
Abstract
Abstract
Background:
Pilonidal disease is a common and painful disorder that can be challenging to manage. Recurrent surgical treatment is often warranted and may result in significant morbidity, with reported wound complication rates as high as 30%. Laser hair depilation of the natal cleft may decrease the incidence of recurrence. The purpose of this study was to assess the safety and tolerability of laser hair depilation in adolescents with pilonidal disease.
Methods:
We performed a prospective, single arm, pilot trial of laser hair depilation to the natal cleft in 13 patients with pilonidal disease. Each patient received an outpatient laser depilation treatment every four weeks with a goal of five total treatments. Follow-up tolerability was measured after each treatment by obtaining Likert scale, patient-reported, pain scores immediately after laser treatment and every six hours post-treatment, for the first 24 hours. Consistent pain scores <4 were used as a proxy for tolerability. The primary end point was tolerability and safety, defined as pain scores consistently <4 and no deep second-degree burns during the 24-hour post-treatment period. The secondary end point was disease recurrence at one year.
Results:
Thirteen patients were enrolled with 12 patients completing five laser depilation treatment sessions and one patient completing only four. There was 100% tolerability of treatments with no occurrence of second-degree burns. No patient was unable to complete a treatment session because of discomfort. Significantly diminished hair growth was noted after three treatments. All 13 patients were recurrence-free at a median follow-up of 13 months post-treatment initiation.
Conclusions:
Laser hair depilation is safe and well tolerated in adolescents with pilonidal disease and may be effective at decreasing pilonidal disease recurrence. A prospective randomized controlled trial is planned to determine effectiveness of laser hair depilation compared with chemical/mechanical depilation methods in preventing pilonidal disease recurrence.
P
Adjunct treatments to prevent recurrence of pilonidal disease are largely dependent on thorough hygiene to the affected area and hair removal by shaving or chemical depilation. The American Society of Colon and Rectal Surgeons recommends that the skin in the buttocks crease be shaved or chemically depilated every 2–3 weeks until the age of 30 to prevent recurrent pilonidal disease [5]. Unfortunately, hair removal through mechanical (shaving) or chemical depilation is not always an adequate treatment for this disease, with many patients having recurrence. Because of the wound location, slow healing, foul smell, and pain, constant care of the infected area is critical to help abate chronicity and recurrence [3]. The chronic nature of pilonidal disease can lead to prolonged dependence on caregivers, long-term disability, reduced quality of life, and social withdrawal [6–11].
Laser hair depilation may be an effective non-invasive adjunct treatment that can reduce pilonidal disease recurrence. Several adult studies have demonstrated that laser hair depilation can reduce pilonidal disease recurrence by as much as 10%–40% compared with standard care. Data on the tolerability and effectiveness of laser hair treatment in adolescents with pilonidal disease are limited, however. The purpose of this study was to examine the safety and tolerability of laser hair depilation in adolescents with pilonidal disease and to determine its initial efficacy to prevent disease recurrence.
Methods
After obtaining Institutional Review Board approval (IRB #16-00104), we performed a prospective single arm pilot trial of laser hair depilation to the natal cleft in patients with pilonidal disease. Patients were identified after having been seen in our pediatric surgery clinic and pilonidal disease was diagnosed. They were approached during their clinic visit, and informed consent and assent were obtained. Patients with an acute abscess or infection were excluded. Each patient received a scheduled outpatient laser depilation treatment every four weeks with a goal of five total treatments.
During each treatment session, the natal cleft was shaved, and a topical anesthetic agent of 7% lidocaine/7% tetracaine was applied and removed after 45 minutes. Subsequently, laser depilation to the natal cleft with an appropriate wavelength laser for the patient's skin type was performed. An 810 nm wavelength Lightsheer laser (for Fitzpatrick skin types I–IV) and neodymium:yttrium aluminum garnet (Nd:YAG) Gemini laser (for Fitzpatrick skin types V–VI) were used because of different skin types having varying absorptions of light wavelengths.
Initial follow-up was performed to assess the tolerability of each laser treatment; pain scores were recorded immediately after treatment and every six hours for the first 24 hours after each treatment. The primary end point was the tolerability defined as pain scores consistently <4. Safety of the laser depilation treatments was defined by the patient having no presence of any second-degree burns immediately after the treatment and no occurrence of second-degree burns during the 24-hour post-treatment period. Pictures of the natal cleft taken by the family at 24 hours after each laser treatment were reviewed to assess for the occurrence of a burn.
