
Abstract
Abstract
Background:
Antibiotic-impregnated central venous catheters (CVCs) decrease the incidence of infection in high-risk patients. However, use of these catheters carries the hypothetical risk of inducing antibiotic resistance. We hypothesized that routine use of minocycline and rifampin-impregnated catheters (MR-CVC) in a single intensive care unit (ICU) would change the resistance profile for Staphylococcus aureus.
Methods:
We reviewed antibiotic susceptibilities of S. aureus isolates obtained from blood cultures in a large urban teaching hospital from 2002–2015. Resistance patterns were compared before and after implementation of MR-CVC use in the surgical ICU (SICU) in August 2006. We also compared resistance patterns of S. aureus obtained in other ICUs and in non-ICU patients, in whom MR-CVCs were not used.
Results:
Data for rifampin, oxacillin, and clindamycin were available for 9,703 cultures; tetracycline resistance data were available for 4,627 cultures. After implementation of MR-CVC use in the SICU, rifampin resistance remained unchanged, with rates the same as in other ICU and non-ICU populations (3%). After six years of use of MR-CVCs in the SICU, the rate of tetracycline resistance was unchanged in all facilities (1%–3%). The use of MR-CVCs was not associated with any change in S. aureus oxacillin-resistance rates in the SICU (66% vs. 60%). However, there was a significant decrease in S. aureus clindamycin resistance (59% vs. 34%; p < 0.05) in SICU patients.
Conclusions:
Routine use of rifampin-minocycline-impregnated CVCs in the SICU was not associated with increased resistance of S. aureus isolates to rifampin or tetracyclines.
A
A wide range of interventions have been developed to decrease CLABSI. Previous studies have demonstrated that use of a bundle including full barrier precautions, appropriate skin preparation, appropriate hand hygiene, and specific anatomic sites for placement can decrease CLABSI rates [5]. Further, administrative interventions, including multidisciplinary educational efforts and checklists, also can significantly decrease the incidence of CLABSI [6]. However, despite wide-ranging implementation of these measures, CLABSI rates remain relatively high.
Over the last 17 years, the surgical intensive care unit (SICU) at Barnes-Jewish Hospital has pursued efforts to decrease CLABSI. This hospital houses a diverse cohort of patients, including acute-care surgery and trauma patients, elective general surgical patients, patients from other surgical specialties, and overflow medicine patients. In 1999, an education program and follow-up behavioral intervention was instituted to increase compliance with known best practices, as defined by the U.S. Centers for Disease Control and Prevention (CDC) CLABSI prevention bundle [6]; these measures indeed led to a significant decrease in catheter-associated infections.
Antimicrobial-impregnated catheters are another tool that might reduce CLABSI. In 2002, routine use of central venous catheters (CVCs) impregnated with chlorhexidine and silver-sulfadiazine was initiated in the SICU and resulted in a small yet significant improvement in CLABSI rates [7]. Subsequent studies from other centers suggested that minocycline- and rifampin-impregnated catheters (MR-CVC) were superior to chlorhexidine/silver-sulfadiazine–impregnated catheters for preventing CLABSI [8]. A prospective study in our SICU documented that use of the MR-CVC was associated with a significant reduction in CLABSI [9]. Therefore, since 2006, only MR-CVC have been utilized for new central line insertions in the SICU. A recent large meta-analysis supports these findings, reporting that MR-CVC are associated with a significantly lower risk of blood stream infections compared with standard catheters, with an aggregate relative risk of 0.28 [8]. Given the high degree of scrutiny placed on CLABSI and the demonstrated benefit of antibiotic-impregnated CVCs, these catheters have become the standard of care in immunocompromised patient populations and in patients at high risk of line infections such as burn patients and those requiring prolonged central venous access.
Nonetheless, routine use of these catheters in all patients may result in increased exposure of microorganisms to these antibiotics, with the potential of developing significant resistance to rifampin or tetracyclines [10,11]. Thus far, studies investigating whether increased antibiotic resistance occurs with use of MR-CVC [12] have given heterogeneous results, although resistance to minocycline and rifampin has been demonstrated in vitro [10,11]. Because mandatory utilization of MR-CVC in the SICU at our institution began in September 2006 but not in other intensive care units (ICUs) or among non-ICU patients, it was possible to track changes in resistance within a single unit where exposure to the antibiotic impregnated-CVCs was high and compare it with other areas of the hospital where exposure was essentially non-existent. To measure the effect of MR-CVC on microbial resistance patterns, we specifically monitored Staphylococcus aureus susceptibilities; this micro-organism generally is susceptible to rifampin and tetracyclines, but this susceptibility could be altered by the selective pressure exerted by MR-CVCs.
