
Abstract
Abstract
Background:
Nutritional status has major impacts on the outcome of surgery, in particular in patients with cancer. The aim of this review was to assess the merit of oral pre-operative nutritional support as a part of prehabilitation in patients undergoing surgery for colorectal cancer.
Methods:
A systematic literature search and meta-analysis was performed according to the Preferred Reporting of Systematic Reviews and Meta-Analyses (PRISMA) recommendations in order to review all trials investigating the effect of oral pre-operative nutritional support in patients undergoing colorectal surgery. The primary outcome was overall complication rate. Secondary outcomes were incision infection rate, anastomotic leakage rate, and length of hospital stay.
Results:
Five randomized controlled trials and one controlled trial were included. The studies contained a total of 583 patients with an average age of 63 y (range 23–88 y), of whom 87% had colorectal cancer. Malnourishment rates ranged from 8%–68%. All investigators provided an oral protein supplement. Overall patient compliance rates ranged from 72%–100%. There was no significant reduction in the overall complication rate in the interventional groups (odds ratio 0.82; 95% confidence interval 0.52 − 1.25).
Conclusion:
Current studies are too heterogeneous to conclude that pre-operative oral nutritional support could enhance the condition of patients undergoing colorectal surgery. Patients at risk have a relatively lean body mass deficit (sarcopenia) rather than an absolute malnourished status. Compliance is an important element of prehabilitation. Targeting patients at risk, combining protein supplements with strength training, and defining standardized patient-related outcomes will be essential to obtain satisfactory results.
“L
Currently, surgery remains the cornerstone of the treatment for colorectal cancer [1]. This specific group of patients, of whom more than 50% are older than 65 years [2], has two imminent factors to put them at risk nutritionally. First, age itself is an independent risk factor for poor nutritional status [3]. Second, cancer can induce significant weight loss resulting in malnutrition [4]. Recent studies show that two of three patients with colorectal cancer experience weight loss pre-operatively, which in one in five is more than 10% [5].
Compared with other gastrointestinal malignancies, however, colorectal cancer is not a major risk factor for cachexia. Nevertheless, a status of relative protein deficiency is related to reduced muscle mass or sarcopenia [6]. Sarcopenia poses a significant risk for post-operative complications in patients undergoing colorectal surgery [7]. Hence, enhancing the nutritional status of these patients might decrease post-operative morbidity [8].
The “enhanced recovery after surgery” (ERAS) programs have contributed greatly to the speed and quality of recovery of patients undergoing colorectal surgery [9]. Nutritional support is a substantial part of these programs, but only in the peri-operative and post-operative periods. The waiting period prior to surgery could be a window of opportunity to enhance the nutritional status of the patients. This pre-operative enhancement has been called “prehabilitation” and can consist of any form of patient optimization before surgery [10].
Nutritional interventions can take many forms. The European Society for Parenteral and Enteral Nutrition (ESPEN) guidelines on nutrition in cancer patients state that nutrition counseling with oral nutritional supplements is the preferred first step in ensuring adequate nutrient intake before surgery [11]. As most patients will be cared for in an outpatient setting in the weeks before surgery, oral nutritional support also would be more practical and cost-effective than parenteral nutrition [12].
The aim of this systematic review and meta-analysis was to assess whether pre-operative oral nutritional support reduces the rate of post-operative surgical complications or improves the post-operative recovery rate in terms of length of hospital stay (LOS), quality of life, and functional outcome after colorectal surgery.
Patients and Methods
A systematic literature search and meta-analysis was performed according to the Preferred Reporting of Systematic Reviews and Meta-Analyses (PRISMA) recommendations [13].
Study selection
The last update of the search was performed on August 30, 2016 (revised for new publications August 1, 2017) involving the MedLine and Embase databases. The search was constructed with the aid of a clinical librarian and consisted of three search term categories: Type of surgery, timing of nutritional intervention, and content of nutritional intervention. The search string can be found in the Appendix.
