
Abstract
Abstract
Background:
Surgical site infections (SSIs) are a leading cause of post-operative morbidity and mortality. We developed Clean Cut, a surgical infection prevention program, with two goals: (1) Increase adherence to evidence-based peri-operative infection prevention standards and (2) establish sustainable surgical infection surveillance. Here we describe our infection surveillance strategy.
Patients and Methods:
Clean Cut was piloted and evaluated at a 523 bed tertiary hospital in Ethiopia. Infection prevention standards included: (1) Hand and surgical site decontamination; (2) integrity of gowns, drapes, and gloves; (3) instrument sterility; (4) prophylactic antibiotic administration; (5) surgical gauze tracking; and (6) checklist compliance. Primary outcome measure was SSI, with secondary outcomes including other infection, re-operation, and length of stay. We prospectively observed all post-surgical wounds in obstetrics over a 12 day period and separately recorded post-operative complications using chart review. Simultaneously, we reviewed the written hospital charts after patient discharge for all patients whose peri-operative adherence to infection prevention standards was captured.
Results:
Fifty obstetric patients were followed prospectively with recorded rates of SSI 14%, re-operation 6%, and death 2%. Compared with direct observation, chart review alone had a high loss to follow-up (28%) and decreased capture of infectious complications (SSI [n = 2], endometritis [n = 3], re-operations [n = 2], death [n = 1]); further, documentation inconsistencies failed to capture two complications (SSI [n = 1], mastitis [n = 1]). Concurrently, 137 patients were observed for peri-operative infection prevention standard adherence. Of these, we were able to successfully review 95 (69%) patient charts with recorded rates of SSI 5%, re-operation 1%, and death 1%.
Conclusion:
Patient loss to follow-up and poor documentation of infections underestimated overall infectious complications. Direct, prospective follow-up is possible but requires increased time, clinical skill, and training. For accurate surgical infection surveillance, direct follow-up of patients during hospitalization is essential, because chart review does not accurately reflect post-operative complications.
G
Understanding and capturing true post-operative infection rates in LMICs is a major challenge. A successful surveillance program includes standardized definitions of infections, effective surveillance methods, organized data collection, and analysis and sharing of results to clinical staff [10]. SSI surveillance methods have been well studied in high-resource settings, although they require adaptation to LMICs [10,11]. Inpatient data collection methods include both direct patient observation at various time intervals and retrospective written chart reviews; however, in LMICs, data extraction from written records is challenging, and electronic medical records are often non-existent. Because most SSIs occur after discharge, outpatient follow-up is important [12]. There are no standard methods for outpatient follow-up, with possible options including scheduled clinic return, patient questionnaires, or ongoing chart review [11,13]. Many of these methods are challenging in LMICs because of poor patient follow-up, long travel distances, and poor access to telecommunication.
In May 2016, the Ethiopia Federal Ministry of Health launched the nationwide program Saving Lives Through Safe Surgery (SaLTS) to address the national burden of disease by promoting improvements in surgical delivery and safety [14,15]. In Ethiopia, cost-effective, simple, and reliable safe surgical implementation strategies are imperative to deliver on the SaLTS mission, yet prevention of post-operative infections is a complex process necessitating proper management and adherence to infection prevention standards. In addition, the magnitude of the problem is unknown, because surveillance is not universally undertaken. The SSI rates in Ethiopia likely range 10%–60%; Jimma University Specialized Hospital (JUSH), the site for this study, reported previously an 11.4% SSI rate after cesarean section[16–21]. In LMICs, prevention and surveillance of surgical infections are critical to delivering safe surgical care [22].