Patients and Methods
The study protocol was approved by the Washington University Institutional Review Board. All blood cultures positive for S. aureus from January 2002 through October 2015 within a comprehensive, de-identified hospital database were selected for further evaluation. The hospital location where the blood culture was obtained was recorded, the time period in which the culture was obtained, and the antibiotic susceptibilities of the isolates were entered in a database. Data on susceptibilities to oxacillin, clindamycin, and rifampin were available throughout the study period, but data on doxycycline and tetracycline susceptibilities were available only from 2009–2015. Organisms resistant to either doxycycline or tetracycline were considered tetracycline resistant for analysis. Isolates reported as having intermediate susceptibility were coded as resistant. There were no patient identifiers available in the comprehensive database, and it was not possible to determine how many blood cultures positive for S. aureus from the same patient were included in the database. There were no changes in how blood culture results were documented in the comprehensive database throughout the study period. Catheter-associated blood stream infections were defined according to CDC-guidelines.
Positive cultures were grouped according to the year obtained and whether they were obtained before or after September 2006, the point when insertion of MR-CVCs became the standard practice in the SICU. However, SICU patients could still have other central access lines, such as hemodialysis or peripherally inserted central lines or catheters inserted at other locations, which were not MR-CVCs. In a prior study, the prevalence of MR-CVCs among all central lines in SICU patients during a portion of the study period was 44% [9].
