
Abstract
Abstract
Background:
Surgical site infections (SSIs) affect the safety of surgical care and are particularly problematic and prevalent in low and middle Human Development Index Countries (LMHDICs).
Methods:
We performed a systematic review of the existing literature on SSIs after tissue flap procedures in LMHDICs through the PubMed, Ovid, and Web of Science databases. Of the 405 abstracts identified, 79 were selected for full text review, and 30 studies met inclusion criteria for analysis.
Results:
In the pooled analysis, the SSI rate was 5.8 infections per 100 flap procedures (95% confidence interval [CI] 2%–10%, range: 0–40%). The most common indication for tissue flap was pilonidal sinus repair, which had a pooled SSI rate of 5.6 infections per 100 flap procedures (95% CI 2%–10%, range: 0–15%). No fatalities from an infection were noted. The reporting of infection epidemiology, prevention, and treatment was poor, with few studies reporting antibiotic agent use (37%), responsible pathogens (13%), infection comorbidities (13%), or time to infection (7%); none reported cost.
Conclusions:
Our review highlights the need for more work to develop standardized hospital-based reporting for surgical outcomes and complications, as well as future studies by large, multi-national groups to establish baseline incidence rates for SSIs and best practice guidelines to monitor SSI rates.
S
One component of this care is prevention of post-surgical infection. Infection can result in increased antibiotic agent use, extended hospital stays, flap loss, re-operation, and, in extreme cases, death. While the rate of SSIs after flap procedures in high Human Development Index Countries (HHDICs) is well described [4,5], less is known about the incidence of SSIs after flap procedures in LMHDICs.
To help address this deficit, we performed a prospectively registered systematic review of the existing literature on SSIs after surgical flap procedures in LMHDICs. Articles describing local or free flap procedures in these countries were critically evaluated to assess baseline SSI incidence and mortality rates and establish a potential benchmark for future studies.
Methods
We performed a systematic review of the existing literature describing the incidence and management of SSIs after tissue flaps in LMHDICs. This review was registered in the Prospero database (Project number 42016036658) in accordance with Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines. PubMed, Ovid, and Web of Science databases were searched using search terms “tissue flap,” “advancement flap,” “rotational flap,” “free tissue flap,” “fasciocutaneous flap,” “muscle flap,” and “pedicled flap” both individually and in combination with the countries of interest to identify articles from January 1, 2000 to March 1, 2016 (Supplementary Appendix 1; see online supplementary material at ftp.liebertpub.com).
Eighty-three countries were included in the search terms, based on the United Nations Development Programme classifications of low and middle Human Development Index Countries [6]. The period was chosen to select for modern studies with the most recent data and to reflect the improving trends in surgical care. The procedure of tissue flaps was chosen because these flaps are undertaken commonly for a wide range of indications; however, they are heterogeneous and poorly studied in these settings. Studies not written in English were included and translated using Google Translate. For the qualitative synthesis, we set no minimum number of patients per study, because we did not expect to identify many articles.
After initially screening for duplicates, abstracts were reviewed for relevance before obtaining full-text articles. Eligible articles were reviewed independently by two blinded reviewers. Reviewers evaluated each study for the following variables: Study location, study duration, study setting, study type, sample size, sample age, sample gender, type of flap procedure, use of pre-operative antibiotic agents, grading of SSIs, number of SSIs, type of SSIs, time to development of SSIs, pathogens, pathogen resistance, cost of infection, comorbid conditions, and need for re-operation. Exclusion criteria included articles with insufficient outcomes data on SSIs, multi-national studies that were not completely conducted in LMHIDCs, and duplicative studies based on the same patient cohort. Information not available from articles was obtained from article authors when possible. Bibliographies of studies were also examined for additional studies that were not identified during the initial search.
For the quantitative pooled infection rate analyses, we excluded studies with fewer than 20 patients based on an assumption of an infection rate of 15% in these settings to assure concordance with the rule of three sample size [7,8]. Pooled SSI rates and 95% confidence intervals (CIs) were calculated for all studies and multiple subgroups. Statistical analysis was performed using STATA® (Version 14.1). This was an Institutional Review Board exempt study because all articles reviewed were available publicly.
