
Abstract
Abstract
Background:
We evaluated the effects of tailoring the operative approach on major surgical site complications and outcomes in lung transplant recipients.
Patients and Methods:
Beginning in July 2013, bilateral lung transplants at a single institution were performed either through sternotomy or clamshell depending on proximity of hilar structures by computed tomography (CT), anticipated complexity, past surgical history, and surgeon experience. Patient demographics and outcomes were collected in the institution's Transplant Information Services (TIS). A major surgical site complication was defined as a sterile or infected incision requiring operative intervention.
Results:
One hundred six bilateral lung transplants (68 via clamshell and 38 via median sternotomy) were performed between July 2013 and June 2016. Median sternotomy patients were older (mean age 55 vs. 50 y, p = 0.04), and less likely to have cystic fibrosis (5 [13%] vs. 19 [28%], p = 0.21) or diabetes (5 [13%] vs. 26 [38%], p = 0.01). There was no statistically significant difference in mean lung allocation score (LAS) (45 vs. 48, p = 0.39) and body mass index (BMI; kg/m2; 25.3 vs. 24.4, p = 0.29) between the sternotomy and clamshell group. Fifteen (14.2%) patients experienced a total of 25 surgical site complications (19 major and 6 minor). No sternotomy patient had a major surgical site complication and 11 (16.2%) clamshell patients had a major surgical site complication (p = 0.01). Of these 11 patients, 5 (45%) required multiple operative revisions related to the surgical site. Freedom from major surgical site complications at three years was 100% for sternotomy patients and 80% for clamshell patients (p = 0.017).
Conclusions:
Tailoring the operative approach can reduce surgical site complications in lung transplant patients by avoiding a clamshell whenever feasible.
T
Previous studies have demonstrated the benefit of pre-operative imaging for virtual planning of cardiothoracic interventions [4,5]. Pre-operative data allows the surgeon to anticipate complexity and avoid pitfalls. In 2013 we began tailoring the exposure to the patient by considering the hilar depth and extent of pleural thickening on computed tomography (CT) imaging, surgeon experience, and patient history of prior interventions. We wanted to incorporate sternotomy as an option to potentially decrease wound complications. This resulted in two separate groups of patients: sternotomy with CPB and clamshell with CPB.
Clamshell is ideal for patients with deep hilar structures when gaining posterolateral exposure to the hilum can be important. It is also well suited for patients with peripheral scarring near the apices or costo-phrenic angles as often occurs in patients with cystic fibrosis or prior thoracic interventions. Hemostasis can be easier to achieve in these cases through a clamshell approach; this is particularly important when using CPB. Conversely, sternotomy spares the internal thoracic arteries and the lateral thoracic muscles; this theoretically improves incision healing and respiratory mechanics [1,6].
Thus, sternotomy offers the potential advantage of better incision healing and recovery at the expense of a more limited exposure. This exposure can be improved with CPB, which is often a pre-requisite for the sternotomy approach. Clamshell offers the advantage of excellent exposure at the expense of greater surgical trauma and potentially compromised incision healing. We sought to compare the outcomes of either approach with regards to major incision complications, operative events, and other short- and long-term outcomes.
Patients and Methods
Study design
This was a single-center retrospective analysis of the University of Minnesota Transplant Information Services (TIS) database, a prospective database incorporating donor and recipient variables and outcomes for all lung transplants. The database was queried for all double lung transplants performed between June 2013 and July 2016 with operative details and incision complications supplemented by the patient record. Of note some patients in this cohort received portable normothermic ex vivo lung perfusion (EVLP) using the Organ Care System (OCS) as part of either the INSPIRE or EXPAND clinical trials [7,8].
Tailored approach to surgical exposure
Beginning in July 2013, we introduced the median sternotomy to our practice if certain criteria were met. By consensus, a distance on axial CT from skin to the middle of left main bronchus (LMB depth) greater than 12 cm and/or a distance from mid-line to left lateral extent of the heart (M-Apx) greater than 10 cm were features that favored a clamshell approach (Fig. 1). In addition, it was agreed that patients with prior chest surgeries other than limited biopsies would be treated through a clamshell. Finally, radiographic evidence of excessive scar tissue would also favor the clamshell. All others were treated via sternotomy. Sternotomies were performed with full CPB to decompress the heart and access the hilum. Clamshells were also done on CPB with the exception of one patient in this cohort.