For analysis, rifampin resistance was compared before and after August 2006. Rifampin resistance during these same time periods was characterized in other ICU patients, including those in the cardiothoracic surgical ICU, the medical ICU, the neurological ICU, and the cardiac ICU and also in non-ICU patients. Because the susceptibilities of S. aureus to tetracyclines began to be reported only in 2009, yearly trends in tetracycline resistance in the SICU and other locations were compared, but a direct comparison before and after institution of the use of MR-CVCs was not possible.
Chi-square tests were used to determine associations between aggregate resistance rates before and after implementation of MR-CVC use. Two-way analysis of variance followed by the Tukey multiple comparisons test was used to assess for differences in average annual resistance rates. A p value <0.05 was considered statistically significant. Statistical analyses were performed using SPSS version 23.0 (IBM Corp., Armonk, NY).
Results
We identified 10,483 blood cultures that were positive for S. aureus during the period queried. Susceptibility data for rifampin, oxacillin, and clindamycin were available for 9,703 of these cultures. For tetracyclines, data were available for 4,627 isolates obtained between 2009 and 2015, when testing for tetracycline susceptibility was reported. The numbers of cultures identified in the SICU, other-ICU, and non-ICU populations, as well as the distribution before and after implementation of routine insertion of MR-CVCs in the SICU in September 2006, are shown in Figure 1.
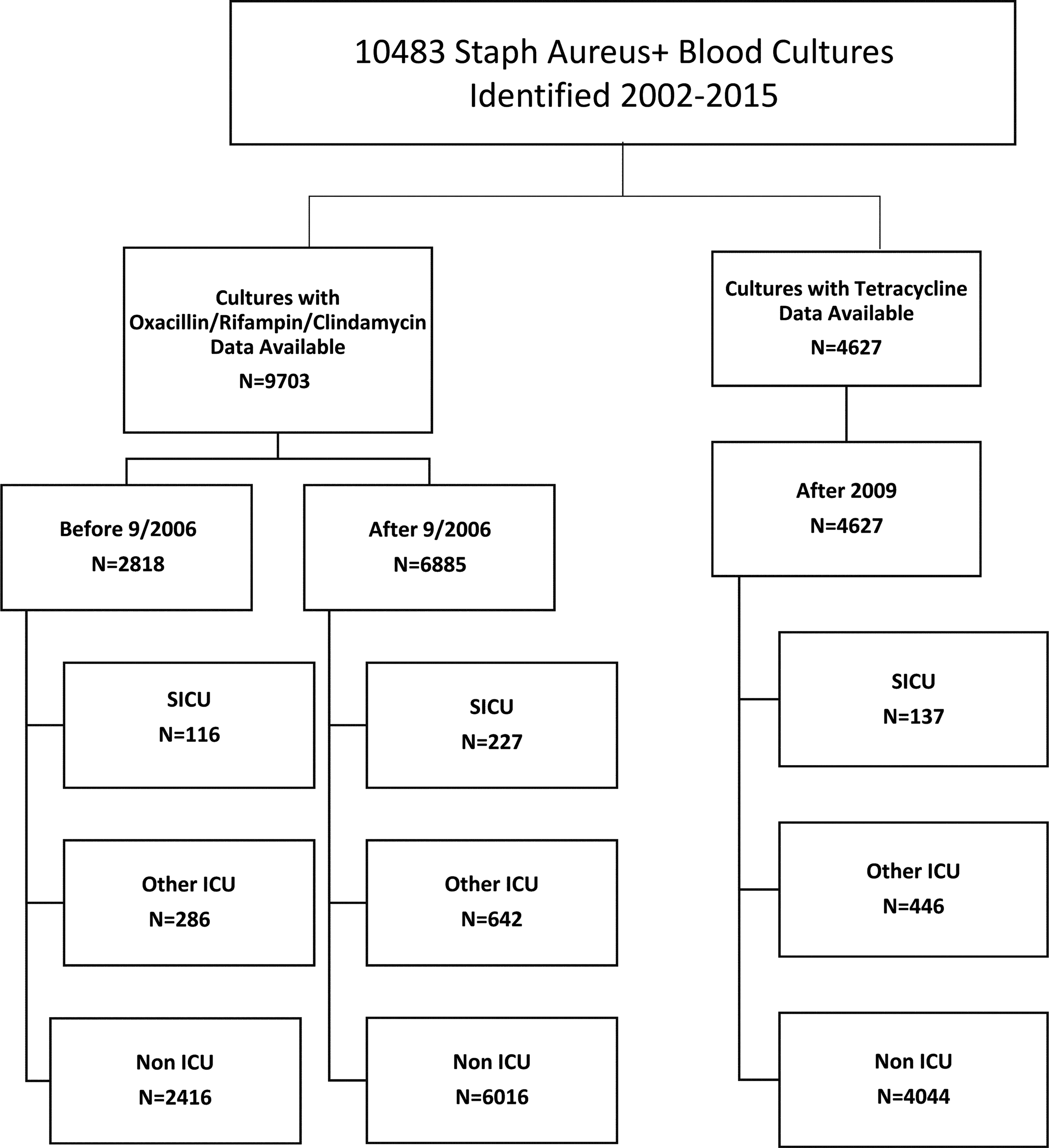
Bacteremias with microbial cultures positive for Staphylococcus aureus from January 2002–October 2015. Of these, 9,703/10,483 had complete data for oxacillin, rifampin, and clindamycin susceptibility; and 4,627 had data available for tetracyclines. After September 1, 2006, all central venous catheters used in the surgical intensive care unit were minocycline and rifampin impregnated.
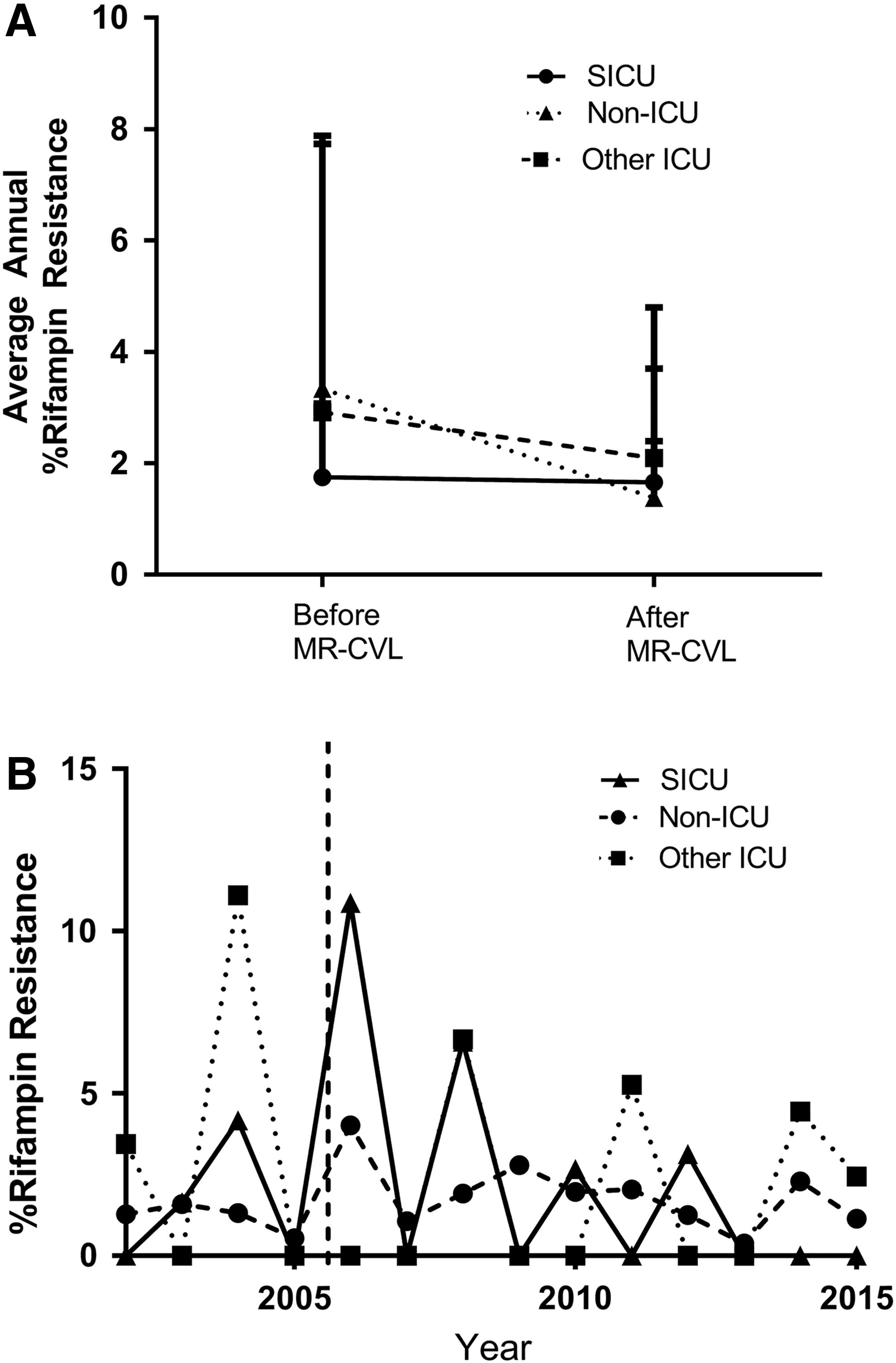
Rifampin susceptibilities were available for all S. aureus isolates obtained during the study period (Table 1; Fig. 1). In the period before MR-CVC use in the SICU, from January 2002–September 2006, 3% of S. aureus isolates in the SICU (4/116) were resistant to rifampin; in the aggregate period after implementation of universal MR-CVC use from October 