Two authors (EB and TA) independently screened all titles and abstracts and the following full text articles. Disagreement was addressed by discussion and consensus. Following this process, a reference search of all included papers and relevant review articles was performed to identify any missed studies.
Eligibility criteria
Studies were included if they answered the clinical question as defined by the population, intervention, control, outcome (PICO) format. In order to study cause–effect relations, only randomized controlled trials (RCTs) and prospective cohort studies were included. The patients had to be 60 years or older and undergoing colorectal surgery. The intervention consisted of oral nutritional support in the form of macronutrients (proteins, carbohydrates, fats), eventually together with micronutrients (e.g., immunonutrition, vitamin supplements) or dietary advice, which is defined as any form of professional consultation involving dietary analysis and consequent advice. Because immediate pre-operative nutritional support is also part of the ERAS protocol [14] (e.g., pre-operative carbohydrate loading), we chose to include only studies that administered oral nutrition for at least 48 h pre-operatively. The control group was to receive a regular diet without specific nutritional support. The primary outcome was overall complication rate, preferably using the Clavien-Dindo scale [15]. Secondary outcomes were the incision infection rate, anastomotic leakage rate (definitions used by the authors of original studies), LOS, quality of life, and recovery (e.g. functional capacity) after the operation.
In order to study the effects of oral nutrition alone, studies investigating the effect of nutrition as a part of a multimodal prehabilitation program involving; e.g., exercise or psychological prehabilitation, were excluded. Studies investigating the effect of parenteral nutritional support also were excluded. Review articles, (retrospective) case-controlled studies, case reports, opinion papers, animal studies, and studies not in English also were excluded.
Assessment of methodological quality
Two authors (EB and TA) independently assessed the methodological quality of the studies. The Cochrane risk-of-bias tool considering seven items was used to grade the risk of bias [16]. A score below 4 of 7 was regarded as “high risk,” 4 of 7 as “moderate risk,” and above 4 of 7 as “low risk.” Disagreement was solved by discussion and consensus.
Data extraction
Study characteristics, including design, sample size, population, and type and duration of nutritional support were obtained from the acceptable studies by two authors (EB and TA). If mentioned, the following data were extracted: Overall complication rate, incision infection rate, anastomotic leakage rate, LOS, quality of life, measures of post-operative recovery, and compliance rate. If data were missing, the first authors of the papers were contacted.
Statistical analysis
Meta-analysis was used to estimate the pooled odds ratio (OR) for categorical data or mean difference (MD) for continuous data to compare the post-operative outcomes of patients having and not having nutritional support. Review Manager version 5.3 (The Nordic Cochrane Centre, Copenhagen, Denmark) was used to estimate the pooled results using the Mantel–Haenszel estimator to calculate odds ratios (ORs). After visual inspection for clinical heterogeneity, the Higgins I2 value was employed to assess statistical heterogeneity. A random-effects model was used to pool data. P < 0.05 was considered statistically significant.
Results
Search results
A complete flowchart of the search is presented in Figure 1. The initial search in PubMed and Embase produced 5,059 articles. After removal of duplicates and title and abstract screening, 52 articles remained for full-text reading. We excluded 47 articles because the study design, patient population, or the intervention did not meet the inclusion criteria. Five studies satisfied these criteria, and one additional study was found in a Cochrane review [20]. Five RCTs [21–25] and one prospective controlled study [26] were selected for analysis.