We developed Clean Cut as a peri-operative infection prevention strategy based on standards embedded in the World Health Organization (WHO) Surgical Safety Checklist. While not specifically part of SaLTS, its two aims fell within the Ministry's program goals: (1) To increase adherence with peri-operative infection prevention standards, and (2) to establish sustainable surgical infection surveillance. Because this program required a reliable method for post-operative infection surveillance, we selected inpatient and outpatient surveillance initially via indirect methods of written medical chart review given the potential ease of adaptability across multiple sites and the lower requirement for clinical skill, training, and time investment. To assess the accuracy and validity of this chart review method, we conducted prospective inpatient direct follow-up with subsequent chart review. We describe our infection surveillance program component with lessons learned from these two distinct strategies.
Patients and Methods
We conducted a prospective, pre- and post-intervention study observing adherence to critical peri-operative infection prevention standards at JUSH, a 523 bed tertiary teaching hospital in Jimma, Ethiopia. JUSH is one of the oldest teaching hospitals in the country and the primary referral hospital for 15 million people in its catchment area of southwestern Ethiopia. The JUSH performs approximately 1,800 cesarean deliveries a year, along with 3,000 elective non-obstetric operations, another 3,000 emergency operations, and 300 minor procedures. At the time of the study, the hospital had three main, one pediatric, one ophthalmic, and two separate obstetric operating theaters (OT).
The Clean Cut infection prevention standards targeted for improvement included: (1) Hand and surgical site decontamination; (2) integrity of gowns, drapes, and gloves; (3) instrument sterility; (4) prophylactic antibiotic administration; (5) surgical gauze tracking; and (6) checklist compliance (Table 1). Peri-operative adherence was recorded on a standardized paper data form by data collectors (three operating theater nurses and one nurse anesthetist) who were trained by a visiting surgical fellow to observe and document surgical practices. We included all patients undergoing surgical intervention regardless of age, gender, or diagnosis. Data collectors were assigned to the operating theater a minimum of five days a week, with a rotating schedule to ensure capture of emergency and nighttime operations. Because cesarean section was such a large proportion of all cases, we categorized its primary indication according to clinician documentation: Poor presentation (including malpresentation and breech), obstructed labor (including failure to progress and cephalopelvic disproportion), fetal distress, previous cesarean section, cord prolapse, failed induction, pre-eclampsia/eclampsia, uterine rupture, ante-partum hemorrhage (including placenta previa or placental abruption), multiple gestation, other reason, and unknown reason (Table 2). Results from this implementation program are still being collected at the time of publication.
No distilled water available in maternity during study period.
No processes for confirming autoclave function besides class 1 indicator color change on outside of packages.
We followed patient outcomes for the duration of the study. Our primary outcome of interest was SSI, with secondary outcomes of other infectious complication, re-operation, length of stay, and disposition on discharge (dead or alive). The SSIs were classified as superficial, deep, and organ space according to Centers for Disease Control and Prevention definitions [23]. For our data collection process, to operationalize the SSI definition, improve usage, and decrease potential for misclassification, we defined SSI as “pus draining from the wound,” “closed wound opened,” and “wound with foul smell.”
Other infectious complications were defined as any HAI occurring within 30 days after operation and included urinary tract infection (UTI), pneumonia (PNA), endometritis, and other unspecified HAIs. A UTI was defined as clinical documentation of infection with prescription of antibiotic agents based on appropriate symptoms with a urinalysis suggestive of infection (positive nitrites, leukocyte esterase, or positive urine culture); PNA was defined as clinical documentation of infection with prescription of antibiotic agents based on two of the following symptoms: Dyspnea, purulent secretions, a new infiltrate on chest radiography, and elevated leukocyte count. Endometritis was a clinical diagnosis defined as the presence of at least two of the following signs with no other recognized cause: Fever (temperature of at least 38°C), uterine tenderness, and abnormal lochia. Unspecified HAIs were defined as written documentation of an infectious complication with prescription of an antibiotic agent.