Clinic follow-up occurred on an as needed basis after the conclusion of the laser treatment sessions. All patients were contacted routinely via phone at one year after treatment initiation to assess for disease recurrence. In addition, a review of each patient's medical record at one year was performed. Summary statistics of demographics, clinical characteristics, and outcomes are presented.
Results
We enrolled 13 patients. Demographic and clinical characteristics of the cohort are shown in Table 1. Twelve patients received treatments with the 810 nm laser, and one patient received treatment with the Nd:YAG laser. All patients completed a minimum of four treatments with 12 of 13 patients completing all five treatments. One patient was unable to finish the treatment course because of scheduling conflicts with the clinic dates. Tolerability was 100% as documented by average pain scores of 2 immediately post-procedure, and no session needed to be aborted because of patient discomfort (Table 2). No second-degree burns were seen immediately after each laser treatment or observed in a picture of the body area taken 24 hours after each laser treatment. Objectively diminished hair growth was noted in these patients after three treatments (Fig. 1). All 13 patients remain recurrence-free at a median follow-up 13 months after the initiation of treatment (Table 2).
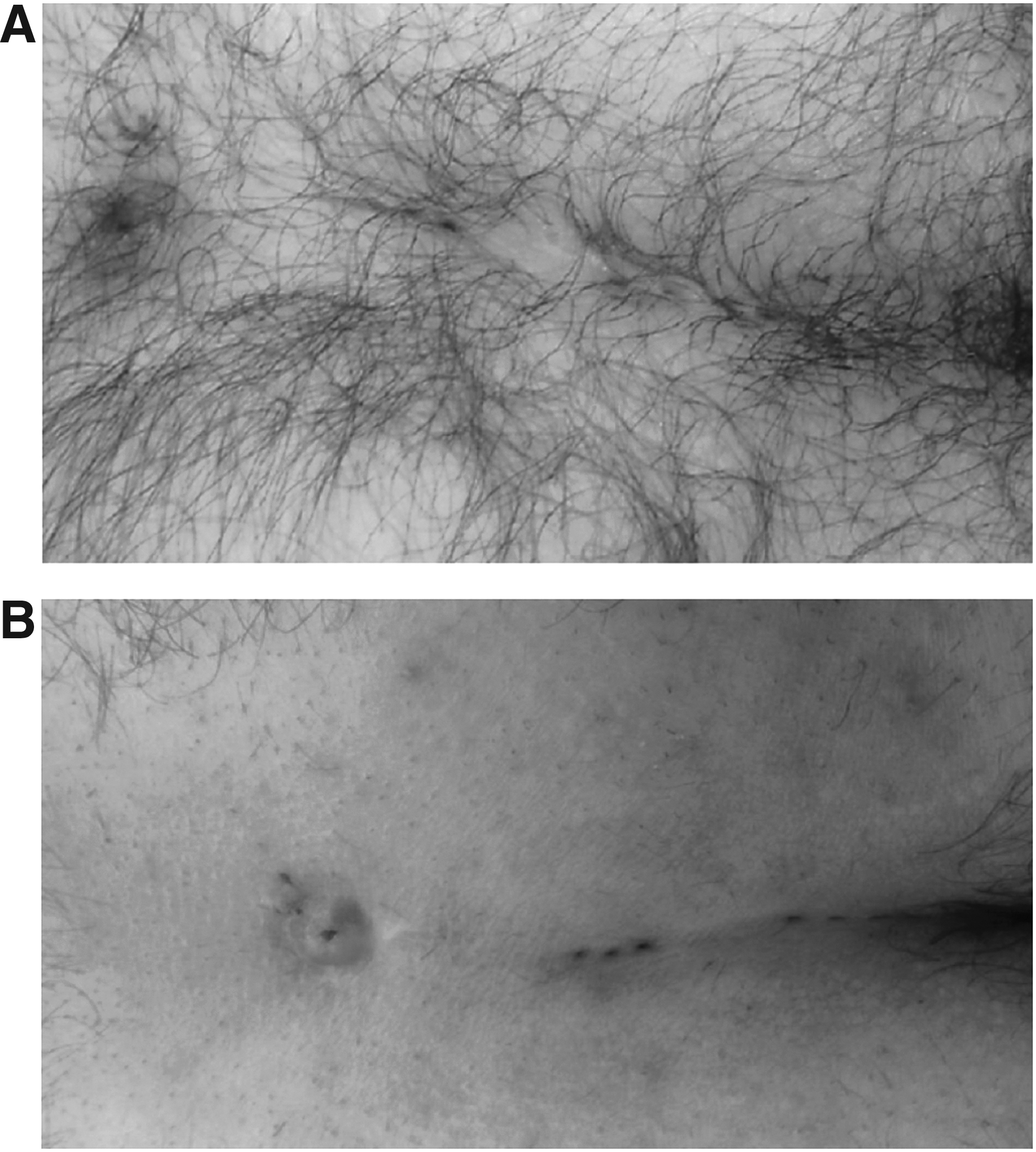
Representative pictures of natal cleft (
VAC = vacuum-assisted closure device.
