
Abstract
Abstract
Background:
The annual prevalence of antimicrobial exposure is high in the outpatient setting and should be a common exposure for surgical patients. Antimicrobials have negative side effects and may be associated with poor outcomes. Logically, one would expect surgical patients to be particularly susceptible to any negative effects of recent antimicrobial exposure. Despite these observations, however, the prevalence of recent antimicrobial exposure among surgical patients remains undefined. The purpose of this study is to define the prevalence of antimicrobial exposure in patients undergoing elective surgical procedures.
Methods:
Patients presenting for elective operations between August 4, 2015 and August 3, 2016 at our institution were asked prospectively about any antimicrobial exposure in the previous three months. Answers were recorded as either Yes, No, or Unsure. Patients were grouped according to age, American Society of Anesthesiologists (ASA) score, primary operative service, and post-operative destination. Descriptive statistics were employed using simple percentages and chi-square analysis when appropriate. Cochrane-Armitage test was used to evaluate temporal trends.
Results:
There were 21,473 elective surgical procedures performed during the study period across 13 operative services. Answers were recorded for 91.2% cases. The overall prevalence of exposure during this period was 28.6%. Exposure varied with age, ASA score, and surgical specialty. Vascular and transplant operations had the highest prevalence of exposure while ophthalmology and pediatric orthopedic procedures had the lowest. Patients with recent antimicrobial exposure were less likely to be discharged home on the same day and more likely to be admitted to an intensive care or intermediate care unit than those who denied recent exposure.
Conclusion:
In this descriptive analysis, the prevalence of recent antimicrobial exposure is overall approximately 28.6% and is higher than anticipated. Further work is needed to determine to what extent, if any, recent antimicrobial exposure impacts post-operative outcomes.
T
Antimicrobial agents have been associated with increased microbial resistance, Clostridium difficile infection, altered microbiome, as well as poor outcomes after a second significant stressor [5–11]. Given the high prevalence of antimicrobial exposure in the outpatient setting with potential negative effects, one would naturally expect surgical patients to be at increased risk for these potential complications. A thorough assessment of this potential risk should include an accurate assessment of the prevalence of recent antimicrobial exposure. This value, however, remains undefined in the literature.
The purpose of this study is to define the prevalence of recent antimicrobial exposure in the elective surgical population.
Methods
The Institutional Review Board Health Sciences Research (IRB-HSR) approved this study and approved a waiver of consent. Between August 4, 2015 and August 3, 2016, all elective surgical patients at the University of Virginia Health System were queried prospectively about recent antimicrobial exposure. Nurses in the pre-operative holding area asked each patient “Have you taken any antibiotics in the last 3 months?” and recorded the answer in our electronic medical record system as either Yes, No, or Unsure. The 3-month prevalence window was chosen by literature review [6–8,10,11]. Only operations occurring in either the main operating room or outpatient surgical center were recorded. Patients with interventions occurring in other procedural areas of the hospital were not queried.
Answers to our exposure survey question, patient age, surgical specialty, operative date, American Society of Anesthesiologists (ASA) classification score, as well as discharge destination were recorded. Descriptive statistics are listed. The chi-square test was used where appropriate. The Cochrane-Armitage test for trend was used to evaluate temporal trends in exposure rates. Statistical analysis was conducted using SAS software, version 9.3 (SAS Institute, Cary, NC).
Results
During the one-year study period, 21,473 elective surgical procedures were performed at our institution with 19,577 (91.2%) patients responding to our question. Overall, 28.6% (5,592) of these responses were Yes, followed by 70.1% (13,727) No and only 1.3% (258) Unsure responses. Fifty-two percent (10,370) of patients received their surgical procedure in the main operating area as opposed to the outpatient surgery center.
There were an average of 1,789.4 elective procedures each month (range: 1,636–1,981). Monthly response rates ranged between 95.9% and 84.0%, which was significant at p < 0.0001 (Fig. 1). Prevalence varied significantly by month (p = 0.01). The lowest response rates were in August, September, and October. Of the available responses, the prevalence of exposure changed very little from month to month (range: 31.0%–26.5%). There is a slight dip in exposure rates during the summer months; however, the Cochrane-Armitage test failed to identify a significant trend (p = 0.20). The difference between the highest and lowest exposed months was significant (February = 31.0% vs. July/October = 26.5%; p = 0.005).