Results
Four hundred and five abstracts were initially identified after applying the search criteria (Fig. 1). After removing duplicates and non-relevant abstracts, 79 (20%) abstracts were selected for full-text review. Forty-nine full-text articles were excluded because of insufficient outcomes data, samples not being from LMHDICs, studies based on duplicative data, no surgical flap procedures, and animal studies. Thirty full-text articles ultimately met all inclusion criteria and were included in our qualitative analysis (Table 1) [9–38]. Nine studies had sample sizes of <20 and were excluded from the pooled infection rate calculations; all pooled infection rates reported are based on the subset of 21 studies with sample size of ≥20.
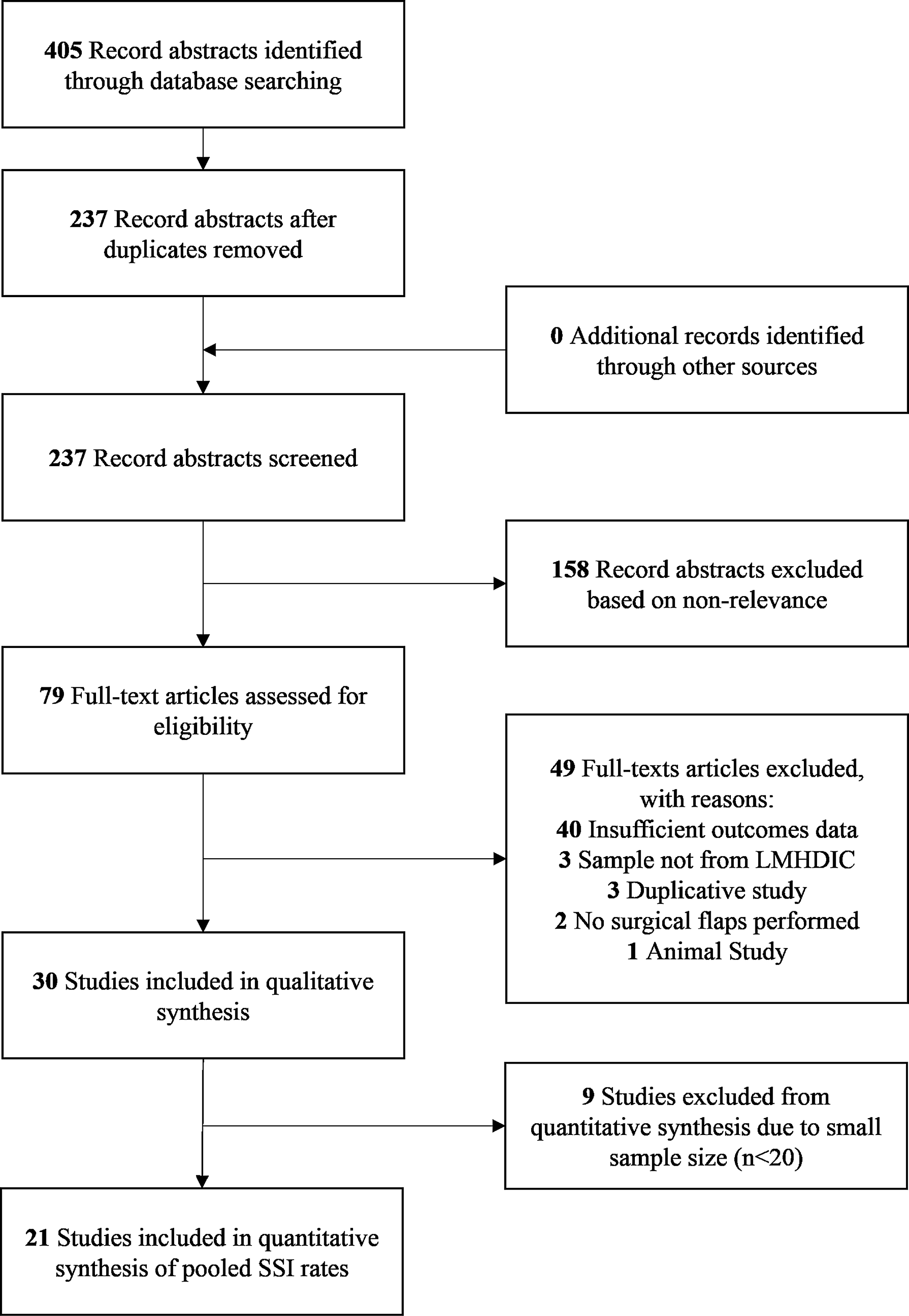
PRISMA diagram of report selection. PRISMA = Preferred Reporting Items for Systematic Review and Meta-Analysis; LMHDIC = low and middle Human Development Index Country; SSI = surgical site infection.
