
Abstract
Abstract
Background:
Combat-related extremity wound infections can complicate the recovery of injured military personnel. The Enterococcus genus contains both commensal and pathogenic bacteria found in many combat wounds. We describe the patient population susceptible to Enterococcus infection, the characteristics of Enterococcus spp. isolated from combat-related wounds, and the microbiological profile of Enterococcus-positive wounds.
Methods:
Patient and culture data were obtained from the Trauma Infectious Disease Outcomes Study. Subjects were divided into a case group with enterococcal extremity wound infections and a comparator group with wound infections caused by other micro-organisms.
Results:
Case and comparator subjects had similar patterns of injury and infection. Case subjects had higher Injury Severity Scores (33 vs. 30; p < 0.001), longer hospitalization at U.S. facilities (55 vs. 40 days; p = 0.004), and required more large-volume blood transfusions (>20 units) within 24 h post-injury (53% vs. 30%; p < 0.001). Approximately 60% of case subjects had three or more infections, and 91% had one or more polymicrobial infections, compared with 43% and 50%, respectively, in the comparator group. The thigh was the most common site of Enterococcus spp. isolation, contributing 50% of isolates. Enterococcus faecium was the predominant species isolated from case-group infections overall (66%), as well as in polymicrobial infections (74%). Frequent co-colonizing microbes in polymicrobial wound infections with Enterococcus were other ESKAPE pathogens (64%) (
Conclusions:
The specific pathogenicity of Enterococcus relative to other pathogens in polymicrobial wounds is unknown. Identifying strain-specific outcomes and investigating the interactions of Enterococcus strains with other wound pathogens could provide additional tools and strategies for infection mitigation in combat-related wounds.
A
Although war wounds typically are colonized by commensal gram-positive and saprophytic gram-negative bacteria soon after injury, bacteria associated with wound infections generally are not among the colonizing organisms [9–12]. Another source of antibiotic-resistant pathogenic bacteria is the hospital, where nosocomial opportunistic pathogens have become established on abiotic surfaces, and virulent organisms disperse within and among patients [12–14]. Civilian and military hospitals alike are plagued by bacteria collectively called the ESKAPE pathogens, which have been identified as the most common and threatening pathogens. These bacteria are
Enterococcus faecium is a facultative anaerobic lactic acid bacterium that, like other species in the genus, forms small white or yellow colonies on blood agar incubated at body temperature, with or without hemolysis. Enterococcus faecium and Enterococcus faecalis are the most common enterococcal species causing infections, particularly healthcare-associated infections [16–21], but E. faecium surpasses E. faecalis in antibiotic resistance [22,23]. In recent years, a notable increase in vancomycin resistance paired with the high innate antibiotic resistance in E. faecium has resulted in restricted treatment options for infected patients [24]. Although there are data examining Enterococcus spp. with regard to healthcare-associated infections, few published studies are available evaluating the role of Enterococcus in civilian wound infections. One analysis from India on civilian trauma wound infections found that E. faecium was the most common species of Enterococcus in this type of wound, with 8% of Enterococcus isolates identified as vancomycin resistant. In addition, 9% of the infections were polymicrobial [25]. Although Enterococcus spp. often are associated with polymicrobial bloodstream and urinary tract infections [16,17], the role that enterococci play in combat trauma infections has not been investigated extensively.
In 2009, the Department of Defense and Veterans Affairs Trauma Infectious Disease Outcomes Study (TIDOS), a multicenter, observational project, began enrolling participants to investigate infectious disease outcomes in combat-injured U.S. military personnel [4]. The overarching purpose of TIDOS is to improve infectious disease outcomes in military members with traumatic injuries [4,26]. Our study utilized TIDOS data to perform a retrospective analysis to describe the injury patterns, infections, and medical treatment of military personnel with wound infections positive for Enterococcus spp. at initial diagnosis. It also describes the variety of species and resistance patterns identified among Enterococcus isolates recovered from the wound infections in these patients.