2006 to October 2015, 3% (6/227) were resistant. This difference was not significant by χ2 analysis (Table 1, Fig. 2A). The annual rate of rifampin resistance among S. aureus isolates between 2002 and 2015 fluctuated within the SICU, but no trend in the yearly percentage of rifampin resistance or in the average annual rate of resistance in the SICU was identified (Fig. 2A, B). In other ICU populations, in which MR-CVC were not routinely utilized, the rate of rifampin resistance before and after September 2006 was not appreciably different from that measured in the SICU and did not change significantly between the two time periods (Table 1; Fig. 2A). As in the SICU, annual rates of rifampin resistance fluctuated somewhat, but there was no overall trend observed between 2002 and 2015 (Fig. 2B). Although resistance rates of S. aureus isolates obtained from patients in non-ICU settings appeared to be slightly lower than those obtained in either SICU or other ICU patients, this difference was not statistically significant. There also was no trend toward increased or decreased resistance throughout the study period. Overall, there were no statistically significant differences in rifampin resistance between the SICU, other ICU, and non-ICU populations, either before or after implementation of mandatory MR-CVC use in the SICU.
Rifampin resistance rates in Staphylococcus aureus isolates.
P < 0.05 by χ2 test.
MR-CVC = methicillin/rifampin-impregnated central venous catheter; SICU = surgical ICU; ICU = intensive care unit.
Data for tetracycline resistance, obtained from 2009–2015 (after implementation of routine use of MR-CVCs in the SICU in 2006) was compared in the SICU, other ICU, and non-ICU populations. Overall rates were low: 3% of isolates (5/137) from SICU patients, 1% of isolates from other ICU patients (5/446), and 3% of isolates from non-ICU patients (133/4,004) (Table 2). Annual rates of tetracycline resistance fluctuated within each population, but no trends in resistance were noted among any of the populations (Fig. 3B), and the average annual rates were not significantly different (Fig. 3A).