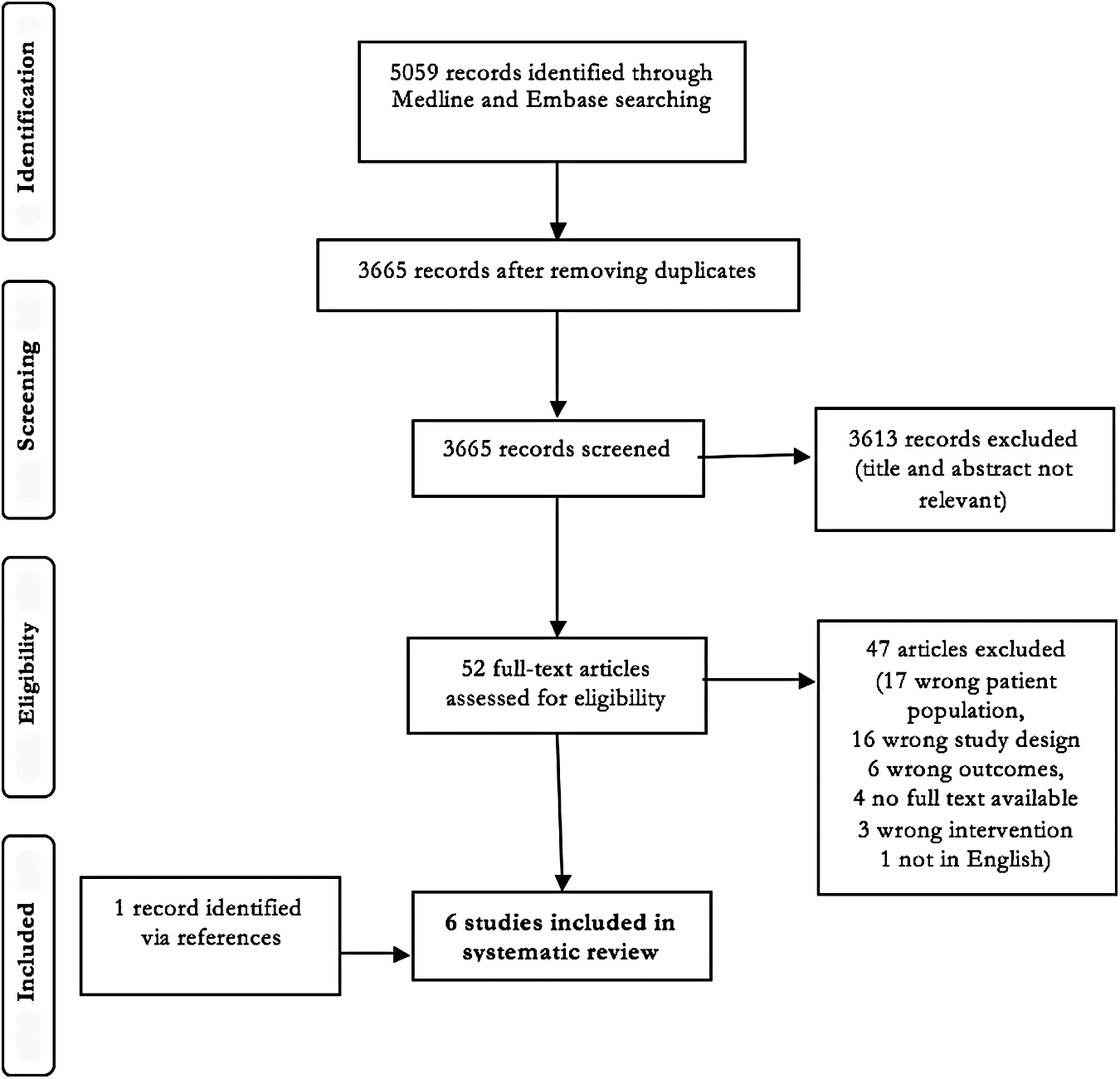
Preferred Reporting of Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of study.
Risk of bias
Two reviewers independently assessed the risk of bias for each article. The results are presented in Table 1. The assessment was done with the Cochrane risk-of-bias tool. One study was considered to be at high risk of bias [26]. Three studies were considered at moderate risk [22,23,25] and two studies at low risk of bias [21,24].

