
Abstract
Abstract
Background:
Abdominal cocoon formation is an uncommon manifestation of abdominal tuberculosis that is characterized by the formation of a fibrous membrane-like sac around the small intestinal loops. Appropriate treatment and outcomes are uncertain
Objectives:
To review the clinical presentation, treatment, and outcomes for tubercular abdominal cocoon (TAC).
Patients and Methods:
We included studies published in the English language and listed in EMBASE or PubMed. All case series or reports that reported patients with TAC were considered for inclusion. Details regarding demographic, clinical presentation, and treatment received were tabulated.
Results:
The clinical features included predominantly abdominal pain, abdominal distension and features of intestinal obstruction, loss of appetite, and weight loss. The diagnosis was usually established at surgery, however, computed tomography was a useful tool. In most patients the treatment reported was surgical, however, conservative therapy with anti-tubercular therapy (ATT) did succeed in a subset of patients. The published literature includes only case series and reports. The outcomes, especially long-term outcomes, have not been reported in most studies.
Conclusion:
Abdominal cocoon is an uncommon form of abdominal tuberculosis and conservative management with ATT may suffice in some patients whereas non-responsive cases require surgery.
T
Abdominal cocoon is also termed as sclerosing encapsulating peritonitis or encapsulating peritoneal sclerosis (when in chronic ambulatory peritoneal dialysis patients). This clinical condition has been described as occurring in either a primary form (idiopathic) or secondary form (related to chronic ambulatory peritoneal dialysis, malignancy, β-blockers) [5,6]. Tuberculosis is an uncommon cause of this condition and the published literature is limited to a few case series and case reports. The objective of this review is to summarize the available literature about TAC and suggest the diagnostic criteria and management approach for this entity [7–26]
Patients and Methods
Literature search
We searched PubMed with the search strategy tuberculosis OR tubercular AND abdominal cocoon OR sclerosing encapsulating peritonitis OR encapsulating peritoneal sclerosis). We also searched EMBASE with the strategy abdominal AND cocoon OR sclerosing encapsulating peritonitis OR (encapsulating AND peritoneal AND sclerosis) AND tuberculosis. Of the 47 and 37 respective results retrieved from PubMed and EMBASE, 25 were duplicates (Fig. 1). In all 59 results were considered for inclusion and eventually four case series and 16 case reports were included in the final analysis (Tables 1 and 2) [7–26]. Among these was one case report in which Mycobacterium bovis was implicated as the causative agent [26].

Selection of articles for inclusion in the present review.
Fourteen had completed follow-up.
Describes 18 cases of tubercular and non-tubercular cocoon; seven patients had received empirical ATT of whom only two had definite TB on histology after surgery.
IO = intestinal obstruction; TB = tuberculosis; CT = computed tomography; MRI = magnetic resonance imaging; NA = not available; ATT = anti-tubercular therapy.
Also on peritoneal dialysis.
Received steroids also.
Related to Mycobacterium bovis
TB = tuberculosis; OOI = other organ involvement; C = confirmed TB; P = probable TB; CT = computed tomography; MRI = magnetic resonance imaging; AFB = acid fast bacilli; IO = intestinal obstruction./
Definitions
We have considered tuberculosis as a definitive possibility in cases in which microbiological evidence in the form of acid-fast bacilli positivity on smear, culture or positivity of polymerase chain reaction using specific primers from tissue in which the presence is not otherwise expected, e.g., peritoneal biopsy or ascites or histopathologic evidence of caseating granulomas in absence of other diseases.
A case has been labeled as having presumptive (or probable) tuberculosis when the patients have all of the following:
1. Clinical and radiologic profile is consistent with tuberculosis 2. Biochemical (elevated adenosine deaminase in fluids), histologic (granulamtous inflammation), or corroboratory evidence (positive Mantoux skin test, changes on chest radiograph consistent with active or old pulmonary tuberculosis) 3. Exclusion of other differential diagnosis.