Indicates studies that had sample sizes of <20. These studies were excluded from the calculations for pooled infection rates, based on the assumption of an infection rate of 15% in these settings to assure concordance with the rule of three sample size.
SD = standard deviation; lat. = latissimus; ALT = anterolateral thigh; gastroc. = gastrocnemius TPF = temporoparietal fascia.
Of the final 30 articles, 28 (93%) were observational studies and two (7%) were randomized interventional studies. The most common countries of origin for these studies were Egypt (n = 9, 30%), India (n = 8, 27%), Pakistan (n = 3, 10%), and Nigeria (n = 3, 10%); other countries included Bangladesh, Iraq, Uzbekistan, Ethiopia, Sudan, Afghanistan, and Cote d'Ivoire (each n ≤ 2). Nearly all studies were conducted in single institutions (n = 26, 87%). Twenty-seven (90%) studies described local and regional flaps, one study (3%) evaluated free flaps exclusively, and two (7%) studies examined both free flaps and local and regional flaps. Pre-operative antibiotic agents were recorded as given in 11 (37%) studies, while the remaining 19 (63%) studies did not explicitly specify whether pre-operative antibiotic agents were administered. Few studies reported responsible pathogens (13%) [12,23,27,33], infection comorbidities (13%) [9,15,27,36], time to infection (7%) [27,38], and bacterial resistance (7%) [12,27]. No studies recorded the cost associated with treatment.
In a pooled analysis of all studies of sufficient sample size, the SSI rate was 5.8 infections per 100 flap procedures (95% CI 2%–10%, range: 0–40 infections per 100 flap procedure). In the two studies that used free flaps, the SSI rate was 8.5 infections per 100 flap procedures (95% CI 0–21%, range: 0–13 infections per 100 flap procedures). In the 20 studies that used local and regional flaps, the SSI rate was 5.0 infections per 100 flap procedures (95% CI 1%–9%, range: 0–40 infections per 100 flap procedures). In the eight studies in which pre-operative antibiotic administration was documented, the pooled SSI rate was 6.9 infections per 100 flap procedures (95% CI 1%–13%, range: 0–25 infections per 100 flap procedures). Although antibiotic agent use was not explicitly stated in the other studies, the pooled SSI rate of the 13 remaining studies was 5.1 infections per 100 flap procedures (95% CI 0–11%, range: 1–40 infections per 100 flap procedures). Only one instance of an organ/space infection was recorded after a necrotic flap used for maxillary and nasal reconstruction. No fatalities were noted (Table 2).
SSI = surgical site infection; CI = confidence interval.
The most common indication for a surgical flap among the reviewed articles was pilonidal sinus repair (n = 6). Subgroup analysis of flaps for pilonidal sinus showed infection rates ranging from 0–5 infections per 100 flap procedures with one outlying study with an infection rate of 15 infections per 100 flap procedures. The pooled populations for these studies included 352 patients with 20 SSIs for a pooled cumulative incidence rate of 5.6 infections per 100 flap procedures (95% CI 2%–10%, range: 0–15 infections per 100 flap procedures). The outlying study with an SSI rate of 15% exclusively treated patients with recurrent pilonidal sinuses who had been operated on previously and were presenting for revision procedures.