Patients and Methods
Study design
The TIDOS project includes military patients with deployment-related traumatic injuries sustained between June 2009 and December 2014 and admitted to Walter Reed National Military Medical Center (formerly Walter Reed Army Medical Center and National Naval Medical Center) and San Antonio Military Medical Center (formerly Brooke Army Medical Center) after medical evacuation from Iraq and Afghanistan through Landstuhl Regional Medical Center in Germany [4]. The study was approved by the Infectious Disease Institutional Review Board of the Uniformed Services University of the Health Sciences (Bethesda, MD).
The subject dataset for this analysis was determined by querying the entire TIDOS population for patients with at least one skin or soft-tissue infection (SSTI) or osteomyelitis diagnosis meeting the standardized National Healthcare Safety Network-infection diagnostic criteria [27] at an extremity anatomic site and with at least one positive microbiologic culture from the infection site within three days before or after the date of infection diagnosis. Demographics, injury characteristics, and treatment data were obtained from the Department of Defense Trauma Registry [28]. Infection data were collected via the TIDOS supplemental infectious disease module [4]. Body sites classified as extremities were the foot, ankle, lower leg, knee, thigh, groin, gluteal muscles, pelvis, shoulder, upper arm, elbow, forearm, wrist, and hand. The subjects were divided into groups with at least one culture positive for Enterococcus (case group) and a comparator group with at least one positive culture, but no Enterococcus isolates.
An infection dataset was created by querying all clinical infectious disease events, including, but not limited to, wound infections associated with the subjects in the case and comparator groups. If the a priori criteria were not met, an infection still was included in the analysis if there was a clinical diagnosis associated with directed anti-microbial treatment for five or more days for SSTIs and ≥21 d for osteomyelitis. Infections were excluded if an alternative diagnosis was indicated in the medical records and anti-microbial treatment was discontinued. As an individual subject could have more than one infection, the multiple infections in the dataset would belong to the same patient and were counted individually on a per-infection level. Wound infections were counted by combining the clinical diagnoses of SSTI and osteomyelitis. Polymicrobial wound infections were defined as an SSTI or osteomyelitis diagnosis associated with positive cultures for more than one organism (within three days of infection diagnosis).
The Enterococcus isolate dataset was selected by querying all bacterial isolates from the TIDOS Specimen Repository identified clinically as a species of Enterococcus and cultured from a wound or bone specimen associated with an SSTI or osteomyelitis within three days before or after infection diagnosis. A wound specimen was defined as tissue, swab, abscess, or drainage material. Anti-microbial susceptibility testing of Enterococcus spp. isolates was performed in the clinical microbiology laboratories using either the BD Phoenix automated microbiology system (Becton, Dickinson and Company, Sparks, MD) or VITEK® 2 (bioMérieux, Durham, NC) per manufacturer guidelines and interpreted in accordance with laboratory protocols and the criteria of the Clinical Laboratory and Standards Institute [29]. Culture data for the isolates were used to compare proportions of species, antibiotic susceptibilities, anatomic site of culture, and source hospital.
The microbial composition of the polymicrobial wound infections containing Enterococcus was determined. The number of unique infections associated with each co-infecting organism was counted.
Statistical analysis
Differences between the case and comparator group related to demographics, injury characteristics, infections, and treatment were evaluated. Categorical data were assessed using the Fisher exact test, the Fisher-Freeman-Halton test, or the χ2 test, as appropriate. Differences in continuous data were analyzed statistically using the Wilcoxon Mann-Whitney test.
Results
Study population
There were 155 subjects with enterococcal wound infections (SSTI and osteomyelitis) in the case group and 237 comparator-group subjects with wound infections attributable only to non-enterococcal microbes (Fig. 1; Table 1). The demographics of both groups were similar: Subjects were almost all male and predominately enlisted, although there was a small difference in rank distribution between the two groups (p = 0.030) caused by a slight increase in officers in the case group relative to the comparator group. There was no significant difference in the proportion of subjects from different branches of the service, with both groups containing primarily Marines Corps and Army personnel.