These definitions are based on the terminology used in Indian Extra-Pulmonary Tuberculosis Guidelines (INDEX-TB Guidelines) [27]. The diagnosis of abdominal cocoon was established by the demonstration of a membrane around a part or whole of small intestine as visualized on computed tomography or magnetic resonance imaging or detected on surgery. Cocoon was labeled a partial cocoon if the membrane surrounded only the small intestine whereas if the presence of large intestine or other organs inside the cocoon was detected the cocoon was labeled as complete cocoon [5]. The diagnostic strategy is depicted in Figure 2.

Suggested diagnostic criteria for tubercular abdominal cocoon (TAC). PCR = polymerase chain reaction; CT = computed tomography; MRI = magnetic resonance imaging; ADA = adenosine deaminase.
Data synthesis and analysis
We tabulated all demographic information (age, gender, place of residence), clinical presentation (pain, intestinal obstruction, lump), diagnostic methods for cocoon (imaging or surgery and tuberculosis (microbiologic, biochemical analysis of fluid, or histologic features) and the management strategy (conservative with anti-tubercular therapy [ATT] alone or surgical therapy) for each of the cases. Wherever the information was available for interpretation, we also recorded whether the cocoon was partial (including only the small bowel) or complete (small bowel and large intestinal or other organ involvement). Risk of bias was not assessed formally because the reports were all case series or case reports.
Results
Clinical and demographic profile
We included four case series and 16 case reports in the present study reporting 66 cases. However, one of the case series by Singh and Gupta [8] included both tubercular and non-TAC and did not provide separate details for the patients with TAC and was therefore excluded from summative analysis. The summative analysis, therefore, is based on 48 patients with TAC. Occasional reports also suggest multiple underlying etiologic factors that could have caused cocoon formation (e.g., tuberculosis and chronic ambulatory peritoneal dialysis) [22].
Most reports seemed to emerge from India as do all of the case series (Fig. 3, Tables 1 and 2). Only occasional cases have been reported from the Western world. Even in such cases the disease was reported in individuals who were immigrants from Asian or African countries [16,25,26]. The disease can afflict patients with any age and either gender. However, a male preponderance was apparent (64.6% of 48 cases) in most of the reports except in a case series from Kashmir, India, in which