Baseline characteristics
The baseline patient and surgery characteristics are summarized in Table 2. All studies were published between 2002 and 2016 and included a total of 583 patients undergoing colorectal surgery. The mean age of the participants was 63 y (range 23–88 y). In four studies, all patients had colorectal cancer [21,22,24,26]. Smedley et al. [25] and Finco et al. [23] included 33% and 50% of patients, respectively, with a benign indication for colorectal surgery. Regarding the physical characteristics of the patients, malnourishment rates were mentioned in four studies [21,22,24,25]; the percentages ranged from 8% to 68%. Burden et al. [22] randomized more malnourished patients to the intervention group, whereas Horie et al. [26] excluded malnourished patients altogether. The definition of malnourishment differed among studies. Five studies [22–26] reported the average body mass index (BMI) of the participants, and three studies [22,24,25] reported the average handgrip strength (GS). The GS can be regarded as a functional measurement of sarcopenia. However, as GS cut-off points for sarcopenia are BMI and gender specific [6], it was not possible to calculate the percentage of functionally compromised patients. The study by Braga et al. [21] contributed two intervention groups and one control group to this review, all with 50 patients: Group 1 received pre-operative immunonutrition, group 2 received comparable nutrition but without micronutrients, and the control group received no supplements.
immunonutrition group **extra nutrition group without immunonutrition
BMI = body mass index; C = control group; CT = controlled trial; GS = grip strength; I = intervention group; kPa = kilopascals; NRS = nutritional risk screening; PG-SGA = patient-generated subjective global assessment; RCT = randomized controlled trial
Intervention characteristics
Table 3 gives an overview of the intervention characteristics. A liquid oral supplement was provided in all of the studies. In the study by Braga et al. [21], one group of participants received Oral Impact (Novartis/Nestlé), one group received an isoenergetic, isonitrogenous formula, and one group did not receive any supplements. Oral Impact also was provided in two other studies [23,26]. Two studies provided Fortisip (Nutricia) [22,25], and one study provided a whey protein supplement (Immunotec) [24]. Sponsorship of the supplements was not documented by Finco et al. [23] or Horie et al. [26].
immunonutrition group **extra nutrition group without immunonutrition
BMI = body mass index; RNA = ribonucleic acid; SD = standard deviation
The supplements consisted mainly of carbohydrates (approximately 50% of the total amount). Whereas Gillis et al. [24] provided only protein at an average of 19.8 g per day (which amounts to 22% of the daily requirement of a 70-kg person according to the ESPEN guidelines [11]), the amount of protein in the supplements in the other studies daily ranged from 18 g to 67.2 g (20% to 74% of the daily requirement [11]). Three studies provided immunonutrition (Oral Impact), which contains the micronutrients arginine, omega-3 fatty acids, and ribonucleic acids [21,23,26].
Most studies asked the patients to consume a standard amount of supplement ranging from 400 mL to 1000 mL per day. Smedley et al. [25] instructed the patients to drink as much as possible between meals, while Gillis et al. [24] provided the patients with an amount of protein that had been calculated to cover the individual protein deficit. Gillis et al. [24] were the only ones providing some patients with a non-nutritive placebo.
The duration of the complete program differed among the studies. Three studies provided the supplements for five days in the week preceding surgery [21,23,26]. The intervention in the three other studies spanned the entire pre-operative period starting from cancer diagnosis and the decision to operate and ending at hospital admission [22,24,25]. Gillis et al. [24] and Finco et al. [23] continued the supplements post-operatively for four weeks and three days, respectively.
Outcomes
Overall complication rate
All studies provided information on overall complications, but the outcome was not reported similarly in the various studies (dichotomous [21–24] vs. count data [25,26]). Dichotomous data were analyzed using risk ratios with Mantel-Haenszel in a random-effects method. Comparative meta-analysis of overall complication rates is presented in Figure 2; the rate was not significantly different between the intervention and control groups (OR 0.82; 95% confidence interval [CI] 0.52 − 1.25).
