
Abstract
Abstract
Background:
The burden of cardiovascular disease is increasing in low- and middle-human development index (LMHDI) countries, and cardiac operations are an important component of a comprehensive cardiovascular care package. Little is known about the baseline incidence of surgical site infections (SSIs) among patients undergoing sternotomy in LMHDI countries.
Methods:
A prospectively registered, systematic literature review of articles in the PubMed, Ovid, and Web of Science databases describing the epidemiology and management of SSIs among persons undergoing sternotomy in LMHDI countries was performed. We performed a quantitative synthesis of patients undergoing sternotomy for CABG to estimate published sternotomy SSI rates.
Results:
Of the 423 abstracts identified after applying search criteria, 14 studies were reviewed in detail. The pooled SSI rate after sternotomy among reviewed studies was 4.3 infections per 100 sternotomies (95% confidence interval [CI] 1.3–6.0 infections per 100 sternotomies), which is comparable to infection rates in high-human development index countries.
Conclusions:
As the burden of cardiovascular disease in LMHDI settings increases, the ability to provide safe cardiac surgical care is paramount. Describing the baseline SSI rate after sternotomy in LMHDI countries is an important first step in creating baseline expectations for SSI rates in cardiac surgical programs in these settings.
A
Prevention efforts directed at CAD in LMHDI countries often focus solely on medical interventions such as anti-platelet therapy, beta blockade, and rarely thrombolysis [2]. Revascularization of ischemic myocardium, however, has been shown to be more effective for the management of acute myocardial infarction and resultant cardiovascular death [6,7]. Unfortunately, coronary artery bypass grafting (CABG)—an essential surgical component in the management algorithm for CAD—is often overlooked as a potential therapeutic modality because of misperceptions of cost, availability, and technical feasibility. Yet there is widespread interest in, and urgent need for, developing this capacity in LMHDI countries [8–10].
Surgical site infection (SSI), an infrequent but potentially devastating complication of performing a sternotomy, remains an important benchmark by which to gauge quality of cardiac surgical care [11–20]. As the capacity to provide complex cardiac surgical procedures improves in LMHDI countries, tracking SSI rates will be essential for ensuring quality care.
Methods
We performed a systematic literature review of existing literature describing the epidemiology and management of SSIs after sternotomy in LMHDI countries. This review was prospectively registered in the Prospero database (Project number 42016036658) in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. PubMed, Ovid, and Web of Science databases were searched using the terms “sternotomy” or “coronary artery bypass” both alone and in combination by country listed by name (see Supplementary Material 1 for search strategy; see online supplementary material at ftp.liebertpub.com/sur). Countries included in the search were those recognized as LMHDI by United Nations Development Programme (UNDP) 2015 [21]. The LMHDI designation is a composite index focusing on three dimensions of human development: Life expectancy at birth, mean year of schooling and expected years of schooling, and gross national income per capita [21]. Inclusion criteria included any randomized, non-randomized, case-control, cohort, or demographic studies published between January 2000 and March 2016 so as to obtain the most recent and relevant information. Translation of studies not written in English was performed using Google Translate.
After initial search, titles and abstracts were screened for eligibility. Eligible articles were independently assessed by blinded reviewers who evaluated each study by pre-established criteria. These criteria included: Study duration, location, type of study, study size, age, gender, indication for sternotomy, frequency of SSI, grade of infection, micro-biologic profile, associated morbidity, death, and cost of infection. Articles were categorized into observational epidemiologic studies, cohort or case-control studies, and randomized trials. Any disagreement between reviewers was resolved through discussion with a third reviewer. Exclusion criteria included case reports, abstracts without available full-text articles, and articles describing only pediatric cardiac surgery. A pediatric patient was defined as a patient ≤18 years of age. Missing data were requested from study authors and incorporated when possible. Additional studies were sought by examining the bibliographies of all studies identified during the search process.
We used established superficial, deep, and organ space SSI definitions as the gold standard definition of infection [22,23]. Deep and organ space infections were combined for analysis. For the qualitative synthesis, we set no minimum number of patients per study, because we did not expect to identify many articles. For the quantitative pooled infection rate analysis, we excluded studies with fewer than 30 patients in concordance with the rule of three sample size. Articles describing studies in unique subpopulations were identified and described in the qualitative analysis.
Because of the heterogeneity of operations that involved sternotomy, only those studies in which the majority (>50%) of the patient population underwent sternotomy for CABG were included in the quantitative analysis to optimize similarities between patients' pre-surgical co-morbid state as well as the physiologic insult of the procedure. Pooled infection rates were sample-weighted. A priori, a study was required to report both the odds ratio and the 95% confidence interval to be included in the risk factor analysis. Because of the heterogeneity between studies and risk factors and discrepant definitions, odds ratios were not pooled. Statistical analysis was performed using STATA® (Version 14.1). This was an Institutional Review Board exempt study because all articles were available publically.