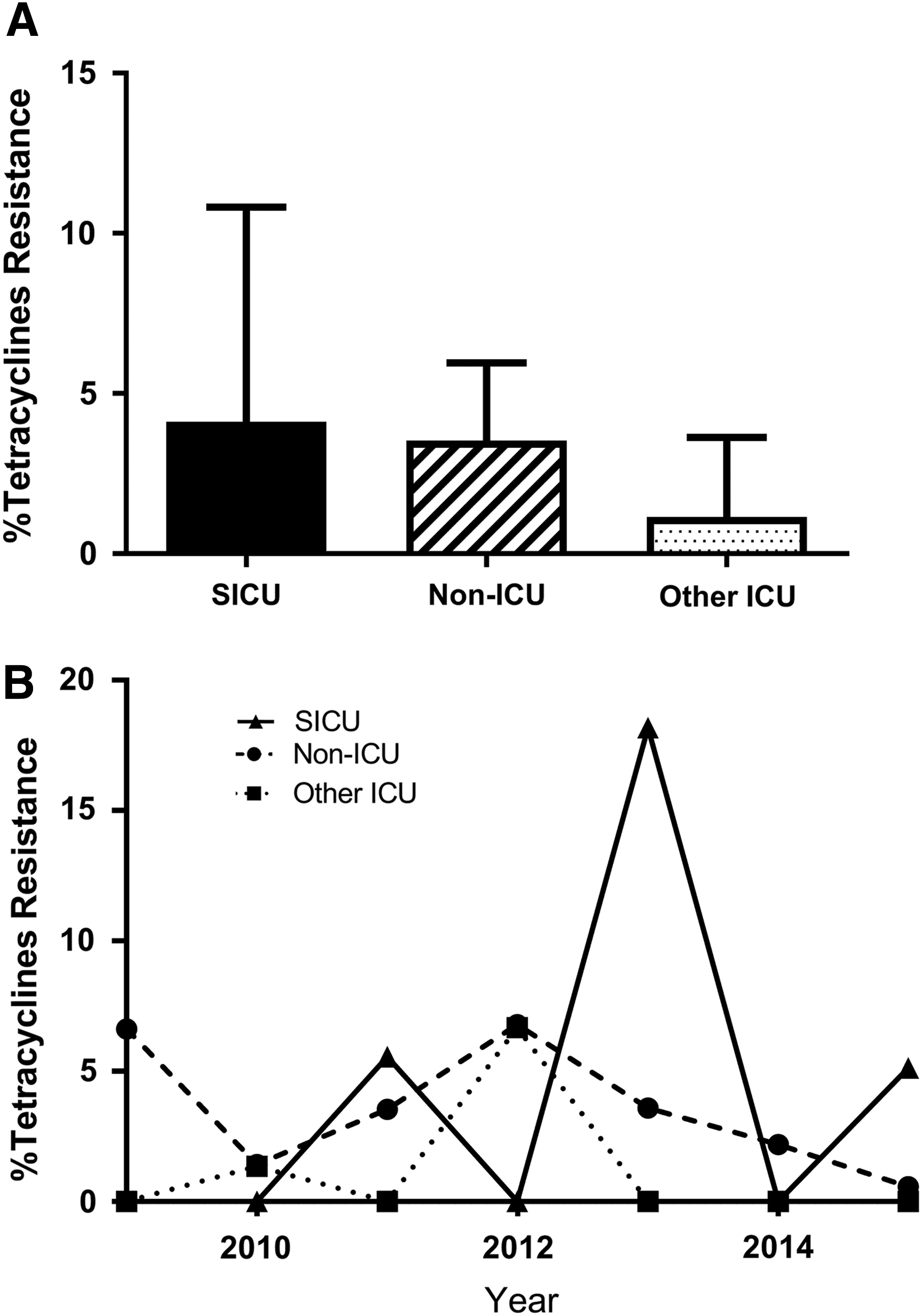
Tetracycline resistance rates in Staphylococcus aureus isolates. Doxycycline and tetracycline resistance data were pooled for the period from 2009–2015.
MR-CVC = methicillin/rifampin-impregnated central venous catheter; SICU = surgical ICU; ICU = intensive care unit.