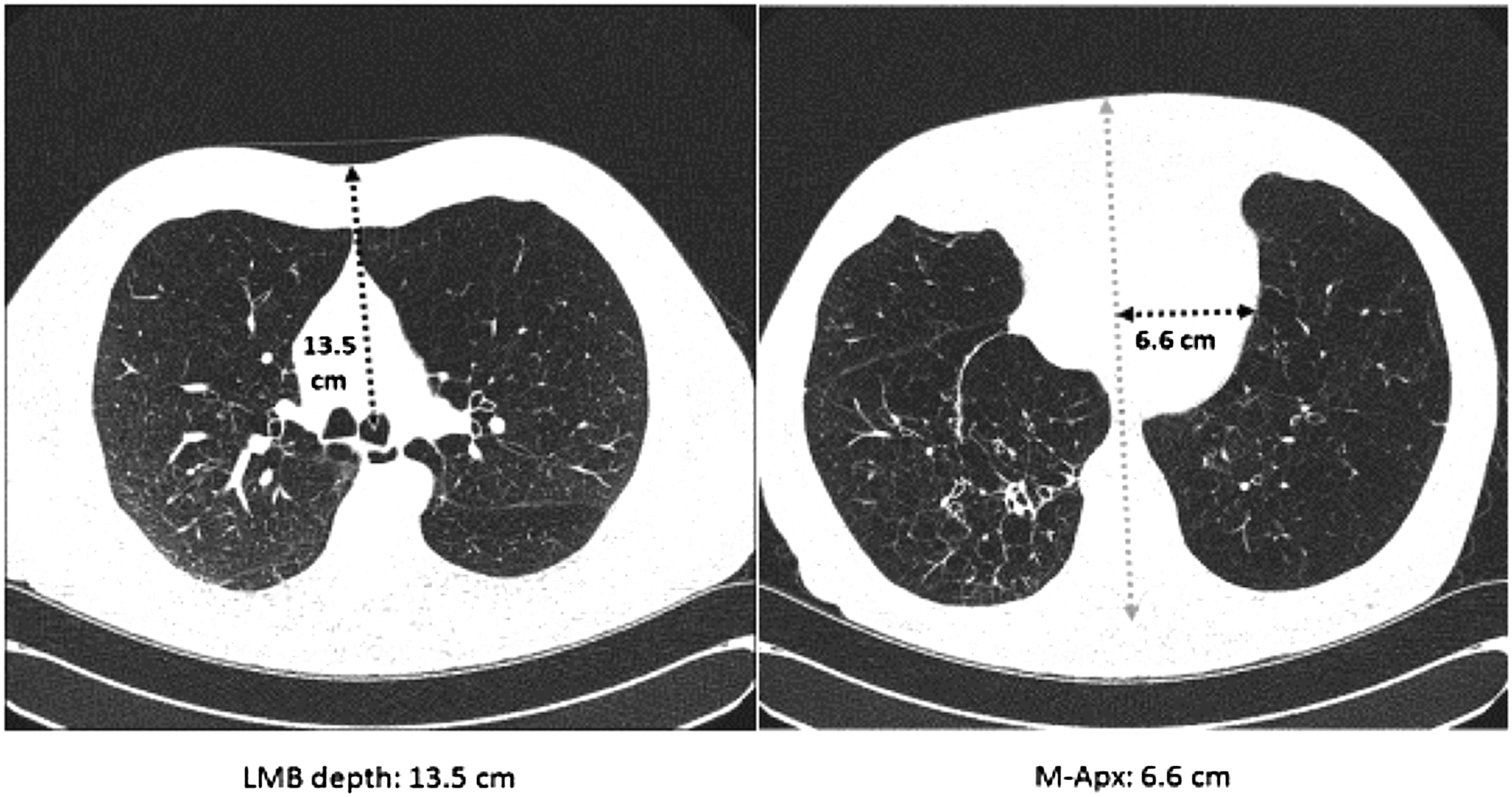
Example of pre-operative axial computed tomography (CT) measurement. Left main bronchus (LMB) depth is measured from the nearest potential point of incision to the center of the LMB. Mid-line-apex (M-Apex) is measured by the distance from the mid-line to the furthest extent of the cardiac apex. The mid-line was centered in the vertebral body and mid-line of the anterior chest wall.