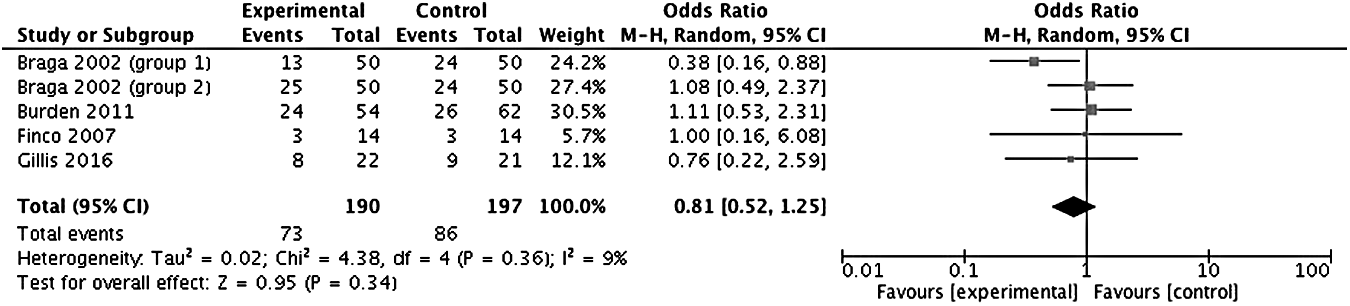
Meta-analysis of overall complications.
Incision infection rate
Four studies recorded incision infection rates [21–23,26], with Horie et al. [26] observing a significant difference in the rate between the intervention and control groups (0 vs. 14.7%; p < 0.05). The data were analyzed using risk ratios with Mantel-Haenszel in a random-effects method; the meta-analysis of incision infection rates is depicted in Figure 3. The overall effect showed no advantage for pre-operative nutritional support (OR 0.57; 95% CI 0.30 − 1.09).
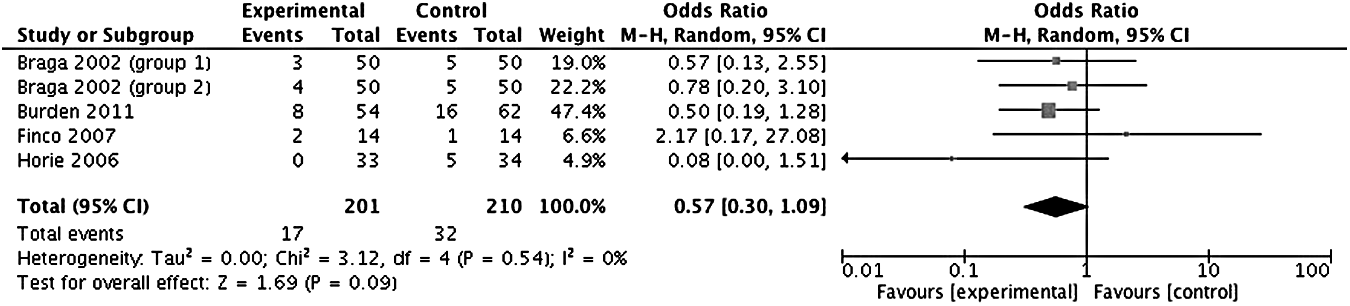
Meta-analysis of incision infections.
Anastomotic leakage rate
Three studies reported anastomotic leakage rates [21,23,26]. Because of the small number of such studies, no meta-analysis was undertaken for this outcome. The leakage rates ranged from 0 to 12% in the nutrition groups compared with 0 to 10% in the control groups. None of the studies demonstrated a significant difference between the treatment arms.
Length of hospital stay
Four studies reported LOS [21,23–25]. The mean number of days ranged from 7.6 to 12.8 in the nutrition group and 6.8 to 17.8 in the control group. Because of the large clinical and statistical heterogeneity among the studies, no meta-analysis was undertaken for this outcome.