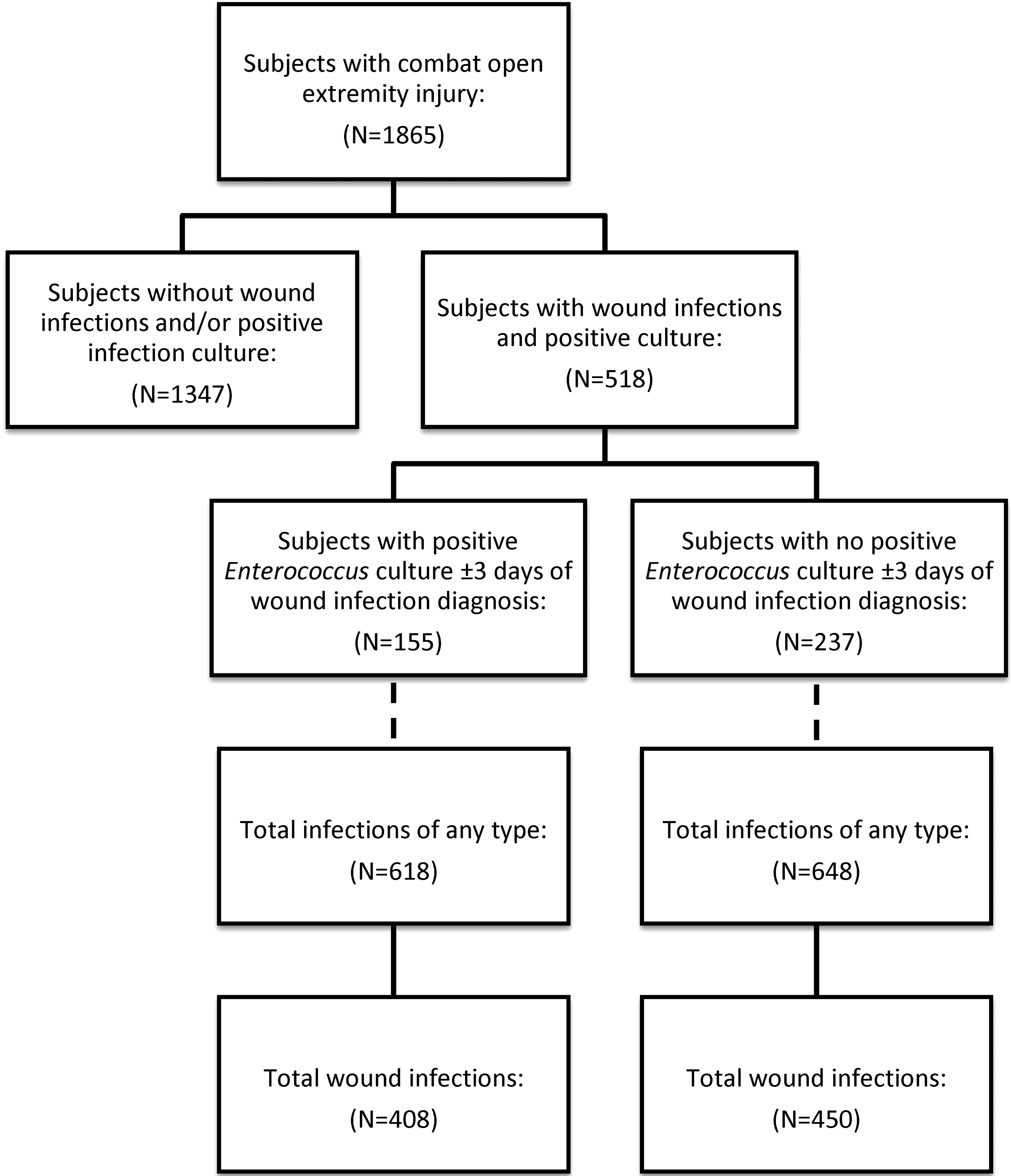
Flowchart of inclusion criteria for subjects and infections. Subjects are a subset of the Department of Defense and Veterans Affairs Trauma Infectious Disease Outcomes Study (TIDOS) population with combat-related extremity injuries and extremity wound infections (skin or soft-tissue infection or osteomyelitis). The cohort was divided into a case group of subjects with at least one Enterococcus culture associated with a wound infection and a comparator group of subjects with wound cultures positive for any other microorganism. The total number of infections and the number of wound infections were determined for the case and comparator group.