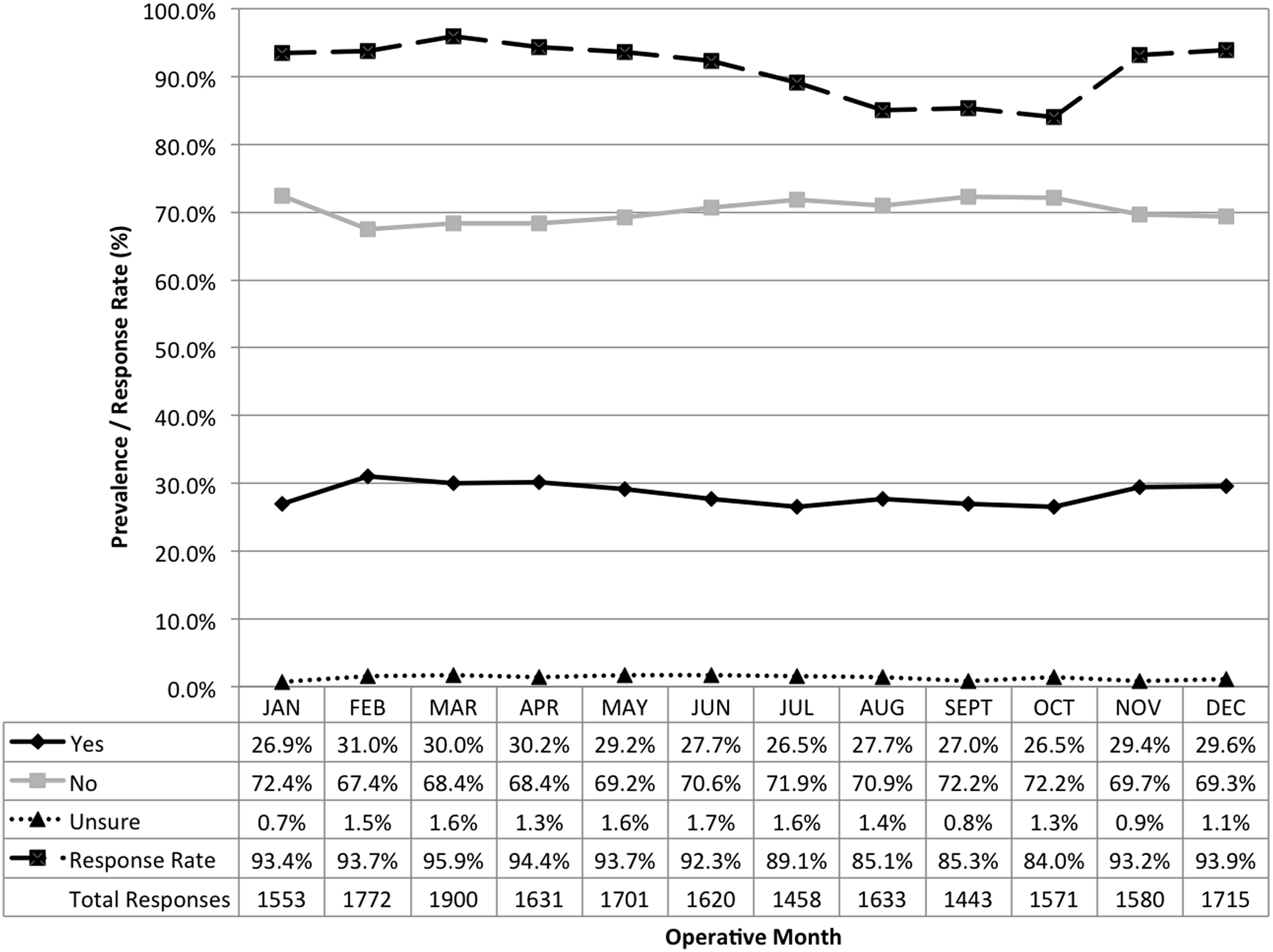
Trends in exposure by month. Response rate <0.0001; exposure p = 0.01; Cochrane-Armitage test for trend, p = 0.