Discussion
Pilonidal disease is a challenging clinical problem for patients and surgeons. As surgical excision of pilonidal disease is frequently associated with wound complications and disease recurrence, treatments that aim to minimize recurrent pilonidal disease, and potentially prevent the need for surgical excision, are needed. Our study demonstrated that laser hair depilation is safe and well tolerated by adolescents with pilonidal disease. In addition, this study suggests that laser hair depilation may be effective at reducing pilonidal disease recurrence.
Consistent with our results, laser depilation has been described in smaller retrospective and prospective adult studies as being well tolerated and describing some efficacy in preventing pilonidal disease recurrence [2,12–21]. Conroy et al. [20] examined 12 young adult patients who underwent a treatment course involving three laser treatments followed by maintenance treatments as required (mean number of treatments 3.9). All of their patients were free of recurrence at one-year follow-up, with none of them needing additional surgery. Odili et al. [12] reported a group of 14 patients treated over a five-year period with an Alexandrite laser. In their follow-up period, all patients had healed with no wound complications observed.12
Similarly, Lindholt-Jensen et al. [18] reported their experience with Nd-YAG laser use in the management of both primary and recurrent pilonidal disease. Forty-one patients underwent laser depilation treatments with a median treatment period of five months. At 15-month follow-up, 28 (76%) patients reported no wound complications after treatment, and 30 (81%) were symptom-free after supplementary laser treatment and minimal surgery (that included granuloma excision).
In adolescents and young adults, prospective data are sparse regarding the tolerability and success of laser hair depilation in pilonidal disease. Lukish et al. [4] performed a retrospective review of adolescent patients with pilonidal disease. In their study, 28 adolescents were identified. Eight patients with abscess underwent incision and drainage and then subsequent excision with delayed closure (vacuum-assisted closure [VAC] therapy), 17 patients underwent excision with primary closure, and three patients were asymptomatic and were observed. Laser depilation was well tolerated and without complication in all patients. Hair in the natal cleft was depilated in all patients. This was quantified in our study by photographic documentation. Nanni et al. [22] reported similar objective measures of hair depilation including photographic documentation, manual hair counts, and patient hair-density estimates. Patients required an average of five laser depilation treatments for adequate hair removal every four weeks. Pilonidal disease recurrence developed in one patient at a follow-up of approximately 23 months.4 The current study adds to the existing data by prospectively documenting the safety, tolerability, and initial effectiveness of laser depilation in adolescents.
Although all of the patients in this study received a diagnosis of pilonidal disease, they had undergone a variety of treatments for their pilonidal disease including various surgical procedures before their laser treatments. Therefore, despite showing the potential for overall effectiveness, the small sample size of this study does not allow us to characterize the potential effectiveness of laser depilation based on previous treatments received. A future randomized controlled trial to determine whether laser hair depilation is an effective therapy to prevent recurrence of pilonidal disease in adolescents and young adults is planned. This study will attempt to characterize the effectiveness based on previous treatments received and will also compare burden of disease and quality of life in these patients.
Conclusions
Laser hair depilation is both safe and well tolerated in adolescents with pilonidal disease and may represent an effective adjunct treatment to prevent disease recurrence. Future studies to determine the effectiveness of laser hair depilation to prevent pilonidal disease recurrence compared with chemical/mechanical depilation are planned.
Footnotes
Acknowledgments
This project was supported by intramural funding from the Research Institute at Nationwide Children's Hospital.
This project was presented at the 2017 Surgical Infection Society Meeting.
Author Disclosure Statement
No competing financial interests exist.