Two case subjects had surgical amputations after admission to U.S. hospitals. The remainder of the amputations occurred in the combat theater or at Landstuhl (Germany) and are considered traumatic.
AK = above knee; BK = below knee; GU = genitourinary, IQR = interquartile range; UE = upper extremity.
Injury, infection, and treatment
There were no significant differences in the injury pattern for the case and comparator subjects (Table 1). Blast injuries were predominant in both groups (95% and 93% for the case and comparator groups, respectively) with a similar proportion of subjects sustaining injuries to the upper and lower extremities (84% and 81%, respectively). Subjects in the case group had a significantly higher median Injury Severity Score (ISS) than those in the comparator group (33 vs. 30, respectively; p < 0.001). Furthermore, the case subjects had a higher rate of intensive care unit (ICU) admission (p < 0.001), received more units of packed red blood cells plus whole blood within 24 h of injury (p < 0.001), and required a greater number of visits to the operating room in the two weeks after injury (p < 0.001; Table 2). Lastly, the duration of hospitalization was longer (median 55 vs. 49 days) for the case subjects than for the comparator subjects (p = 0.004).
Within 24 h of injury.
Packed red blood cells plus whole blood within two weeks of injury.
CSH = combat support hospital; IQR = interquartile range; LRMC = Landstuhl Regional Medical Center.
Infection patterns were similar in the case and comparator subjects; however, case subjects had a higher incidence of multiple and polymicrobial wound infections. Subjects with three or more in-patient infections represented 60% of the case group, but only 43% of the comparator group (p < 0.001; Table 2). The proportion of subjects with at least one polymicrobial wound infection was significantly higher in the case group (91% vs. 50%; p < 0.001). In addition to wound infections, bloodstream infections and pneumonia contributed more than 5% of the total infections in both groups (Table 3). As the infection-level data were not independent (i.e., multiple infections from the same patient were counted as individual infections, along with infections from other patients), no statistical analysis was performed on these data.
Data are presented on a per-infection level,
Other infections: Clostridium difficile (presumptive and confirmed), eye infection, sinusitis, otitis interna, non-pneumonia lung abscess, tracheobronchitis, and undifferentiated.
Microbial isolates
The most common species of Enterococcus identified was E. faecium (66%), followed by E. faecalis (13%) (Table 4). There was one isolate identified as E. gallinarum, which was collapsed into the group of unspeciated Enterococcus (n = 53; 21%) for clarity (Table 4). Vancomycin resistance was not common among Enterococcus isolates, but did occur in a higher proportion among uncommon or unspeciated Enterococcus spp. (15%) than E. faecium (1%) or E. faecalis (0) (Table 4). Resistance to other classes of antibiotics was higher, with 52% of Enterococcus isolates resistant to at least one antibiotic in the beta-lactam class (e.g., penicillin derivatives, cephalosporins, and carbapenems) and 17% resistant to one or more antibiotics in the aminoglycoside class (e.g., gentamicin). The anatomic source of the largest number of isolates was the thigh, followed by the lower leg, pelvis, forearm, and upper arm. The majority of the Enterococcus isolates were cultured from polymicrobial wound infections (Table 4).
Includes unspeciated Enterococcus isolates and one isolate identified as E. gallinarum.
LRMC = Landstuhl Regional Medical Center.
Polymicrobial wound infections
A total of 211 polymicrobial Enterococcus wound infections were identified in the case group, and E. faecium was the most common enterococcal species cultured (74%; Table 5). ESKAPE pathogens (other than Enterococcus spp.) were co-cultured from 64% of the polymicrobial wound infections, with E. coli, E. cloacae, P. aeruginosa, and A. baumannii being the most frequent (Table 5). Bacillus spp. (20%) and Aspergillus spp. (17%) were the most common non-ESKAPE pathogens co-cultured from polymicrobial Enterococcus infections. Mold and yeast growth was identified in 35% of the polymicrobial infections.