Discussion
In our review of the past 16 years of literature on SSI rates after surgical flap procedures in LMHDICs, only 30 studies had sufficient outcomes information for qualitative or quantitative analysis. Studies showed a wide distribution of SSI rates, ranging from 0 in four studies [16,25,30,35] to ≥25% in four studies [17,24,32,38]; more than half of the studies' SSI rates fell between 3% and 15%. As expected, there was some variability in SSI rates among flap type and flap indication.
For some flap procedures, there were similar infection rates between procedures performed in HHDI and LMHDI. Among patients undergoing flap surgery for breast reconstruction, SSI rates were reported between of 1%–12% [13,29,34]. The frequency of infection reported in these studies is similar to a review of nearly 3000 US-based free flap breast reconstructions, which noted an overall SSI rate of 4.9% [4]. Similarly, pilonidal sinuses are a relatively common condition with an incidence of 26 per 100,000 person-years [39]. In our review, pilonidal sinus closure was the most common indication for performing a surgical flap; five studies reported predominantly first-time closures with SSI rates between 0 and 5 infections per 100 flap procedures, and one study reported on recurrent sinus closures with an SSI rate of 15 infections per 100 flap procedures. These six studies focused predominantly on Karydakis and Limberg flaps, and their reported SSI rates are consistent with the existing literature. A recent Cochrane review of surgical management for pilonidal sinus found a pooled incidence of 10.0 infections per 100 surgical interventions and an SSI risk ratio of 3.75 for midline (e.g., Limberg) versus non-midline (Karydakis) closures (13 infections vs. three infections per 100 surgical interventions) [40]. Given the relatively higher SSI rate associated with midline closures, additional studies that directly compare the SSI rate of these two common techniques may help guide surgical management in LMHDIC settings.
A common indication for flaps is coverage of traumatic injuries. Road traffic injuries (RTIs) are responsible for approximately 1.25 million deaths each year, 90% of which occur in low- and middle-income countries [41]. Based on the current trajectory, RTIs are predicted to become the seventh leading cause of death globally by 2030. RTIs create contaminated wounds, poorly vascularized tissue beds, and complex polytrauma injuries. Three studies focused exclusively on flap procedures after RTI traumas, and six additional studies included patients who had sustained soft tissue defects secondary to RTIs. The three studies that examined flap outcomes exclusively after RTIs had SSI rates of 0, 11, and 31 infections per 100 flap procedures [9,25,32], while the SSI rates for the six studies that included RTIs as part of the sample ranged from two to 15 infections per 100 flap procedures [12,18,21,27,35,38]. These six additional studies, however, did not provide a breakdown of SSIs based on the initial indication, which may affect the reported SSI rate.
To compare, a review of free flap reconstruction after traumatic upper extremity injury in HHDICs found infection rates ranging from seven to 17 infections per 100 flap procedures, with variation based on the time from injury to reconstruction [42]. Meanwhile, other retrospective single-site studies in HHDICs examining lower extremity reconstruction after trauma have reported infection rates ranging from 12 to 33 infections per 100 flap procedures [43,44]. While these rates initially appear similar, it is unclear whether there are differences in the severity of initial injury, long-term functional outcomes, or other confounding factors that influence SSI. In the absence of these data, it is challenging to directly compare the infection rates between LMHDICs and HHDICs.
Less than half of the studies described pre-operative antibiotic use. We suspect, however, that antibiotic agents were administered in a majority of the studies reviewed, given the similar SSI rates between studies that reported pre-operative antibiotic agent use and those that did not. The role of prophylactic antibiotic agents in reducing SSI is well described, and new literature now examines factors such as timing and type of prophylaxis. While the studies in this review sometimes specified whether antibiotic agents were administered pre-operatively, they typically did not identify the class of antibiotic agent, the timing of pre-operative administration, or whether they were continued post-operatively. This highlights a need not only for the use of prophylactic antibiotic agents for such procedures, but also for detailed documentation of how prophylaxis is performed to place subsequent SSI investigations into context.