Other outcomes
Two studies measured quality of life four weeks after surgery: Gillis et al. [24] used the Short Form Health Survey 36 (SF-36) [27], and Smedley et al. [25] used the SF-36 and EuroQol [28] instruments. No significant differences were found in the results of these questionnaires. Gillis et al. [24] also looked into functional walking distance with the six-minute walk test (6MWT) [29] and changes in lean body mass four weeks after surgery but found no differences between the intervention and control groups. Smedley et al. [25] quantified weight loss after surgery, but again, the groups were not significantly different. All outcomes are summarized in Table 4.
immunonutrition group bextra nutrition group without immunonutrition,∮reported as number of complications, significant results are emboldened
6MWT = 6-minute walking test; C = control group; I = intervention group; LBM = lean body mass; SD = standard deviation; QoL = quality of life
Compliance
Compliance with the intervention was recorded in four studies [21,22,24,26]. Rates ranged from 72% to 100% (Table 5). Three studies used patient diaries as a compliance instrument [21,22,24], Horie et al. [26] did not specify how compliance was recorded, and Gillis et al. [18] had weekly contact with the participants to identify problems with compliance. No extra measures to increase compliance were employed in any of the studies.
immunonutrition group bextra nutrition group without immunonutrition
Patient diary
Feedback result visible to patient
Discussion
The current review was unable to record an effect of pre-operative oral nutritional supplementation on the rate of post-operative complications in patients undergoing colorectal surgery. Although the pre-operative phase might be a window of opportunity to improve the nutritional status of the patients, a clear-cut recipe for pre-operative nutritional enhancement in colorectal surgery has not been defined. Nevertheless, on the basis of the limitations of this review and the studies included, several suggestions can be made to improve the quality of future research in this field.
The number of studies was restricted, and the overall methodological quality was only moderate. A meta-analysis was precluded in some cases because of the restricted amount of data available or the clinical and methodological heterogeneity among studies. Prehabilitation as an intervention has been gaining momentum only in recent years, which limits the amount of evidence available. Furthermore, considering the fact that more than 50% of colorectal cancers are diagnosed in patients older than 65 years [2], the scarcity and the small samples could also be explained by the fact that only 7% of all trials worldwide specifically target older patients [30].
With regard to inclusion criteria, patients who would most likely benefit from a nutritional intervention were not well represented in the studies. The patients were relatively young (<65 years) and in a good nutritional status (rates of malnourishment were generally low, and the average BMI was well within the recommended range for older people). Burden et al. suggested that patients who have been losing weight pre-operatively could best profit from pre-operative nutritional support [22]. Indeed, malnourishment increases the risk of post-operative morbidity in patients undergoing colorectal surgery [31]. However, traditional measures of malnourishment, such as weight loss and low BMI, do not capture the whole picture. Instead, the deficits might be subtler. “Sarcopenia” refers to a low skeletal muscle mass that results from age-related impaired protein turnover [32]. It is exacerbated by inadequate protein intake and a sedentary lifestyle [33]. The loss in lean body mass can be masked by excess fat tissue on the scale, which is illustrated by the fact that the majority of sarcopenic colorectal cancer patients are overweight or obese (34]. Sarcopenia is accompanied by declining muscle strength and reduced functional capacity [32], and sarcopenic patients have a higher risk of complications after colorectal surgery [7,35–37]. Sarcopenia is readily diagnosed by measuring grip strength or by a standard pre-operative computed tomography scan [6,38]. Targeting sarcopenic patients and improving their nutritional status with a focus on protein intake might decrease post-operative morbidity, but few studies so far have included measures of sarcopenia in the baseline assessment.
There are certain pitfalls when it comes to the design of the intervention. Most studies provided the patients with a liquid supplement consisting mostly of carbohydrates. However, as patients at risk do not necessarily have an absolute poor caloric intake but rather a relative protein deficiency, enhancing protein intake could be the key to successful recovery. The ESPEN guidelines recommend a daily protein intake of 1.2 g/kg [11]. In most of the studies examined, it was not possible to determine whether these requirements were met, as only three of them provided information on the baseline caloric and protein intake of the patients [22,24,25], and most provided an identical amount of supplement [21–23,25,26]. Only Gillis et al. calculated the protein deficit of the patients and provided them with an amount that should cover the deficit [24]. Furthermore, the fact that patients were asked to consume up to a liter a day of an artificial supplement might have decreased compliance. If a nutritional supplement is to become a daily habit, patients have to find it desirable. A tailor-made approach that not only considers the individual dietary requirements of the patients but also integrates the supplements into the daily routine might prove to be essential.