Exposure prevalence by age is listed in Figure 2. Prevalence varied significantly by age (p < 0.0001). Children under the age of 10 years had the highest overall prevalence rates at 33.8% followed by patients aged 60–69 years (30.6%). Patients more than 90 years old had the lowest exposure rates within the previous three months at 24.3%.

Exposure by age group; p < 0.0001.
Patients with higher ASA scores had higher exposure rates (p < 0.0001; Fig. 3). The ASA class I patients had a three-month prevalence of 21.9% compared with 44.6% for ASA class IV patients.
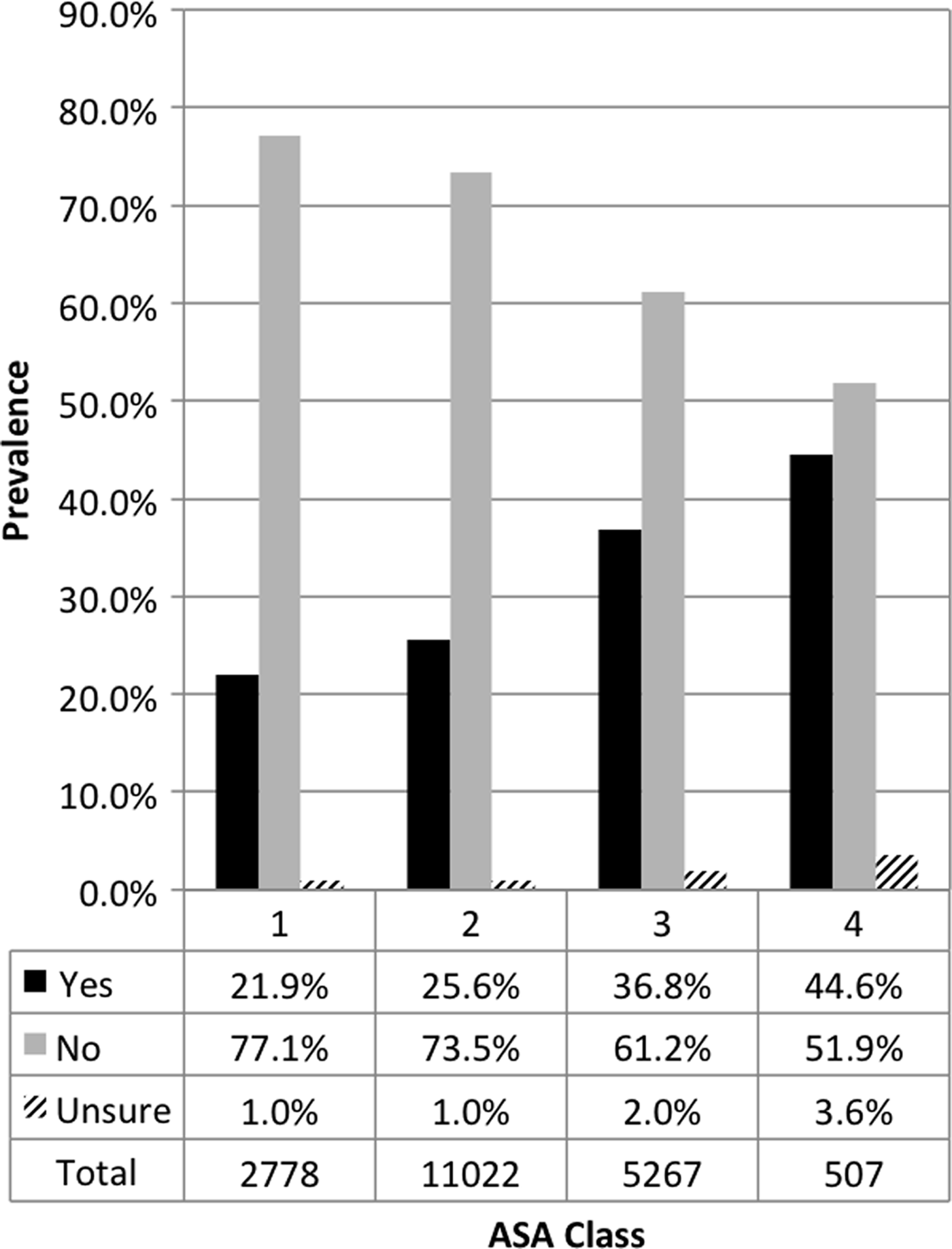
Exposure by American Society of Anesthesiologists (ASA) class; p < 0.0001.