From September 9 to 20, 2016, we performed a 12-day prospective study in the obstetrics ward, where previously published baseline infection rates were available. Inclusion criteria were any post-operative patient in the obstetrics ward with at least one direct observation of the surgical wound on rounds. Exclusion criteria were those patients operated on during this time period with no observation on patient ward rounds. Two inpatient infection surveillance strategies were utilized. Direct follow-up was defined as patient outcome data obtained during the direct every-other-day follow-up of patients during ward rounds. Chart review only was defined as patient outcome data obtained only from review of hospital records. For comparison, a true rate was compiled, incorporating both an inpatient (direct follow-up) and outpatient (chart review) surveillance approach, 30 days after discharge (Fig. 1). Primary and secondary outcomes were calculated for all patients from both surveillance methods. During the same time period (August 15 to September 23, 2016), we reviewed the written hospital charts after patient discharge for all patients whose operation was observed and captured in the main, orthopedic, and pediatric OT by the data collectors during the baseline period. A visiting surgical research fellow (JAF) attended bi-weekly patient ward rounds to assess charting accuracy.
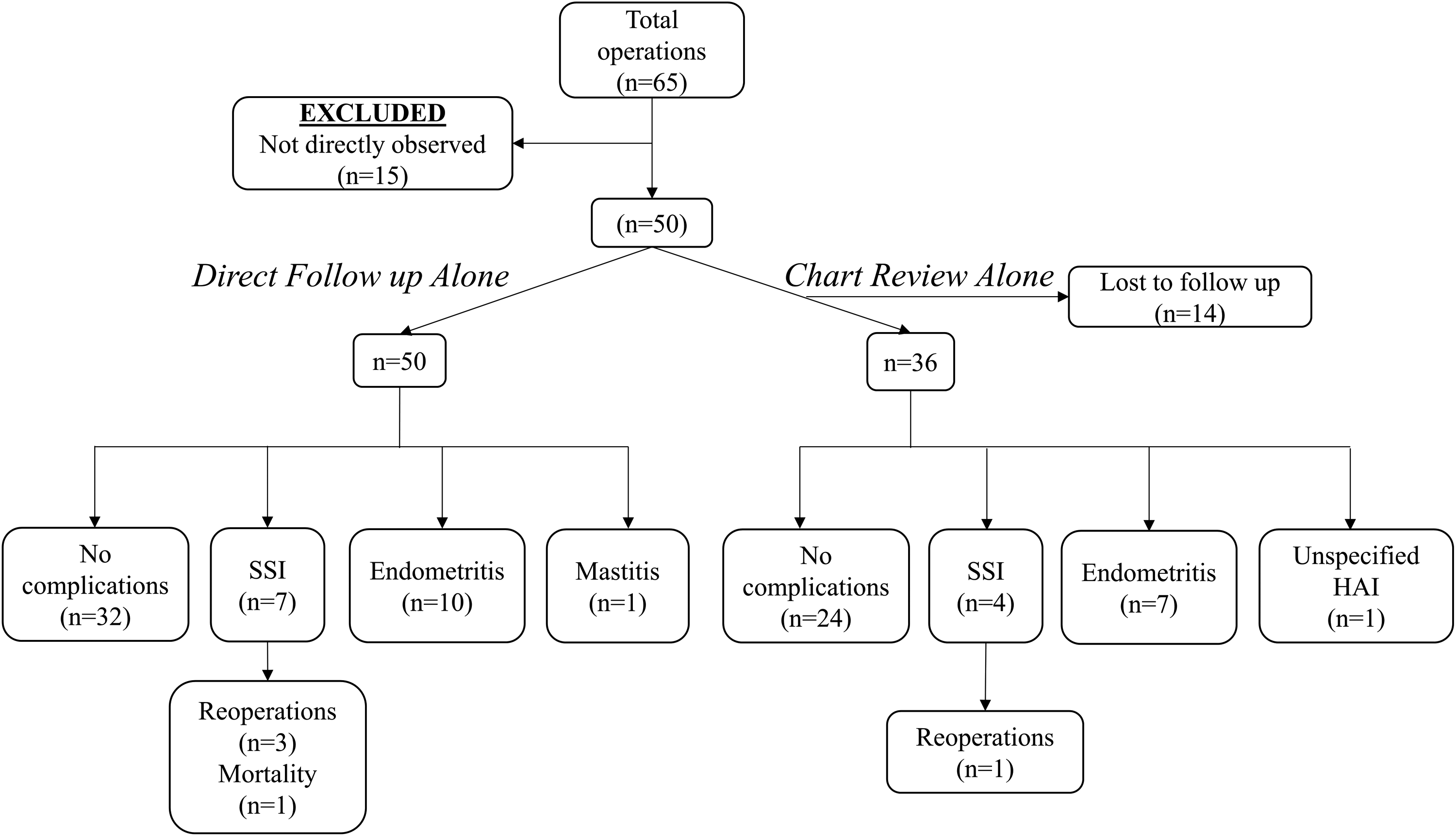
Obstetrics surgical infection surveillance method. SSI = surgical site infection; HAI = hospital-acquired infection.