The mere provision of extra dietary calories is overlooking the fact that inadequate nutrition is only a part of the problem. As already mentioned, both sedentary lifestyle and poor protein intake contribute to the development of sarcopenia [33]. A combination of exercise and enhanced protein intake is the most successful strategy to increase muscle mass [39–41]. Therefore, prehabilitation programs combining nutritional supplements with exercise might demonstrate a synergistic effect that translates into better recovery. Gillis et al. and Chia et al. have shown that multi-modal prehabilitation programs involving protein supplementation and strength training can lead to a better functional recovery [42,43].
Patients are most likely to benefit from a tailor-made and multi-factorial prehabilitation approach [44,45]. However, it will be essential to deconstruct a prehabilitation program into individual elements to measure their specific attributive value. This review focused specifically on the effects of nutritional enhancement, as it is a complex intervention in itself.
Lastly, at the outcome level, the choice of a validated and relevant indicator to assess the effect of a pre-operative nutritional intervention on recovery remains a challenge. Current studies use traditional measures of recovery such as the rate of complications and LOS. Especially, LOS is influenced by many factors outside the investigator's control and may not be sensitive enough to detect an effect from a nutritional intervention [46]. Furthermore, studies often are underpowered to detect a statistical difference in the occurrence of a single complication; e.g., anastomotic leakage. From a nutritional point of view, it might be appealing to look at recovery based on a single nutritional element (such as basal-rate metabolism or serum albumin concentration). However, small changes in laboratory values have no substantial meaning for the patient. Patients undergo an operation in order to enhance their physical condition, and if recovery is to be described from the patient's perspective, an improvement in post-operative functional capacity (measured with 6MWT or Short Physical Performance Battery [47]) might be a more relevant outcome.
In conclusion, a beneficial effect of pre-operative oral nutritional support on post-operative recovery of patients undergoing colorectal surgery is yet to be demonstrated. On the basis of the observed challenges, this review offers four recommendations for future studies. First, patients at risk for poor post-operative outcomes need to be identified and targeted: old, malnourished patients are especially at risk and might benefit the most from nutritional interventions. Second, because of the limited results of nutritional interventions alone, the effects of a combination of nutrition and exercise in the setting of a multi-modal prehabilitation program should be investigated further. Third, outcomes should be measured with validated tools from a perspective that matters to the patient and that is relevant to the nutritional intervention. Lastly, as no two patients are the same, a tailor-made approach might result in greater yields. So that, in the end, food can indeed be our medicine.
Footnotes
Acknowledgments
We thank clinical librarian F van Etten for contributing to the development of the search terms.
Author Disclosure Statement
All authors state that they have no conflict of interest with regard to this manuscript.
Appendix A
Search strategy in Pubmed:
(“Abdomen/surgery”[MeSH] OR “Digestive System/surgery”[Mesh] OR “Digestive System Neoplasms/surgery”[Mesh] OR “Digestive System Surgical Procedures”[MeSH] OR bowel surger*[tw] OR bowel resection*[tw] OR abdominal surger*[tw] OR colorectal surger*[tw]) AND (“Preoperative Care”[Mesh] OR preoperat*[tiab] OR pre-operat*[tiab] OR prehabilitat*[tw] OR pre-surg*[tiab] OR presurg*[tiab]) AND (“Food”[Mesh:NoExp] OR “Dietary Supplements”[Mesh] OR “Dietary Proteins”[Mesh] OR “Nutritional Requirements”[Mesh] OR nutritional supplement*[tiab] OR food supplement*[tiab] OR dietary supplement*[tiab] OR dietary protein*[tiab] OR nutraceutical*[tiab] OR nutriceutical*[tiab] OR food[tiab] OR nutrient*[tiab] OR nutrition*[tiab])