Exposure varied by surgical specialty (p < 0.0001; Fig. 4). Patients undergoing vascular surgical procedures and abdominal transplantation procedures had the highest rates of exposure (43.1% and 38.3%). The prevalence among the general surgery population was 32.9%. Patients with operations in the ophthalmology (20.1%) and pediatric orthopedics departments (16.6%) had the lowest prevalence of exposure.
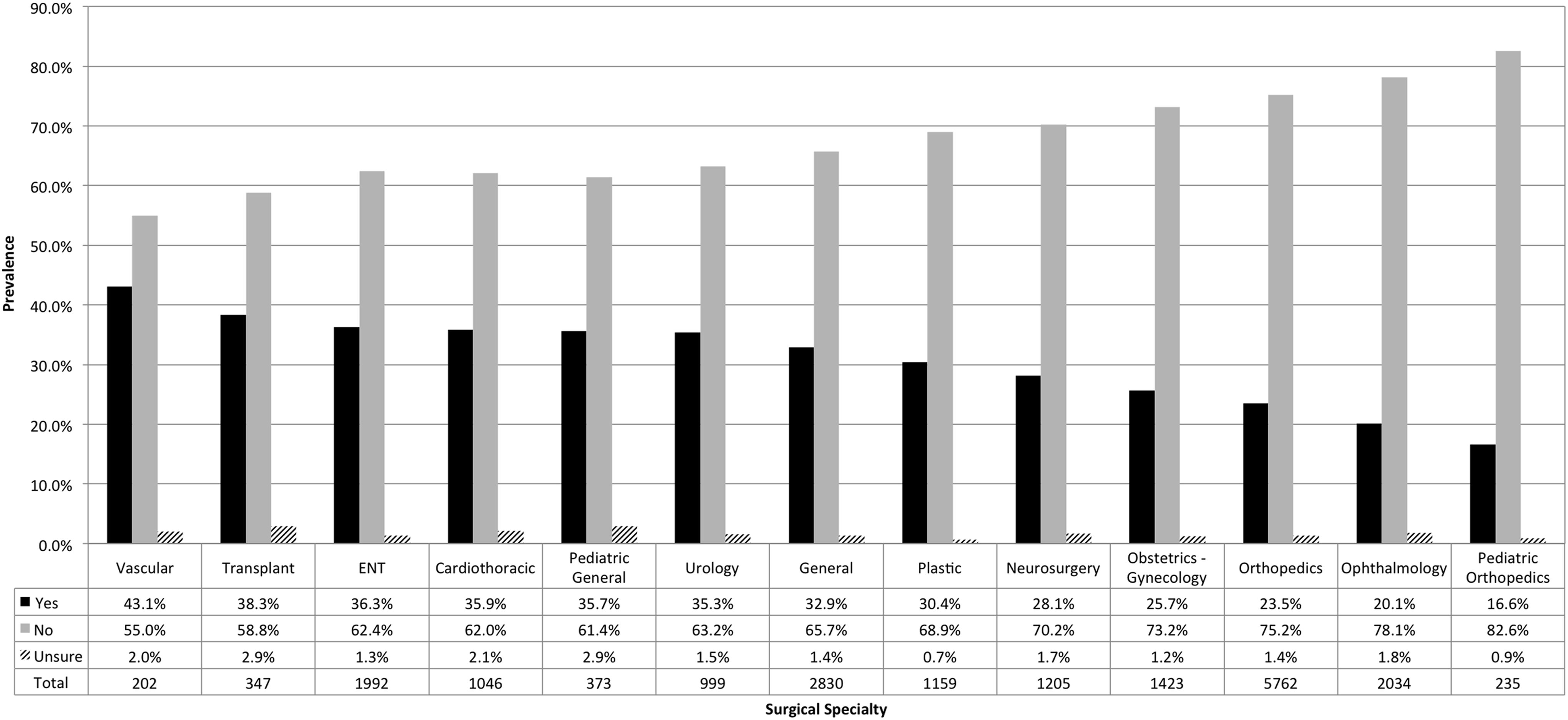
Exposure by surgical specialty; p-value = 0.0001. ENT = ear, nose, and throat.