Results
There were 423 abstracts identified after applying search criteria (Fig. 1). After duplicate records were removed, 352 abstracts remained. Of these abstracts, 233 abstracts were excluded for non-relevance. Complete articles were obtained for all 119 remaining studies, and 105 were excluded because of the following reasons: No SSI data were reported, only HIV+ patients were included, data overlapped with another study, no sternotomies reported, only pediatric patients evaluated, no full text available, or study did not evaluate LMHDI populations. Fourteen full text articles met all inclusion and exclusion criteria and were used for the qualitative analysis [8,24–36]. These studies are included in Table 1.
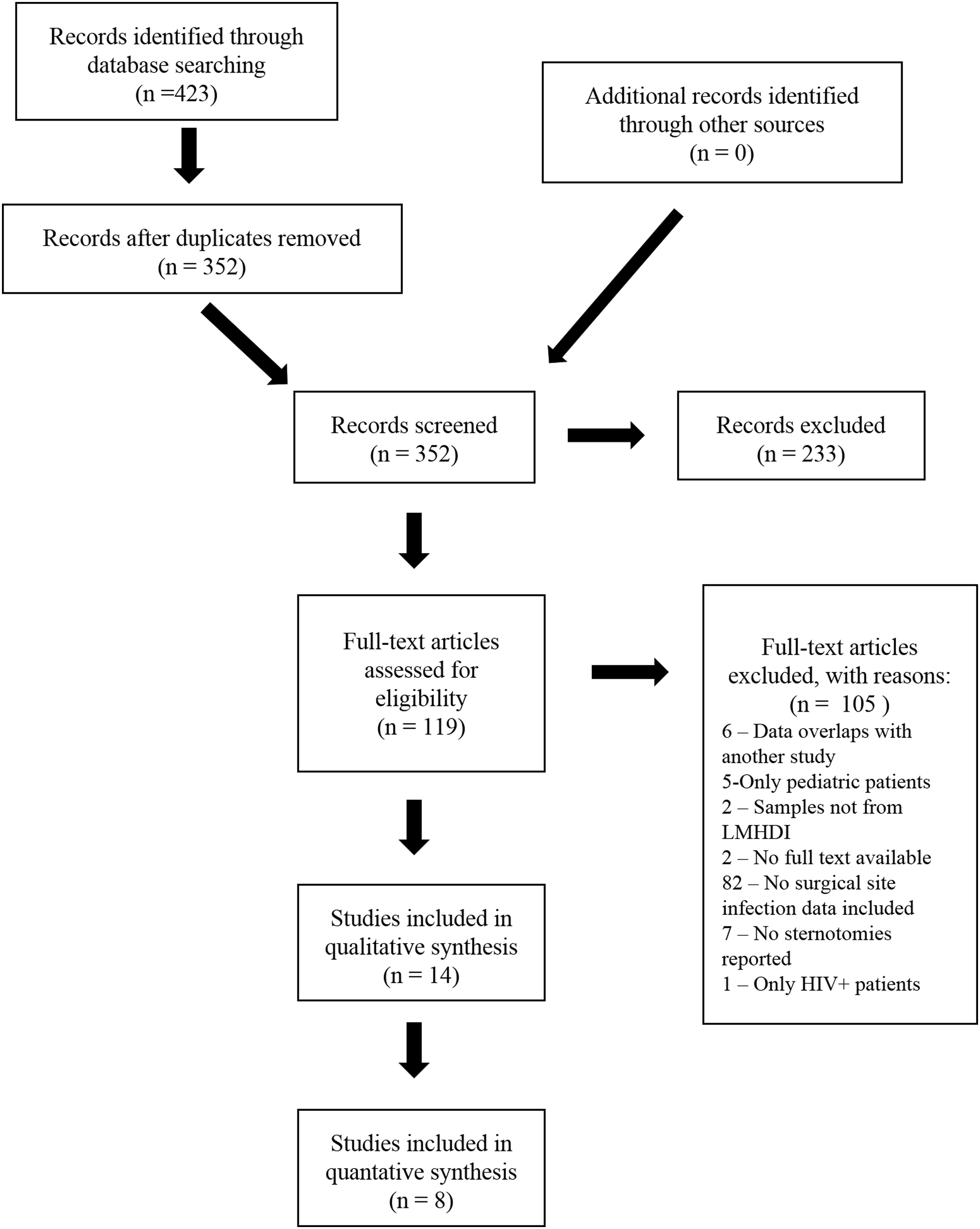
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowsheet of article selection process. LMHDI = low- and middle-human development index; HIV = human immunodeficiency virus.