Direct consent from patients was not required because the intervention is a quality improvement strategy that does not introduce new clinical methods or involve any direct risk to patients. The study was approved by the Institutional Review Boards at Stanford University and the College of Health Sciences at Jimma University. A Student t test was used to compare average hospital length of stay between those with and without infection, and p < 0.05 was considered significant. Microsoft Excel (Microsoft, 2013, Redmond, WA) was used for all statistical analysis.
Results
There were 65 total operations in the obstetric OT during the 12-day observational period of which we were able to directly observe 50 patients on ward rounds. Patients averaged 28 years (range 18–40), with the majority being emergency operations (76%); 90% underwent cesarean section with the most common indications being obstructed labor (n = 10), poor presentation (n = 9), and fetal distress (n = 7) (Table 3). Through direct follow-up on ward rounds, the post-operative infectious complication rate was 36% (superficial SSI 10%, deep space SSI 4%, endometritis 20%, mastitis 2%), with three re-operations and one death. Using chart review alone, 14 (28%) patients were lost to follow-up, and of those whose charts were available for review, we noted a post-operative infectious complication rate of 33.3% (11.1% SSI, 19.4% endometritis, and 2.78% unspecified HAI) and one re-operation (Fig. 1).
p = 0.0068.
SSI = surgical site infection; CI = confidence interval.
Combining inpatient direct follow-up with post-discharge chart review, we noted a post-operative infectious complication rate of 44% (superficial SSI 10%, deep space SSI 4%, endometritis 26%, mastitis 2%), with three re-operations and one death. Overall post-operative average length of hospital stay was 5.81 days ±1.82 with a significant difference between those with (8.94 days ±3.71) and those without post-operative infectious complications (3.43 days ±0.85); p = 0.0068 (Table 3).
When comparing the directly observed follow-up group with the charted documentation from this same cohort of patients, there were marked differences in patient outcome because of loss to follow-up and documentation errors. Of the 28% of patients lost to follow-up because of missing charts, there was substantial morbidity and death captured by direct follow-up: SSI (n = 2), endometritis (n = 3), re-operations (n = 2), death (n = 1). Of the 36 patients with successful chart review, eight patient charts (22%) had no discharge summary, and two patient charts (5.56%) failed to mention observed infectious complications (SSI [n = 1], mastitis [n = 1]); however, three patient charts (8.3%) revealed a previously undiagnosed infectious complication not identified during direct ward rounds (endometritis [n = 3]) (Fig. 1).