Patients undergoing a surgical procedure in the main operating room rather than the outpatient center had higher rates of recent exposure (34.7% vs. 21.7%; p < 0.0001). In addition, patients with a recent antimicrobial exposure were less likely to be discharged home (45.4% vs. 59.3%; p < 0.0001) and significantly more likely to be admitted to an intensive care unit (8.8% vs. 5.7%; p < 0.0001] or intermediate care unit (2.2% vs. 1.6%; p = 0.002) post-operatively than those who did not have a recent antimicrobial exposure.
Discussion
In this prospective descriptive analysis, we defined the three-month prevalence of antimicrobial exposure across a broad spectrum of the elective surgical population during a one-year period at our institution. There were consistently low numbers of patients reporting Unsure. These data suggest that the three-month prevalence threshold is short enough that most patients can remember the exposure. There are lower response rates from August to October that correlate with the beginning of the study. An interim analysis performed in late October to evaluate our data collection efforts resulted in re-education of nursing staff and appears to have increased response rates throughout the remainder of the study. We were pleased with our response rates, however, during all portions of the study.
We identified some temporal variation in antimicrobial exposure with a dip in exposure rates during the summer months. This finding is likely because of the prevalence of upper respiratory infections during these times [12,13]. Exposure may vary not only with time of year but also with geographic location [14]. We consider the difference in monthly exposure rates to be small overall. Different locations may experience swings in exposure prevalence that were larger or smaller than what we observed.
Surgical patients appear to have higher rates of antimicrobial exposure than the general outpatient population. Shallcross et al. [3] described a 30.1% annual exposure rate while our exposure rate was 28.6% but over a much shorter threshold. The authors also describe that the presence of any comorbidities increased the antimicrobial prescribing rate by 44%. Patients requiring admission to long-term care facilities who likely have higher rates of comorbid conditions have a much higher exposure prevalence—up to 79% annually [4]. Our data support these findings. In our analysis, increasing ASA scores were associated with increased rates of exposure. Nearly half of all ASA class IV patients reported taking antimicrobials in the last 3 months.
We observed that exposed patients were more likely to be admitted to the hospital, intensive care unit, or intermediate care unit post-operatively. There are several possible explanations for this finding. The most likely is that exposed patients have higher comorbidities resulting in higher admission rates as observed by our ASA scores and others [3]. Also, we limited this study to only elective cases, but theoretically misclassification may allow urgent and emergent cases into our cohort resulting in higher exposure and admission rates. Finally, while it is possible that antimicrobial exposure may have somehow altered these patients' stress responses to surgical procedures resulting in a variation in admission status, other more benign causes and associations must be ruled out first, which is beyond the scope of this study.
Our study is strengthened by its prospective nature. Nonetheless, there are a few weaknesses worth discussing. First, we were not able to verify patient responses. Most patient-reported medical and surgical history, however, is not verified in practice, giving us no reason to suspect that these responses are any more or less valid than other patient-reported history items. Second, as a single center study, our data may not reflect the true prevalence of antimicrobial exposure nationally. Third, selection and recall bias may influence our reported prevalence.
Conclusion
This prospective analysis has defined the prevalence of recent antimicrobial exposure among elective surgical patients at a single institution. The overall prevalence of 28.6% is higher than expected. Prevalence varies by age, surgical specialty, and underlying degree of comorbidity reflecting differences in the underlying patient population. Further study is needed to evaluate the impact, if any, that antimicrobial exposure has on outcomes after surgical intervention and what this common exposure may say about the underlying population.
Footnotes
Author Disclosure Statement
No competing financial interests exist.