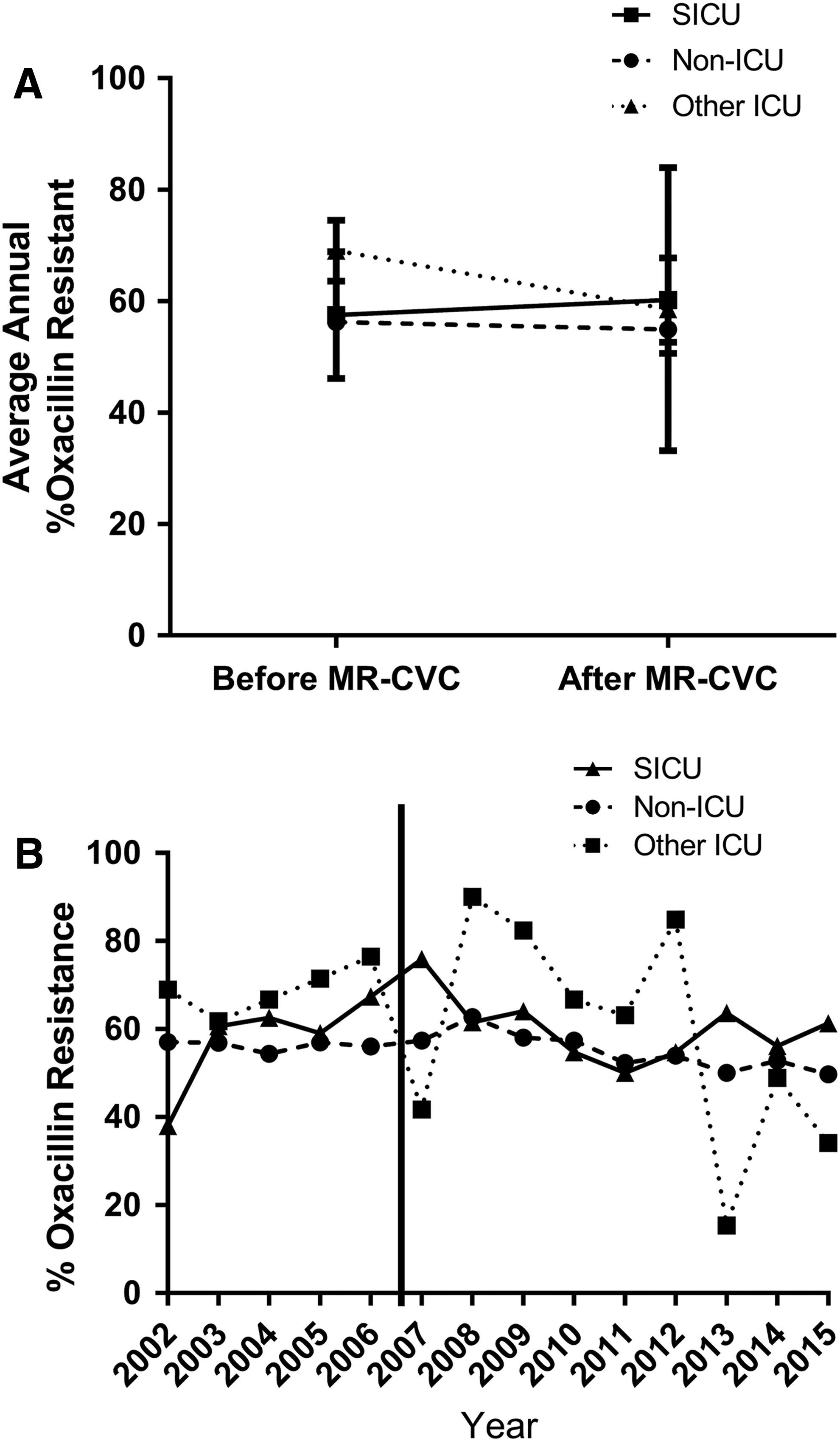
Changes in the sensitivity to oxacillin and clindamycin also were assessed, as these could reflect the relative prevalence of methicillin-resistant S. aureus (MRSA) strains in isolates obtained before and after implementation of use of MR-CVCs. Oxacillin-resistant strains were assumed to be MRSA. Among all patients, 56.8% of S. aureus isolates were MRSA strains in the period before September 2006 and 56.2% of isolates were MRSA strains after September 2006. There were no significant changes in the incidence of MRSA in the SICU, other ICU, or the non-ICU populations with initiation of routine use of MR-CVC in the SICU (Table 1; Fig. 4A). Evaluation of annual rates of oxacillin resistance demonstrated no temporal change throughout the study period (Fig. 4B).
Oxacillin resistance rates in Staphylococcus aureus isolates.
In the period prior to use of the MR-CVC, the aggregate clindamycin resistance rate in S. aureus isolates from SICU patients was higher than the rate observed in isolates from other ICU patients and from the non-ICU population, although this was statistically significant only for the comparison with the latter (Table 1; Fig. 5A). In the period after implementation of universal insertion of MR-CVCs, however, there was a significant decrease in clindamycin resistance observed in the SICU isolates compared with the pre-implementation period (59% vs. 34%; Table 1; Fig. 5A). Rates of clindamycin resistance in isolates from SICU patients were actually lower than those observed in the non-SICU populations, but this difference was statistically significant only for isolates from patients in other ICUs (Table 1; Fig. 5A). There appeared to be a trend toward decreased clindamycin resistance on an annual basis after routine use began of MR-CVCs in the SICU population (Fig. 5B), although this trend did not reach statistical significance. There was no change in clindamycin resistance observed in S. aureus isolates from patients in other ICUs before or after September 2006, but there was a parallel, although less dramatic, decrease in clindamycin resistance in isolates from non-ICU patients before and after September 2006, which did reach statistical significance (45% vs. 41%; see Table 1).