Among the patients undergoing a surgical procedure in the main, obstetrics, and pediatric OT, we directly observed 137 operations (89.8% in main/pediatric OT, 10.2% in obstetrics OT). Patients were majority female (56.2%), average age 38 years (range 8 months–85 years), and primarily consisting of elective operations (83.2%); the most common pre-operative diagnoses were bladder outlet obstruction from benign prostatic hypertrophy (n = 19), obstetrics (n = 15), and thyroid pathology (n = 14) (Table 2). Of these, 42 (30.7%) patients were lost to follow-up because of missing medical charts. Review of the 95 available medical records identified a 17% post-operative infectious complication rate (5% SSI, 4% unspecified HAI, 3% UTI, 2% PNA), with one re-operation and one death (Table 4). Overall post-operative average length of hospital stay was 5.46 days ±1.42 with a significant difference between those with (9.36 days ±5.69) and those without post-operative infectious complications (4.78 days ±1.36), p = 0.02 (Table 4). Scrutiny during observed ward rounds revealed multiple documentation inconsistencies including failure to record suture removal to open infected wounds, initiation of antibiotic agents without documented indications, UTIs, wound dehiscence, and SSIs.
p = 0.0215.
SSI = surgical site infection; CI = confidence interval.
Discussion
There are few studies of SSI surveillance methods in sub-Saharan Africa, although combining surveillance with a surgical infection prevention quality improvement program is essential [13,24,25]. Our study investigating surgical infection surveillance methods in a group of obstetrics patients found a substantially higher rate of post-operative infectious complications detected using direct inpatient follow-up combined with chart review compared with retrospective chart review alone (44% vs. 36%). The rate of SSIs (14% vs. 11%), re-operations (6% vs. 3%), and death (2% vs. 0%) were all markedly higher with direct follow-up compared with retrospective chart review in this obstetrics group. The results demonstrate that within the prospectively observed obstetric patients, there was a significant increased post-operative length of stay in those with infectious complications, demonstrated also in the larger baseline group.
The patient outcome differences between the two follow-up strategies demonstrate that effective inpatient surgical infection surveillance requires a component of direct follow-up, necessitating clinical skill and training. Within the obstetrics cohort, loss to follow-up was the largest contributor to patient outcome differences, representing 23.8% of the total post-operative infectious complications, along with two re-operations and one death. Documentation errors, detected through direct follow-up with subsequent retrospective chart review, accounted for a lost capture of almost 10% of the total post-operative infectious complications. The recorded 5% SSI rate of the baseline chart review only group is much lower than reported previously in Ethiopia and likely underrepresented because of the 30.7% lost to follow-up and potential documentation inconsistencies [16–20]. Direct follow-up is critical because it improves surgical infection surveillance accuracy, avoids loss to follow-up, and reduces the impact of documentation inconsistency.
The 14% SSI rate for the direct follow-up group in the obstetrics ward is similar to that reported previously at JUSH and among the highest reported for SSI surveillance studies in sub-Saharan Africa of cesarean section patients utilizing direct follow-up (4.9% to 16.4%) [21.26–35]. Our direct follow–up group consisted of majority obstetric emergencies, with obstructed labor accounting for the most common indication for cesarean section. This finding is similar to those reported previously in sub-Saharan Africa [36,37]. Patient loss to follow-up is similar, although our captured SSI rate is higher compared with other sub-Saharan African studies on SSI after cesarean section [38].
Post-cesarean endometritis accounted for a quarter of total post-operative infectious complications in the direct follow-up group. Our findings are substantially higher than historical rates (6%–18%) and different from most studies of infectious complications after cesarean section, with SSI being the most common [39,40]. There are multiple factors that could contribute to the elevated incidence of post-cesarean endometritis at our site, although we hypothesize that the prophylactic antibiotic choice could represent a particular risk factor. Ampicillin was the prophylactic antibiotic agent administered for cesarean sections at JUSH during this study period, which is insufficient coverage for the responsible bacterial flora. Published data on cultures from wound infections at JUSH demonstrated a high resistance to ampicillin (Staphylococcus aureus 91.8%, gram negative bacteria 57.1%–100%) [19].