Outcomes
The primary outcome was incidence of major incision complications. This was defined as any incision complication requiring return to the operating room (OR) at any time post-operatively. This included sterile necrosis, dehiscence, hematomas, or infections. Routine irrigation of patients with delayed chest closure resulting from edema, return for bleeding, or re-exploration, if not in combination with an overt wound complication, were excluded. A minor incision complication was defined as a wound during the index transplant hospitalization that was managed conservatively or with local debridement but did not require operative exploration in the OR (e.g., signs of superficial skin infection, surface wound dehiscence) as indicated in the discharge summary. Total surgical site complications describes the sum of all major and minor incision complications. Primary graft dysfunction (PGD) scores were defined according to the International Society for Heart and Lung Transplantation (ISHLT) PGD working group report by Christie et al. [9]. Our study was approved by the Institutional Review Board, which waived the need for consent from individual patients.
Statistical analysis
Variables of interest were compared between clamshell and median sternotomy patients using a t-test for continuous variables, and either a χ2 or Fisher test for categorical variables. A p value <0.05 was considered significant. A logistic regression model utilizing backwards selection was considered for the composite outcome of any incision; incision type was kept in the final model regardless of significance. Additionally, a multi-nomial ordinal model was fit for the outcome of peak PGD score. Last, Kaplan-Meier survival curves were used in conjunction with log-rank tests to compare survival time and time to first major wound following transplant. All statistical analysis was performed in SAS version 9.4 (SAS Institute, Cary, NC).
Results
Patient characteristics
One hundred six bilateral lung transplants were performed between July 2013 and June 2016, 68 via clamshell and 38 via median sternotomy. Table 1 details the differences between groups. There were more males than females in both groups. The median sternotomy patients were older (mean 55 vs. 50 y, p = 0.04) and more likely to have used portable normothermic EVLP with OCS (17 [45%] vs. 14 [21%], p = 0.01). There were more patients with pulmonary fibrosis in the median sternotomy group (17 [44.7%] vs. 19 [27.9%], p = 0.21]. Patients in the clamshell group were more likely to have cystic fibrosis (19 [28%] vs. 5 [13%], p = 0.21) and diabetes mellitus at the time of transplant (26 [38%] vs. 5 [13%], p = 0.01). Mean lung allocation score (LAS) was 48.2 for clamshell patients and 45.1 for sternotomy (p = 0.39). Mean BMI was 24.4 for clamshell and 25.3 for sternotomy (p = 0.29). Pre-admission albumin, pre-operative immunosuppression, and incidence of prior thoracic procedures were similar between groups.
COPD = chronic obstructive pulmonary disease; AAT = alpha-1 antitrypsin deficiency; IPF/ILD = idiopathic pulmonary fibrosis/interstitial lung disease; LAS = lung allocation score; BMI = body mass index; BSA = body surface area; HBA1c = hemoglobin A1c; EVLP = ex vivo lung perfusion.
Operative variables
Average LMB depth and M-Apx for clamshell and sternotomy were 11.43 cm versus 11.22 cm (p = 0.54), and 8.25 cm versus 8.34 cm (p = 0.82; Table 2). Longer mean CPB times were noted in the sternotomy group (245 min vs. 202 min, p < 0.01). There were no differences noted in mean number of blood transfusions (6 clamshell vs. 6 sternotomy, p = 0.96). In the patients receiving standard of care (SOC) with ice transportation and cold Perfadex® (XVIVO Perfusion, Goteberg, Sweden) flush, the ischemic times were longer with the sternotomy approach (407 min vs. 360 min, p = 0.03). In the EVLP group this difference was less apparent.
CT = computed tomography; LMB = left main bronchus; M-Apex = mid-line apex; CPB = cardiopulmonary bypass; pRBC = packed red blood cells; OCS = organ care system; SOC = standard of care.
Incision complications
Fifteen (14.2%) patients experienced a total of 25 wound complications (19 major, 6 minor; Table 3 and 4). There were 9 (47%) operative procedures performed for sterile major surgical site complications and 10 (53%) operative procedures performed for deep sternal surgical site infections (DSWI). No patients in the sternotomy group had a major surgical site complication but 11 (16.2%) patients in the clamshell group had a major surgical site complication (p = 0.01). Of these 11 patients suffering a major wound complication, 5 (45%) required multiple operative revisions related to the incision. On logistic regression analysis controlling for patient characteristics, the odds ratio for any incision complication was 3.88 (confidence interval [CI] range 0.8–18.85, p = 0.09) for clamshell and 1.04 (CI 1.01–1.07, p = 0.01) for LAS. An increase of one unit in LAS was associated with a 3.5% (95% CI 1%–7%, p = 0.01) increase in the risk of developing any surgical site complication after transplant (Supplementary Figure S1 and Supplementary Table S1; see online supplementary material at http://www.liebertpub.com/sur). Estimated probability of freedom from major surgical site complications at two years was 100% for sternotomy patients and 81.1% for clamshell patients (95% CI 67.9–89.2, Log-rank p = 0.0165; Fig. 2). In the clamshell group, 4 patients (5.9%) required treatment for minor complications that did not require a return to the OR, compared with 2 patients in the sternotomy group (5.3%, p ≥ 0.99)

Differences in freedom from major surgical site complications between sternotomy and clamshell.
