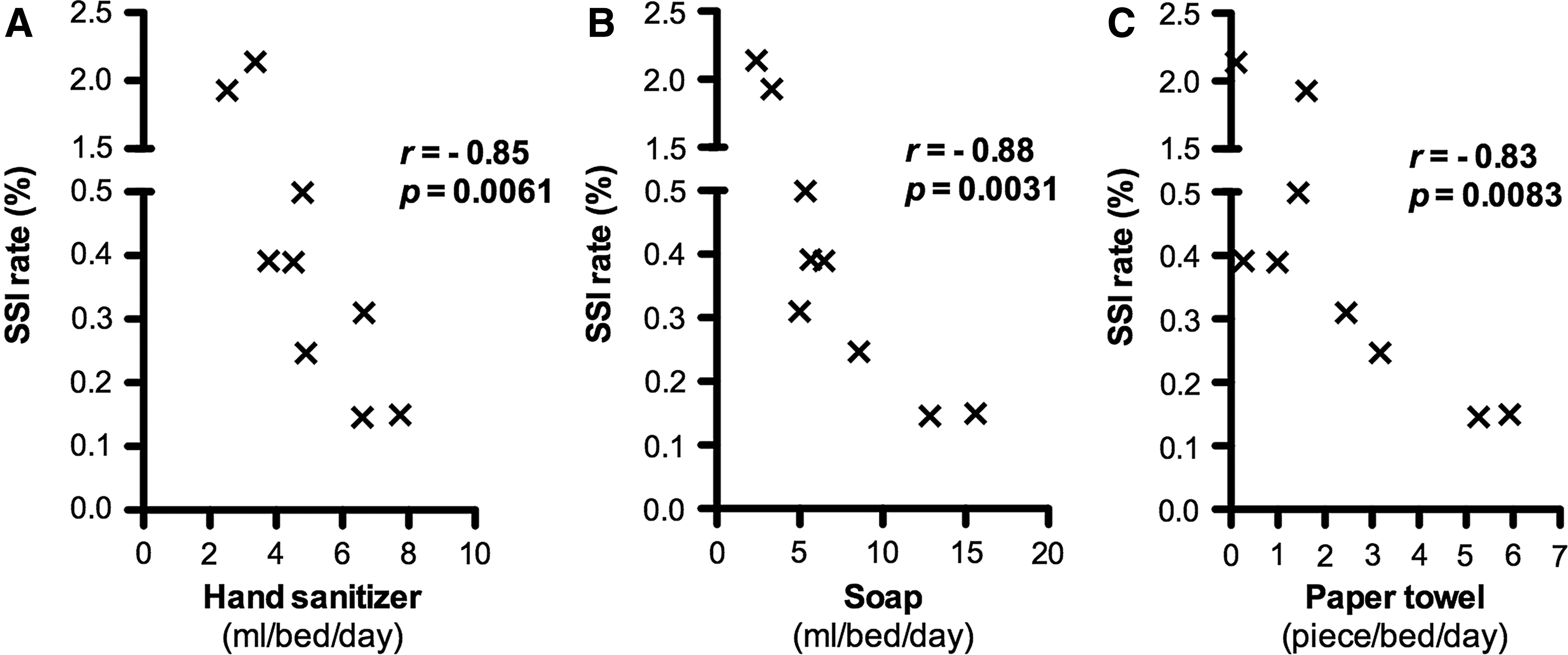
Correlation between the incidence of surgical site infections (SSIs) and utilization of hand hygiene products. Spearman correlation analysis was performed in 46,589 patients from nine surgical departments. R value and p value represented correlation coefficient and statistical significance, respectively. Negative correlation was revealed between SSI rate and utilization of hand sanitizer (
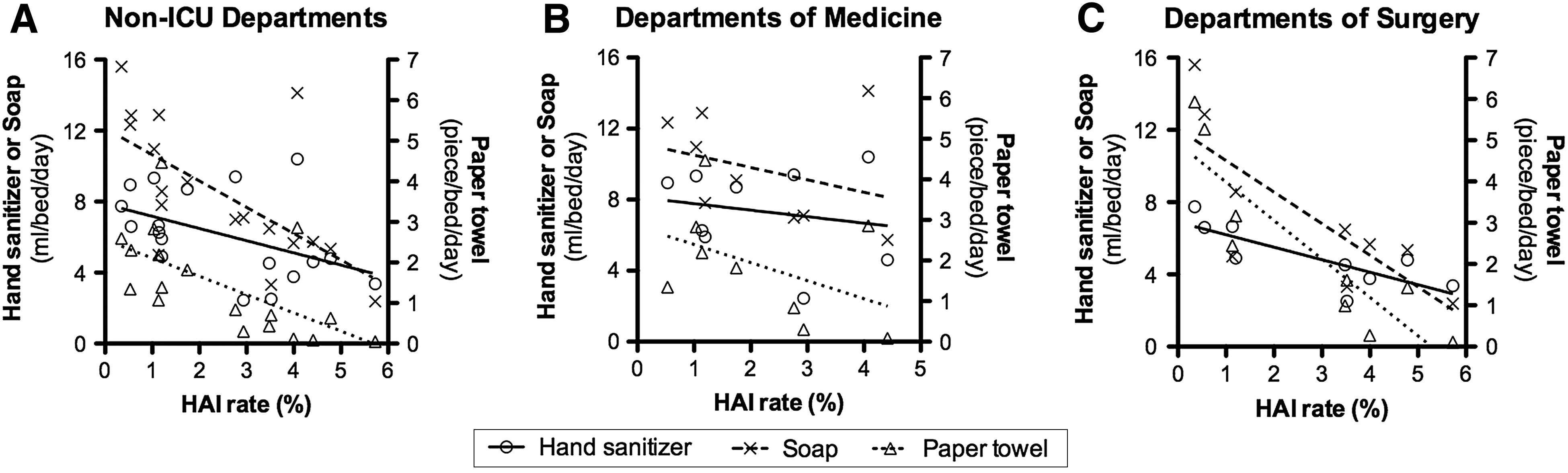
Correlation between the incidence of nosocomial infection and the utilization of hand hygiene products. Spearman correlation analysis was performed in 78,344 patients from nine departments of surgery, nine departments of medicine, and one intensive care unit (ICU). R value and p value represented correlation coefficient and statistical significance, respectively. Correlation was not significant in patients from all departments (data was not shown). Further analysis found significant correlation in non-ICU departments including both surgical and medical departments (
Values in bold indicate statistical significance.
Subsequent regression analysis identified that higher utilization of hand sanitizer correlated with lower SSI incidence (B = −0.33, 95% confidence interval [CI]: −0.06 to −0.61, p = 0.023), higher utilization of soap correlated with decreased HAI incidence in non-ICU patients (B = −0.28, 95% CI: −0.11 to −0.46, p = 0.004), and higher utilization of paper towels correlated with decreased HAI incidence in surgical patients (B = −0.84, 95% CI: −0.45 to −1.24, p = 0.001; Table 7).
SSI = surgical site infections; HAI = hospital-acquired infection; ICU = intensive care unit.
Discussion
According to a large meta-analysis [10], the overall incidence of SSI in mainland China is 4.5%. The incidence fluctuates between 2% and 9.7% in Korean health care facilities [11] whereas it is estimated to be 2.8% in the United States [12]. Meanwhile, the incidence of SSI continues to be reported with great variability globally. Inconsistent classification and definition as well as an increase in post-discharge identification of incisional infection are partially responsible for this variation [13]. Previous reports have found a high incidence of SSI in patients receiving emergency surgery. For instance, the SSI rate was 32.1% reported by Watanabe et al. [14] and 36.5% reported by Ruth et al. [15] in emergency colorectal surgery. Notably, patients from the Department of Emergency and the Department of Infectious Disease have been excluded from this study. We assume that the exclusion of emergency surgery contributed to the relatively low incidence of SSI in our study.