females contributed to eight of the 11 cases [9]. The clinical manifestations include abdominal pain, abdominal distension, and features of intestinal obstruction, loss of appetite and weight loss. Of the 48 cases in which the clinical details were summated, 34 (70.8%) had episode(s) of intestinal obstruction, 19 (39.6%) has loss of appetite or weight, 16 (33%) had a palpable abdominal lump, 12 (25%) had abdominal pain without intestinal obstruction whereas 13 had history of fever. One patient was reported to have presented with features of perforation peritonitis [16]. The frequency of human immunodeficiency virus (HIV) infection was not reported and no case with concurrent HIV infection could be identified in our literature search.
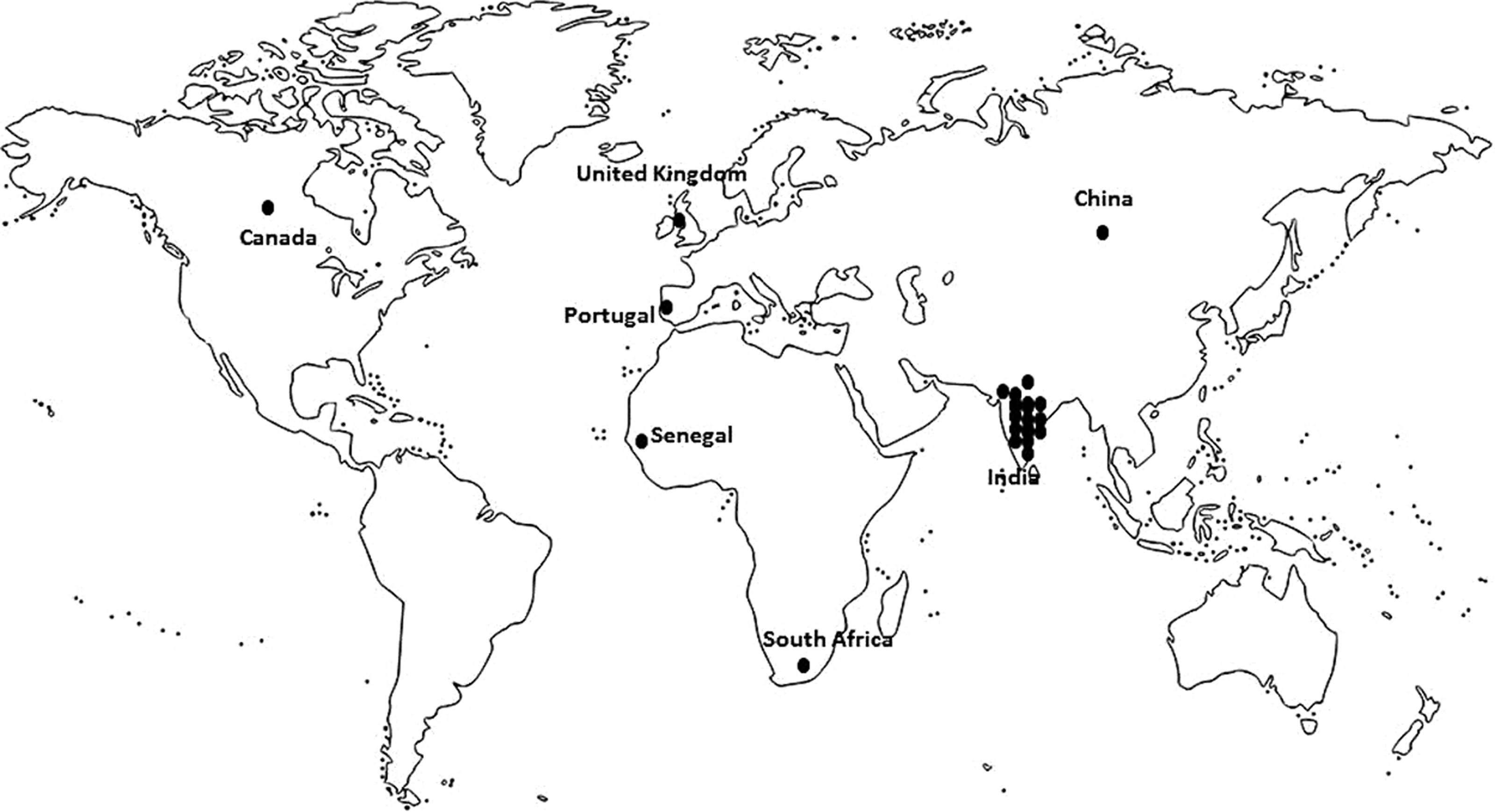
Geographic locations from which cases of tubercular cocoon have been reported.
Diagnostic evaluation
The positivity of Mantoux skin test has been reported infrequently. However, in one case series 80% of patients had a positive Mantoux skin test [7]. The use of interferon gamma release assays (IGRA) has not been reported in the published literature.
For the diagnosis of abdominal cocoon the use of computed tomography and diagnosis at time of surgery was reported in various reports. In the four case series (Table 1) only one series reported pre-surgical diagnosis using computed tomography whereas in others pre-operative diagnosis was reported infrequently [7]. In series from Srinagar, India, only one of the 11 patients had a pre-operative diagnosis made on imaging [9]. In our recent series, all except one of the 15 patients had a diagnosis on imaging [7]. Although most cases suggest a radiologic and surgical correlation, occasional cases have been reported suggesting that computed tomography may miss the cocoon on some occasions [19]. Most studies have not reported whether the underlying cocoon was partial or complete. In our series, most patients (80%) had a complete abdominal cocoon [7]. In reports by Wani et al. [9] and Kaushik et al. [10] most patients seemed to have a partial cocoon on basis of description provided.
The diagnosis of tuberculosis was based on combination of criteria. In a series by Sharma and Gupta [7] only three patients had confirmed tuberculosis, whereas all of the patients in series by Wani et al. [9] and Kaushik et al. [10] had confirmed tuberculosis. This is primarily based on the presence of caseating granulomas although the microbiologic evidence was not available. Most of the case reports that have reported the use of polymerase chain reaction have not identified the primers used.