Clindamycin resistance rates in Staphylococcus aureus isolates.
To determine if our change to antibiotic-impregnated catheters was temporally associated with a change in CVC usage in the SICU, we measured the total number of catheter days from 2002–2015 in both the SICU and other-ICU populations. To determine if there were changes in catheter exposure over time, simple linear regression was calculated to predict the number of catheter days over time. A significant regression equation was found (F = 13.0; p < 0.05; R2 = 052) demonstrating that there was a statistically significant increase in CVC use in the SICU over time. There was no significant trend in the other ICU populations (F = 1.8; p = 0.2; R2 = 0.13). These data demonstrate that since the institution protocol MR-CVL use in the SICU, total line exposure in the SICU has increased, whereas there has been no change in line exposure in the other ICU populations.
We also measured the rate of CLABSI at our institution. We previously reported that MR-CVL led to a significant reduction in the CLABSI rate in our SICU [9]. We find that we have had a continued low rate of CLABSI in both our SICU and other ICU populations, with average annual rates of <2 CLABSI/1,000 line-days (Fig. 6B). Importantly, fewer than 5% of the CLABSI in our institution are caused by S. aureus, and therefore, the bacteremia results we report above are rarely CLABSI but in contrast represent non-catheter-associated primary or secondary bacteremias.

Central venous catheter line-days and central line-associated blood stream infections (CLABSI) in surgical (ICU) and other ICU populations.
Discussion
This retrospective study evaluated the antibiotic susceptibilities of all S. aureus isolates from blood cultures for four years before and nine years after initiation of mandatory use of a MR-CVC in the SICU at this institution. Use of these catheters was not associated with any notable increase in resistance to rifampin or tetracyclines. Further, resistance patterns in other ICUs and throughout the institution did not diverge significantly from those seen in the SICU, providing an internal control to verify these findings. To our knowledge, this is the longest follow-up reported to date of antibiotic resistance after initiation of MR-CVC use.
These results significantly expand on the study by Ramos et al., who also measured antibiotic sensitivities before and after introduction of MR-CVC. These authors compared the average rate of resistance in 1998, one year prior to the introduction of MR-CVC, with the average rate of resistance in 2006, seven years after the introduction. During this interval, there was intermittent use of MR-CVC until 2003, after which MR-CVC use became mandatory. Similar to our results, that study reported no increase in resistance among bacterial isolates after introduction of the MR-CVC.
Although implementation of MR-CVC was not associated with a change in susceptibility to tetracyclines or rifampin, an unexpected finding was the significant change in the susceptibility profile of S. aureus to clindamycin in isolates obtained from patients in the SICU after initiation of MR-CVC use. There was an almost 50% decrease in clindamycin resistance between 2006 and 2015. Prior to that time, clindamycin resistance rates in the SICU were significantly higher than the rates in non-ICU populations, but after the introduction of MR-CVC, clindamycin resistance rates regressed toward the mean hospital rate and then became lower. There was no significant change in clindamycin resistance in the other ICU populations and only a small decrease in the non-ICU populations, suggesting that the change occurred primarily in SICU patients.
One potential explanation for this phenomenon was that use of MR-CVCs led to selection of different S. aureus strains causing bacteremia in SICU patients or, alternatively, to an overall change in the types of S. aureus strains colonizing SICU patients. However, this change in susceptibility of S. aureus to clindamycin over time may well have been an independent phenomenon related to a shift in the incidence of S. aureus infections from the hospital-acquired USA100 MRSA strain to the community-associated USA300 MRSA strain. The USA300 strain emerged as an important pathogen during the time of this study [13]. Further, this institution is in a geographic area where there is a high degree of USA300 emergence [13]. Of note, the USA300 strain is characterized by less antibiotic resistance than the USA100 strain [14–16]. The USA300 strain generally is susceptible to clindamycin (6% resistance), whereas the USA100 strain is not (95% resistance) [17]. A remaining question, however, is why the change in S. aureus susceptibility to clindamycin was observed only in SICU patients and not in other ICU patients and only minimally in the general hospital population. It is possible that SICU patients have a much greater risk of infection with the USA300 MRSA strain because of its propensity to produce skin and soft tissue infections [14], creating a lower risk for patients in other ICUs. Nonetheless, this difference makes it difficult to conclude that an overall change in microbial ecology in the geographic area was solely responsible for this change in S. aureus susceptibility that was limited primarily to SICU patients.