OR = operating room; PGD = primary graft dysfunction; ICU = intensive care unit.
I&D = irrigation and drainage; VAC = vacuum-assisted closure; VRE = vancomycin-resistant Enterococcus; LIMA = left internal mammary artery; N/A = not available.
In-hospital outcomes
Differences in hospital outcomes between groups are detailed in Table 3. Incidence of peak PGD3 within 72 hr in the median sternotomy group was 39.5% versus 20.6% in the clamshell group (p = 0.04). After adjusting for covariates, incision type was not associated with increased incidence of peak PGD3. However, the odds ratio of a one hour increase in CPB time for an increase in the risk of elevated peak PGD (i.e., a score increasing from 1 to 2, 1 to 3, or 2 to 3) was 1.62 (95% CI 1.10–2.40, χ2 = 0.02) (Supplementary Table S2; see online supplementary material at http://www.liebertpub.com/sur). Mean ventilator days were 15.4 in the sternotomy group and 11.9 in the clamshell group (p = 0.48). Of patients in the sternotomy group, 7.9% returned to the OR for bleeding compared with 10.3% in the clamshell group (p = 0.69). There were no statistically significant differences in length of stay. Post-transplant pneumonia rates during the index hospitalization were similar between groups (clamshell 75%, sternotomy 68.4%, p = 0.47, Table 3).
Bronchiolitis obliterans syndrome and survival
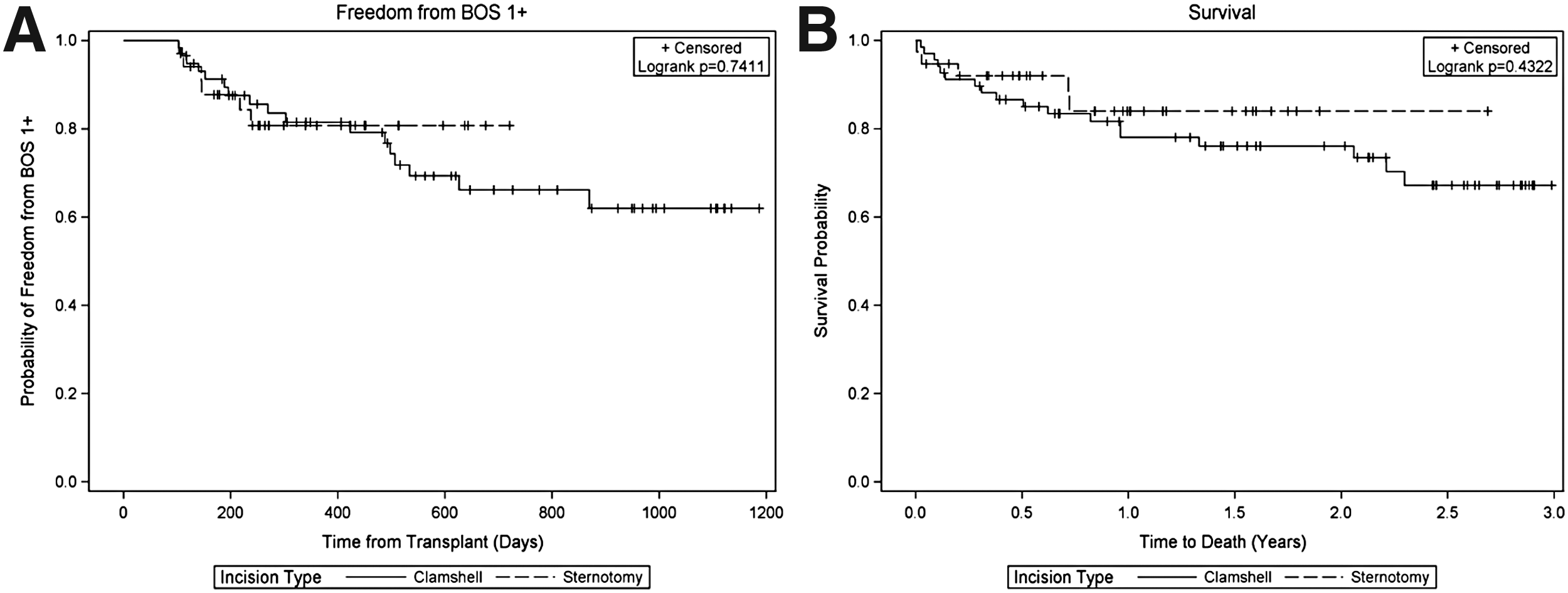
Two-year freedom from bronchiolitis obliterans syndrome (BOS) was 80% for sternotomy patients compared with 62% for clamshell (p = 0.74) (Fig. 3A). The adjusted hazard ratio for developing BOS after clamshell versus sternotomy was 1.45 (CI 0.54–3.87, p = 0.46). Only donor age was found to be significant on the adjusted analysis of this cohort for onset of BOS (HR 1.03, CI 1.00–1.06, p = 0.03); 2.5-year survival was 82% for sternotomy and 67% for clamshell patients (p = 0.43; Fig. 3B). Backwards survival selection model adjusting for patient characteristics showed no interactions in this cohort. The hazard for clamshell (versus sternotomy) in the survival model was 1.49 (CI 0.54–4.10, p = 0.44).