Treatment and outcomes
Most reports have described surgical therapy for the TAC. However, some reports suggest that a conservative approach with ATT may also improve symptoms. In a case report, Jain et al. [13] described a 13-year-old male patient who improved with ATT. Similarly a 37-year-old male reported by Gomes et al. [21] improved with ATT. Also, in a series from India a majority of patients who were started on ATT showed improvement [7]. However, the course is often punctuated by recurrent episodes of intestinal obstruction and occasionally conservative therapy may fail necessitating surgery [7,21,22]. In a series of six surgical patients of TAC, apart from one death, four patients developed post-operative enterocutaneous fistulae [10]. Other surgical series, however, report excellent outcomes [8,9]. Occasional reports also describe utility of a laparoscopic approach [12]. The recurrent episodes of obstruction may warrant a long hospital stay or re-admission [26]. Unrecognized cocoon may be complicated by development of intestinal perforation [16]. Use of steroids has been reported in three patients in one series with good outcome [7].
Discussion
Tubercular abdominal cocoon is an uncommonly described variant of abdominal tuberculosis. Because the literature regarding this entity is scarce, we attempted to collate the literature to seek a diagnostic and management strategy based on the literature. The difficulty in diagnosis of abdominal tuberculosis is well known and microbiologic evidence of tuberculosis is difficult to obtain in this entity. Therefore, a response to therapy (Logan modification of Paustian criteria) is often used as one of the criteria to establish the diagnosis [2,28]. However, the appropriate definition of “response to therapy” is uncertain and a recent article suggests that mucosal (ulcer) healing is the appropriate definition for patients with intestinal tuberculosis. Even so, the patients may continue to remain symptomatic because of formation of stricture [29]. The use of these criteria in TAC is even more difficult because of the lack of any objective criteria for response. To date, no evidence suggests that the cocoon or the membrane disappears with ATT [7]. Even with ATT, the patients may continue to be symptomatic and need surgery. Furthermore, if surgery is done after a period of ATT, the pathognomonic findings of tuberculosis could have disappeared as has been noted in one series in which patients who were on ATT prior to surgery did not have evidence of tuberculosis on histology [8]. We therefore propose that TAC may be described to be either a confirmed or a clinically diagnosed case on the basis of microbiologic and histologic findings (Fig. 2). Also, the diagnosis of cocoon has been established on basis of imaging (computed tomography or magnetic resonance imaging) or surgical findings. The use of ultrasound has been described for diagnosis of cocoon but the modality is operator dependent [30]. Also, the presence of pulmonary tuberculosis (past or current) may not be apparent in all the patients. In one series of 15 patients with abdominal cocoon related to tuberculosis, only four had evidence of pulmonary infection [7]. When present, the evaluation of pulmonary lesions with sputum examination for acid-fast bacilli may help in the diagnosis in a given case. However, in a majority of cases there may be no pulmonary lesions and the clinician may encounter diagnostic difficulty in such cases.
The treatment of TAC should include effective ATT and management of episodes of intestinal obstruction. The episodes of intestinal obstruction should be managed with nasogastric aspiration, monitoring of abdominal girth, and intravenous fluids. If the situation improves, one can suggest dietary modifications and hope that inflammatory component would be addressed by the ATT. In non-responsive cases, surgical intervention with resection of membrane and adhesiolysis may be needed. All attempts should be made to avoid surgery because the surgery for this condition is associated with significant morbidity. As of now, the utility of steroids is anecdotal and cannot be recommended. However, steroids have been used in encapsulating peritoneal sclerosis observed with peritoneal dialysis and may be considered along with ATT as an option.
To conclude, abdominal cocoon formation is an uncommon clinical manifestation of abdominal tuberculosis and usually presents with abdominal pain and intestinal obstruction. The diagnosis is on basis of a combination of features: diagnosis of cocoon with imaging or surgical findings and the diagnosis of tuberculosis using clinical, radiologic, histologic, biochemical, and microbiologic findings. Once the diagnosis is established management of intestinal obstruction and use of ATT may suffice in a subset of patients, however, recalcitrant cases may need surgical intervention.
Footnotes
Author Disclosure Statement
No competing financial interests exist.