A United States (U.S.)- and Canada-based review found that costs of SSIs ranged from less than $400 per case for superficial SSIs to more than $30,000 per case for organ or space infection [45]. Similarly, a U.S.-based study on SSIs after breast operations found that SSIs accounted for an additional median cost of $10,750 and an additional median 4.3 days of hospital stay [46]. There is a paucity of literature on the cost of SSIs in low-resource settings for any procedure. None of the studies in this review examined the cost associated with SSI. Several studies noted their methods for treating patients with an SSI—ranging from intravenous antibiotic agents to debridement and skin grafts to new flap reconstruction—which could be used as a crude approximation for the cost of the SSI, but no objective data were available. This highlights a need for future studies to explore both the direct and indirect economic burden of SSIs.
This review has several limitations. First, the broad range of indications, types of flaps, and surgical techniques limit our ability to apply the results of this study to particular surgical flap procedures. These pooled results, however, do give us a better understanding of the infection burden for complex flap procedures in general. Second, only a small subset of the 83 LMHDICs was included in this review. Even including all full-text articles that were reviewed and not included in the final analysis, studies on surgical flaps were only available from 22 LMHDICs. Clearly there is wide variation between surgical prophylaxis and post-operative care between institutions and between countries. This review, however, is to our knowledge the most broad-reaching attempt to date to define a baseline SSI incidence after flap reconstruction. Third, there may be selection bias in the literature for studies with lower infection rates. It is possible that surgeons with particularly high SSI rates may elect not to publish their results, which would skew the reported infection rates. Further, the majority of these studies do not differentiate between superficial, deep, or organ/space infections and typically report all infections as equivalent. This once again limits our ability to compare results between studies and to generalize our findings. Finally, sample sizes for the studies tended to be small and may collectively be underpowered to provide accurate infection rates. We attempted to limit this by performing a subanalysis of studies with ≥20 patients, but this could still bias our sample.
This study highlights the need for more work to develop standardized hospital-based reporting for surgical outcomes and complications, as well as future studies by large, multi-national groups to establish baseline incidence rates for SSIs and best practice guidelines to monitor SSI rates. Best practice guidelines exist for the monitoring of SSIs in acute-hospital settings in the United States [47]. Using reporting systems such as the Centers for Disease Control and Prevention's National Healthcare Safety Network, these systems rely on internet infrastructure and resources that may not be broadly available in LMHDICs. Similarly, best practice guidelines for reducing the incidence of SSIs in a global setting, such as those promulgated by the World Health Organization [48], offer solutions on how to manage this complication in resource-constrained settings but fall short in how to monitor SSIs at either a hospital or national level. Establishing effective, practical, and cost-effective international SSI monitoring systems is essential to effectively grade the success or failure of recommended prevention efforts.
A majority of the full texts that we reviewed did not discuss SSIs, and most of those that did provided limited data on antibiotic agent use, infection comorbidity, causative organisms, and pathogen resistance. Studies by the International Nosocomial Infection Control Consortium on tracking country-by-country SSI rates provide data such as culture results and antibiotic resistance and could serve as a model for future studies [49–51]. Ultimately, by failing to identify causative organisms, patient comorbidities, and pathogen resistance, it is challenging to clearly establish epidemiologic factors that contribute to SSIs and their subsequent management in LMHDIC settings. This review underscores the importance of developing widespread hospital-based SSI surveillance programs.
Conclusions
As patients in low-resource settings increasingly gain access to surgical care, it is critical to establish a baseline for surgical outcomes and complications, particularly for SSIs. Little literature exists, however, that quantifies the rate of SSIs after surgical flap procedures in LMHDICs. Based on our review of existing studies, there is wide variability in SSI rates after flap procedures. The small number of studies, however, makes it difficult to conduct rigorous subgroup analyses on specific indications or flap procedures. Large multi-national studies that describe the risk factors for development of SSIs, epidemiology of pathogens, antibiotic resistance patterns, patient factors, and cost of infection are needed to establish expected SSI rates across a range of LMHDICs.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.