CABG = Coronary artery bypass graft; N/R = Not recorded.
Indicates studies that were not included in the quantitative analysis for reasons: ≤ 50% of sternotomies performed for CABG and sample size ≤ 30.
Of the remaining 14 studies, nine (64%) were observational, one (7%) was a case control study, and four (29%) were randomized trials. More than half (n = 8) of studies were performed in Eastern Mediterranean countries, two (14%) in African countries, three (21%) in Southeast Asian countries, and one (7%) was performed across multiple World Health Organization (WHO) regions. Notably, the article by Rosenthal et al. [26] describing cases across multiple WHO regions contained the greatest number of cases of any included in this review. All but one study reported single-institution results.
Five (36%) studies focused exclusively on patients undergoing CABG, four (29%) included any cardiac procedure necessitating sternotomy, two (14%) included only patients requiring valvular surgical procedure, and single studies each described sternotomy for adult congenital disease, trauma, and thymectomy, respectively. Of the four studies describing any cardiac procedure necessitating sternotomy, three had patient populations in which 50% or more patients underwent CABG. Six (43%) studies provided definitions for what they considered SSIs in their Methods sections, and eight (57%) specified that peri-operative antibiotic agents were used. No studies described the impact of cost of care as a result of SSI, nor did they describe any secondary infections acquired as result of treatment for the initial SSI.
Of these 14 studies, eight (57%) were included for quantitative analysis because they involved entirely or primarily patients undergoing CABG [26,28,29,31,32,34–36]. A total of 39,433 sternotomies were performed with a median 266 sternotomies (range: 60–36,057 sternotomies) per study; of the five studies that reported gender data, sternotomies were performed on 1,723 (72%) males. A total of 1,698 SSIs were reported with a median 11 SSIs (range: 1–1615 SSIs) per study; this corresponds to a pooled, weighted, infection rate of 4.3 infections per 100 sternotomies for CABG (95% confidence interval [CI] 1.3–6.0 infections per 100 sternotomies). Six of the eight studies differentiated between superficial, and deep or sternal wound infections, and in these studies, 57 (75%) SSIs were superficial. Only two infections were reported as fatal in studies where this information was available, resulting in a pooled, weighted infection fatality rate of 0.02 per 100 SSIs (95% CI 0–0.3 fatal cases per 100 infections). Only one study described odds ratios for infection, so no pooled risk factor analysis was possible.
Discussion
In high-human development index (HHDI) countries, general SSI rates among patients undergoing sternotomy range from three to seven infections per 100 sternotomies [15,18,20]. The pooled overall SSI rate seen among the studies in our analysis was 4.3 per 100 sternotomies, a rate within the range described in HHDI settings. The epidemiologic transition of disease occurring in LMHDI countries is occurring rapidly, and the burden on the healthcare systems will be profound [1,2]. Developing safe and effective cardiovascular surgical procedures now is important in these settings, because the burden of cardiovascular disease will increase and strain available surgical capacity.
The complex healthcare ecosystem required to safely and effectively perform cardiovascular operations represents an opportunity for establishing SSI prevention benchmarks in LMHDI settings. It is possible that the similar pooled sternotomy SSI rates observed in LMHDI countries and HHDI countries are an indicator of the health of the complex healthcare ecosystem required to safely navigate a patient through cardiac surgical procedures. Of the infections described in the LMHDI settings, 75% were superficial SSIs, in contrast to series in HHDI settings where superficial SSIs occurred less frequently [15]. There are several potential explanations for this observed difference.
In HHDI settings, published rates of deep sternal wound infections (DSWI) range from 0.1%–7% [15,37–42], representing approximately 50% of observed infections. In HHDI series, superficial SSIs were associated with obesity, smoking, and age, while DSWI tended to be associated with more complex and lengthy repairs necessitating transfusion, transplant, and urgent repairs in addition to the risk factors associated with superficial SSI [15,17,20,43]. Given the nascent state of cardiac surgery in some LMHDI countries, one explanation for the observed difference is that complex cardiac repair is undertaken less frequently [8]. Another possibility is that patients in whom deep or organ space infections develop are misdiagnosed or die before diagnosis is performed.
It is also possible that patients undergoing cardiac surgical procedures in LMHDI countries tend to have fewer or less severe co-morbidities. From the few comparative series available among patients undergoing CABG, however, co-morbid profiles in LMHDI settings overall appear to be similar or perhaps less favorable than in HHDI settings [29,34]. As the frequency of obesity, smoking, and hypertension increase among these populations in overburdened healthcare systems, the patient risk profile of persons undergoing cardiac operations likely will worsen.