(
Discussion
Refinements in the technique of bilateral lung transplantation could affect both short- and long-term patient outcomes. We sought to investigate the effect of the operative exposure. Our principal findings were as follows: (1) patients who underwent sternotomy had significantly less likelihood of experiencing a major surgical site complication compared with a clamshell and (2) clamshell was associated with shorter CPB and ischemic times and potentially as a result of this, lower incidence of peak PGD3 within 72 hours.
Computed tomography imaging has revolutionized our ability to plan an operation. For example, in minimally invasive valve surgery, CT guidance allows the surgeon to determine candidacy for a minimally invasive approach and the best location for the incision [5,10]. In lung transplantation, there are several options including sternotomy, clamshell, and isolated bilateral thoracotomies. In July 2013 our program incorporated sternotomy into the armament as long as the CT imaging and other patient factors predicted that this was feasible. The impetus for this was the theoretical reduction in surgical site complications by sparing the mammary arteries as well as better respiratory mechanics.
Based on our experience we decided on anatomic thresholds (Fig. 1) that would favor one approach over the other. Sternotomy was reserved for patients with LMB depth less than 12 cm and/or M-APx distance less than 10 cm. The deeper the hilar structures are and the larger and more deviated the heart is to the patient's left, the more challenging it can be to perform the transplant pneumonectomy and the anastomosis of the bronchus, pulmonary artery, and pulmonary vein cuff. Surprisingly, the average LMB depths were only slightly deeper in the clamshell group and the M-Apx distance was actually larger in the sternotomy group. The reason for this is that several patients who were candidates by our pre-specified size criteria were not offered sternotomy because of additional factors including prior significant chest surgeries and evidence of scar tissue on CT imaging. Also, there was a tendency to offer clamshell more often to patients with cystic fibrosis because of the concern for un-anticipated adhesions. Patients with pulmonary fibrosis were more common in the sternotomy group, reflecting the relative proximity of their hilar structures to the midline and the sternum.
Analysis of our three-year experience with this tailored approach allowed us to assess the effect of exposure on surgical site complications. There were 19 major operative interventions required for surgical site complications in the clamshell group compared with none in the sternotomy group. Freedom from long-term major surgical site complications was far superior for sternotomy. The reasons for this are intuitive. The clamshell incision crosses both mammary arteries rendering the divided sternum susceptible to ischemia, infection, and dehiscence. The incidence of sterile versus infected surgical site complications in the clamshell group was similar (9 vs. 10). There were a similar small number of superficial minor surgical site complications in both groups, (clamshell, 5.9% and sternotomy, 5.3%).
The finding of large differences in major surgical site complications between groups supports our hypothesis that division of the internal mammary arteries in the clamshell incision impairs healing of the sternum and adjacent deep soft tissue, which may predispose the patient to infections. Conversely, since the superficial skin has alternate collateral blood flow, the rates of superficial minor surgical site infections were not different between groups. The rate of pneumonia was similar in both groups suggesting that the surgical approach was not as important of a risk factor. Pneumonias tend to be influenced more by the compromised immune system, inadequate bronchial clearance, and diverse donor and recipient flora. Thus, the discrepancy between rates of major surgical site complications versus minor surgical site complications and pneumonia in sternotomy and clamshell groups may be caused by loss of the predominant vascular supply to the sternum, while alternate mechanisms are likely responsible for superficial skin infections and pneumonia.