Our study design has several strengths that support our conclusions. First, MR-CVCs have been inserted in the SICU for more than nine years, potentially allowing any accumulated changes in antimicrobial resistance over this long period of time to be detected. Second, because MR-CVCs have not been used routinely in other ICUs in this institution, changes in antibiotic resistance independent of MR-CVC use could have been observed. Finally, the extensive database available allowed analysis of more than 9,500 culture results, permitting detection of relatively minor changes in antibiotic resistance.
Despite these strengths, there are several limitations to this study. First, it was retrospective, thus providing only associative data and not allowing conclusions to be drawn regarding causality or mechanism. Moreover, the data are indirect, utilizing a database of culture results to link isolation of a microorganism with a specific resistance profile to the times and locations where use of MR-CVCs differed. Direct patient-linked data were not available using this study design; we are unable to correlate our resistant cultures with specific use of MR-CVCs. This will be an important issue for future studies. We did assess the number of CVC-days in the SICU vs. other ICU populations and found that the number of CVC days increased over the study period in the SICU but not in other ICU populations, demonstrating an increasing exposure of the SICU microbiome MR-CVL in the SICU over the study period. Another potential limitation is the reliance on S. aureus bacteremia data. All of these cultures are blood cultures, but we cannot determine if these are CLABSI and have no specific data regarding the relation between catheter use and bacteremia for specific patients. At our institution, S. aureus accounts for less than 5% of CLABSI; therefore, the majority of these positive cultures are bacteremia but possibly not CLABSI. As an additional limitation, we report only data for S. aureus, and resistance in other organisms isolated from different sites certainly could have been impacted by use of the MR-CVC. Prior in vitro studies have demonstrated inducible resistance to rifampin and tetracycline in both Pseudomonas aeruginosa and S. epidermidis. With regard to S. aureus susceptibilities, only qualitative data were available. Data regarding minimal inhibitory concentrations or zone of inhibitions might have made it possible to monitor more subtle quantitative changes in antimicrobial susceptibility. In addition, we report only data on S. aureus bacteremia. The study design does not allow us to assess changes in other microbial cultures, and an analysis of the resistance profile of a broader cohort of microbes, including surveillance cultures, will be an important next step. However, the absence of these data does not temper the strength of our conclusions that use of M-R catheters was not associated with any meaningful changes in resistance of blood stream isolates of S. aureus to rifampin and tetracyclines.
In addition, we cannot account specifically for other changes in practice that could alter the local microbial resistance pattern. Within the SICU, we have followed CDC best practice guidelines for CVC insertion since 2002, and no systematic changes were made to our line insertion protocol over the study period. Since 2002, there have been no specific institutional changes designed to alter resistance to rifampin or tetracyclines. We cannot exclude the possibility that interventions in infection-control practices over the study period contributed to changes in local antibiotic resistance profile, although it seems unlikely that such non-specific efforts would have altered resistance specifically to rifampin and tetracyclines. Moreover, a review of institutional hospital infection-control protocols does not demonstrate any significant, systematic institutional changes over this time period. Finally, changes in prescribing of relevant systemic antimicrobials were not evaluated. Use of systemic antibiotics might influence emerging resistance to a far greater degree than use of the MR-CVC, making any altered susceptibility difficult to detect. However, the relatively static resistance profiles (except to clindamycin) observed across all units suggest that this confounder did not have a major influence on these results.
This study does lay the groundwork for future investigations into any role that MR-CVCs play in altering microbial ecology. Such work would preferentially utilize patient-specific data to determine if the presence and duration of MR-CVCs had any association with increased resistance among microbial isolates. Such a study could overcome some of the limitations of this present study. However, it may not provide conclusive data, given the low overall incidence of bacteremia caused by any particular pathogen in ICU patients, and would be much more labor intensive.
In conclusion, despite nine years of continuous use of MR-CVCs in the SICU, generalized emergence of antimicrobial resistance of S. aureus to rifampin and tetracyclines was not observed. Of interest, use of MR-CVCs was temporally associated with a decrease in resistance of S. aureus to clindamycin, although it is unclear if this reflected overall changes in MRSA ecology or an effect of these catheters. These data do not support the hypothesis that use of MR-CVCs leads to a significant increase in antibiotic resistance. Given the benefit of these catheters in reducing CLABSI, their use in selected patients remains an appropriate option for decreasing overall rates of CLABSI.
Footnotes
Author Disclosure Statement
No competing financial interests exist for any of the authors.