Since the 1980s, shifts in the microbial etiology of nosocomial infections have been occurring worldwide [16–18]. Drug-resistant pathogens with fewer therapeutic options stress the importance of microbial surveillance [19]. Current knowledge of the characteristics of MDROs in HAIs and associated clinical outcomes is based overwhelmingly on reports from industrial countries. Although recent studies have reported that drug resistance is emerging in developing countries as well [20,21], epidemiology and microbial profiles of MDROs in developing countries are still scare. Our data could contribute to a global insight into the current status of MDROs in hospital facilities.
The antimicrobial ability of alcohol is attributed to the ability to denature proteins of pathogens, of which the recommended concentration of alcohol ranges between 60% and 95% [22,23]. Previous studies have demonstrated the in vivo and in vitro antiseptic ablility of alcohol and its effectiveness in preventing the spread of health care-associated pathogens [24,25]. Nevertheless, alcohol is not appropriate in certain scenarios, e.g., when hands are visibly dirty or contaminated with proteinaceous materials [26–29]. Therefore, both alcohol-based hand sanitizer and antiseptic soap (plus disposable paper towels) are provided for hand hygiene in our hospital. However, selection of hand hygiene products varies between hospitals because of diverse local habits and dispenser systems, and the superiority of different hand antiseptic methods remains in debate according to recent studies [30–32]. In our hospital, the recommendation of hand hygiene methods is in accordance with the WHO guideline [2], i.e., antiseptic soap is preferred when hands are visibly dirty whereas waterless sanitizer is recommended when not visibly dirty. In the current study, we found that the utilization of sanitizer and soap was independently associated with the incidence of nosocomial infections.
A nosocomial surveillance system is responsible for monitoring the incidence of HAI and provides evidence for the control of hospital infections. Quick and assertive responses to health care-associated infections improves health care quality and reduces social and financial burdens [13], however, few strategies are available currently to predict the prevalence of HAI. Our data demonstrated that the utilization of hand hygiene products correlated with the incidence of HAI, and suggested that the utilization should be monitored by the nosocomial surveillance system.
We are aware of the limitations of this study. First, this is a single-center study (although with large sample size), resulting in possible selection bias. Second, in addition to the utilization of hand hygiene products, there are potential confounders (e.g., waste of products, pre-operative/intra-operative protocols) in the correlation analysis. Before the release of new WHO recommendations for SSI prevention in 2016 [33,34], the NICE Guideline for prevention and treatment of SSI [35] had been implemented in our hospital. This peri-operative protocol is recommended strongly all departments of our hospital, although we could not ensure that all peri-operative preparations in different patients were performed consistently. Third, the incidence of SSI might be underestimated in this study because a certain number of health care workers is involved in the diagnosis of SSI. Nevertheless, most of the involved health care workers are physicians or surgeons, to whom SSI is a fundamental concept. The definition of SSI is consistent among all departments in our hospital as well.
In conclusion, this study demonstrated that MDROs are emerging in Asia–Pacific health care facilities. Utilization of hand hygiene products correlates with the incidence of nosocomial infections. Our study could assist in developing a globally feasible hand hygiene guideline. Future projects with hand hygiene research priority are expected to protect patients from microbial spread in health care facilities.
Footnotes
Acknowledgments
The authors thank the Hospital Infection Control Office at Nanjing Drum Tower Hospital for assisting with microbial data retrieval. The authors thank Dr. Daren Low (Agency for Science, Technology and Research, Singapore) for critical review and language editing of this paper.
This study was supported by a grant from the National Natural Science Foundation of China (No. 81602103), the Natural Science Foundation of Jiangsu Province (No. BK20160114), the Key Project of Medical Science and Technology Development Foundation of Nanjing Department of Health (YKK16114), the Fundamental Research Funds for the Central Universities (No. 021414380169), and the Jie-shou Li Gut Barrier Foundation (LJS-201604).
Dr. Wenxian Guan and Dr. Jianan Ren designed the work and performed critical revision of the manuscript; Dr. Song Liu, Dr. Meng Wang, Dr. Gefei Wang, and Dr. Xiuwen Wu performed the study and analyzed the data. Orginal data was provided by the Hospital Infection Control Office. Dr. Song Liu drafted the manuscript.
Author Disclosure Statement
All authors declare that there is no conflict of interest.