Needless to say, a return to the OR after lung transplant for a surgical site intervention affects re-admission rates and subsequent length of stay. An important contributor to the incidence of any surgical site complication was the LAS score. Thus, patients with greater acuity on the waitlist may be more susceptible to a surgical site complication; these patients should be considered for sternotomy from a healing standpoint.
Of note, although a concern of many surgeons regarding the sternotomy approach is the exposure, there was no difference in the return rate for bleeding or transfused units of packed red blood cells between groups. However, CPB times were longer in the sternotomy group. Posterior hilar exposure is more difficult with sternotomy. This can challenge both the transplant pneumonectomy and the implantation. In addition, adhesions toward the apices or toward the posterior diaphragmatic recess can take more time to dissect through a sternotomy. Also, most, if not all, of the dissection takes place while on CPB through a sternotomy. Conversely, with a clamshell and a double lumen endotracheal tube one could proceed through a fair amount of the case without CPB and, in fact, many practitioners will avoid CPB altogether.
The finding that increased time on CPB led to increased PGD in our cohort is supported by others who have found CPB to be an important risk factor for PGD [11,12]. There is an initial learning curve to doing a bilateral lung transplant via sternotomy and it is conceivable that with experience and improved patient selection alone, the bypass times can become similar to clamshell. Certain adjuncts have facilitated our sternotomy approach such as use of the self-retaining Estech® retractor (AtriCure, Minneapolis, MN) to push the hilum medially, use of a longer inferior incision, and use of the Ligasure and Aquamantys® (Medtronic, Minneapolis, MN) bipolar devices for hemostasis. Nonetheless, our data cautions the practitioner to choose the patients wisely and improve their efficiency during a sternotomy approach to limit potentially adverse graft dysfunction.
Our longer term outcomes do not suggest that there was a penalty caused by the increased time on CPB. In fact survival and BOS free survival both appeared superior in the sternotomy group, though not statistically significant. This is consistent with others who have refuted the detrimental potential of using CPB in bilateral transplant operations [13,14]. Moreover, it is conceivable that patients who undergo a sternotomy may have less of a disruption of their normal chest wall compliance and respiratory mechanics than those who undergo a clamshell. The best surrogate that we had access to was the BOS score, which factors in the patients forced expiratory volume in one second (FEV1). There was a better long-term freedom from BOS with sternotomy than clamshell, which is consistent with the potential for improved respiratory mechanics. However, there was also a greater incidence of patients with cystic fibrosis and patients with diabetes in the clamshell group. Whereas this has not been shown previously, it is conceivable that residual effects of cystic fibrosis such as the presence of multi-drug–resistant organisms played a role in the slightly increased incidence of BOS. However, the lack of difference in intensive care unit and post-transplant length of stay or ventilator days suggests that the choice of exposure does not have a meaningful impact on short-term recovery metrics.
Limitations
This study was designed to compare the effects of major surgical site complications between sternotomy and clamshell patients. The definition of major surgical site complications and the detection of such was complete and accurate from the medical record in all patients. However, the minor complications were not as easy to detect despite our best efforts. It is possible that some long-term minor surgical site issues may have been missed. The adjustment models are limited by the numbers included in this cohort and there is potential for a type II error of claiming no difference in survival or BOS when one existed. Also, other factors could have accounted for the surgical site complications; for instance, increased diabetes mellitus in clamshell patients and lower pre-operative albumin in patients with cystic fibrosis. Thus, our analysis is subject to the biases inherent to a retrospective data review. In addition, the two groups are inherently selected based on programmatic consensus but also based inevitably on surgeon preferences and bias. Nonetheless, this is the largest series addressing the question of sternotomy versus clamshell. We did not have access to other components of respiratory mechanics such as vital capacity and total lung capacity, which would have been useful for clarifying the effect of exposure on chest wall compliance. We also did not have good record of pain requirements although it is unlikely that there were major differences given the similarities in intensive care unit and post-transplant length of stay.
Conclusions
The choice of exposure is ultimately up to the surgeon and our data suggests that either clamshell or sternotomy, when properly selected, offers good exposure, equal blood loss, and similar long-term outcomes. However, whenever a sternotomy is feasible, it exposes the patient to a much lower risk of major wound complications.
Footnotes
Acknowledgment
Gabriel Loor and Stephen Huddleston receive grant support for participation in the INSPIRE and EXPAND EVLP clinical trials.
Author Disclosure Statement
The authors report no relevant conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.