There are important differences between JUSH during this study period and other sub-Saharan Africa studies utilizing prospective observational methods for SSI surveillance. In Rwanda, there was an implementation of infection prevention control strategies before the study period, and at all Medecins sans Frontieres sites, reliable electricity, clean water, and sterilization units were present [26,27]. At JUSH, this patient outcome follow-up comparison occurred before our infection prevention intervention. In addition, at JUSH, there is poor reliability of electricity and lack of running water in the obstetrics ward, which impacts patient care.
An ideal surgical infection surveillance strategy should incorporate inpatient direct follow-up and a post-discharge follow-up component. Importantly, in our cohort, of patients with post-cesarean endometritis, 23% received the diagnosis after discharge. We used retrospective chart review to help capture outpatient infectious complications, although other options are feasible. Chart review is important for highlighting potential surrogate markers for surgical infections, including duration of antibiotic prescription post-operatively and hospital length of stay. Chart review alone, however, underrepresents post-operative complications because of loss to follow-up and inaccurate charting. Outpatient surgical infection surveillance is challenging at JUSH given the high percentage of rural patients, poor cellular telephone access, and small percentage with reliable internet access [41]. Therefore, an infection surveillance strategy that incorporates inpatient surveillance using direct and indirect methods in combination with a reliable outpatient surveillance method is essential.
Limitations
There are a number of limitations to our study. First, the sample size in the cross-sectional direct follow-up group is approximately a third the size of the chart review group, which could potentially overestimate the burden of infectious complications. Given similar SSI rates during a one-year prospective study at JUSH, however, this seem unlikely [21]. Second, there are confounders between our two study groups including differences in patient demographics as well as in operating theater environments. The larger chart review only group consisted of mainly elective general surgical operations compared with the majority emergency obstetric operations in the obstetrics cohort. A higher baseline infection rate in the obstetrics cohort would lead to the notable differences between the two groups. In addition, patient co-morbidities known to increase the risk for development of post-cesarean endometritis, including premature rupture of membranes, chorioamnionitis, diabetes, and immunodeficiency, were not recorded. Given similar record keeping throughout JUSH, the underestimation of infectious complications noted in the obstetrics ward using chart review indicates a similarly likely underestimation of infectious complications in the general surgical baseline chart review group.
Third, endometritis is mainly a clinical diagnosis, which is inherent to provider bias. Regardless, we argue the importance for inclusion within infectious complications because post-cesarean endometritis is similar to an SSI given the organ space violation and re-approximation during the course of the operation. Last, it is unclear how much impact the differences in location and resources between the separate OTs had on patient outcomes. The main OT is located in the same building as the main central sterile re-processing area, whereas the obstetric OT is located separately. Importantly, in the obstetric OT, there is no running water for surgeon hand scrubbing and, during the study period, they utilized a different area with different autoclaves for sterile processing. The points made by creating an internal control and comparing chart review only against direct, prospective follow-up in the obstetric group are still valid, however.
Conclusion
Surgical infections cause substantial morbidity and death. Simple, reliable, and reproducible surgical infection surveillance methods are crucial for improving patient care. At our pilot site in Ethiopia, patient loss to follow-up and poor documentation underestimated overall infectious complications. Direct observation and prospective follow-up are possible in a resource-limited setting but are time-intensive and require substantial clinical acumen. For accurate surgical infection surveillance in LMICs, clinical training coupled with both inpatient follow-up using direct and indirect methods and post-discharge follow-up are essential.
Footnotes
Acknowledgments
The authors would like to thank all the JUSH data collectors—Gezahegn Tesfaye, Yibekal Ambachew, Bezawit Berhanu, and Wasihun Akeberegn—for their assistance on this study as well as the surgical, obstetric, and gynecology residents for their excellent care of the patients.
We would like to thank the GE Foundation for their grant to Lifebox for Clean Cut. The funder played no role in the decision to submit this work for publication, and the views expressed are those of the authors.
Author Disclosure Statement
JAF, LK, and TGW are members of Lifebox, where TGW is a trustee. For them and the remaining authors, no competing financial interests exist.