Regardless of the underlying cause for SSI in LMHDI countries, opportunity remains for improvement in preventing and managing SSIs. Bundled care packages and checklists represent a low-cost method of improving cardiovascular surgical care and have been shown to be effective in LMHDI settings [15,42,44–46]. In 2012, the Society of Thoracic Surgeons (STS) expanded participation in the STS National Database to international partners, providing cardiac centers worldwide the opportunity to integrate their cardiac surgical outcomes and benchmark their institution's outcomes against those in “like” practice environments [47]. Importantly, adherence to these protocols in the complex cardiac healthcare environment may have important trickle-down effects on the implementation of these principles in other surgical settings that are traditionally less resource intensive [45,48].
Another benefit of reducing sternotomy SSIs in LMHDI settings is a decreased cost to the healthcare system. In HHDI settings, the increased cost and length of stay associated with sternotomy SSI are nearly three-fold that of an operation without SSI [16,49–51]. Unfortunately, none of the studies reviewed in this meta-analysis reported cost-of-infection data, so no cost comparison could be made between HHDI and LMHDI settings. This information represents an underreported and underutilized variable that is important to include in future studies from LMHDI countries, particularly as future studies seek to understand or justify the cost-effectiveness of cardiac surgical interventions in these LMHDI settings. A consortium of institutions performing cardiac care in LMHDI countries might be well suited to perform a wider-ranging epidemiologic assessment of the burden of SSI after sternotomy that incorporates cost-of-care data [26].
National investment by LMHDI countries in cardiac care referral centers might have positive secondary benefits. Only 14 studies describing SSI after sternotomy were identified over a 16-year period in LMHDI countries, suggesting that a considerable deficit exists in the availability of cardiac surgical care. The infrastructure required to start and maintain a comprehensive cardiac center is great and is frequently cited as a justification as to why establishing such centers should be avoided. The high upfront cost investment in such centers, however, might have widespread downstream positive impact on the ability to deliver high quality surgical care as a whole in LMHDI countries beyond the immediate scope of cardiovascular surgical procedures [52]. The ability to triage ill cardiac patients, perform rapid cardiac diagnostics, store and deliver blood products, care for critically ill patients, and develop close collaboration between anesthesiologists, surgeons, and nursing staff may have far reaching impacts throughout the healthcare system [52].
Another secondary benefit is promoting confidence in national healthcare systems, because having a safe and functioning cardiovascular care referral center may build the confidence of both national physicians and the public [8,52]. An example of such a case is Narayana Health in India, which has demonstrated remarkable resiliency, outcomes, and cost savings in a LMHDI setting [53]. Finally, development of cardiac care centers represent an opportunity for longitudinal, capacity-building collaborations between physicians and surgeons among LMHDI countries and those in HHDI countries outside of the “medical mission” model [8].
There are several limitations to this review. First, there is likely publication bias among the reported studies from LMHDI countries. It is possible that surgeons and centers with higher SSI rates chose not to publish their results. Second, several of the studies did not delineate between superficial, deep and organ space infections, or provide reported definitions for SSIs, limiting comparisons between studies. Third, only one study evaluated risk factors for infections, so pooled risk factor analysis was not possible. Fourth, only a small subset of the 83 LMHDI countries was included in this review, and only two studies described series occurring in sub-Saharan Africa. This limits extrapolation of the results for other LMHDI settings.
Fifth, sample sizes for the studies tended to be small and may be underpowered collectively to provide accurate infection rates. We attempted to limit this by performing a subanalysis of studies with ≥30 patients, but this could still bias our sample. Because of the relative low study populations of many of the studies, findings from studies of larger patient populations biased calculated infection rates. Specifically, the study performed by Rosenthal et al. [26] had a substantially larger n-value than the other reviewed studies. Finally, the Rosenthal et al. [26] study included saphenous vein graft donor site infections in the number of infections reported for CABG, which may have led to an overestimation of sternotomy infection risk in that study [54].
As the burden of cardiovascular disease increases in LMHDI settings, the ability to provide safe cardiac surgical care is paramount. An essential component of providing this cardiac surgical care is understanding and defining an acceptable baseline for SSIs in these settings. Monitoring, accurate data collection, and prompt reporting are essential to developing an actionable SSI surveillance program. Among reviewed studies, sternotomy SSI rates were comparable between LMHDI countries and HHDIs, suggesting that adherence to rigorous healthcare bundles, such as those seen in cardiac operations, may make obtaining equivalent SSI rates in LMHDI countries a possibility.
Footnotes
Acknowledgments
The authors would like to thank Dr. Jack Boyd for his review of the article.
Author Disclosure Statement
No competing financial interests exist.
The views expressed in this article are those of the authors and do not necessarily represent their affiliated institutions.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.