Organism categories are the total number of infections with those organisms. Species under the categories are counted individually, so may sum to more than the total for each category. Infections are polymicrobial; they may include multiple microorganisms within each category.
Includes unspeciated Enterococcus isolates and one isolate identified as E. gallinarum.
Includes Acinetobacter radioresistans, Acinetobacter ursingii, Chryseobacterium spp., Citrobacter spp., and Ralstonia spp.
Includes Lactobacillus spp. and Vagococcus spp.
Includes Bifidobacterium spp., Eubacterium spp., Finegoldia magna, Fusobacterium spp., Peptostreptococcus spp., and Propionibacterium spp.
Includes Absidia spp., Arthrographis spp., Bipolaris spp., Chaetomium spp., Geotricum spp., Gliocladium spp., Malbranchea spp., Mycelia sterilia, Pithomyces spp., Rhizopus spp., Scytalidium spp., Trichosporon spp., and unidentified mold, yeast, and fungus.
Discussion
Wound infection is a major cause of morbidity and death and a primary concern of the U.S. Military Health System as it pursues better outcomes for personnel injured in combat. Whereas other recent studies of trauma wounds in military personnel generally have focused on the role of antibiotic-resistant gram-negative pathogens or invasive fungal infections [30–34], this study is the first targeted investigation of the incidence of Enterococcus in combat wounds. The findings indicate that patients with enterococcal wound infections had patterns of injury similar to those of patients with other wound infections but had elevated ISSs, required a greater volume of blood transfused after injury, and had a longer duration of hospitalization in the United States. Individuals with enterococcal wound infections also had more inpatient infections on average than those in the comparator group and a much higher incidence of polymicrobial wound infection.
Treatment of combat-related trauma is challenging because of the high ISS and is often complicated by the development of infections [4,5,35,36]. Because of the high prevalence of extremity trauma among combat casualties from the wars in Iraq and Afghanistan [37–39], we limited our study to subjects with combat-related extremity injuries. This pattern consists mainly of penetrating soft-tissue injuries (53%), with a large number of fractures also reported (26%) [40]. Furthermore, traumatic amputations are common as a result of explosive blasts, which were the predominant injury mechanism in Afghanistan [41–44]. Both the case and comparator groups in this study included a high proportion of blast-injured subjects with severe and complex injuries to both the upper and lower extremities. Although our study does not break out injuries based on pattern, the incidence of SSTIs and osteomyelitis is consistent with previously reported proportions of infections associated with soft-tissue injuries and fracture [14,36,45].
Despite a lack of targeted studies of the microorganism, Enterococcus has been a frequently observed gram-positive genus in wounds sustained during the wars in Iraq and Afghanistan [5,11,12]. One prospective study investigating the contribution of early wound-colonizing organisms to later infecting pathogens in open fractures detected Enterococcus in extremity wounds. Enterococcus spp. were identified in 8 of 14 wounds and in 6 of 10 patients who required amputation of at least one extremity; however, initial and early wound sampling was not predictive of future infecting pathogens [11]. Combining their findings with those reported here, Enterococcus appears to be a common early colonizer in severe wounds that may be capable of surviving alongside other pathogens, resulting in infectious complications. Nevertheless, the role of Enterococcus as an opportunistic pathogen or an incidental colonizer in the early stages of wound colonization remains unknown.
According to our characterization, Enterococcus is an organism of as much interest to the trauma infection community as other wound pathogens. There are a number of reasons Enterococcus deserves more attention. Primarily, there is the presence of commensal Enterococcus in the healthy skin and gut microbiome, the incidence of Enterococcus in polymicrobial wound infections, and the potential additive or antagonistic impacts of co-colonization of Enterococcus and other pathogenic organisms.
The high incidence of polymicrobial wound infections in subjects with enterococcal infections is perhaps the most important finding of this study. Not only is the diagnosis of polymicrobial infections challenging because of the limitations of traditional culture methods, such infections can be difficult to treat, as micro-organisms interact to create biofilms that form physical barriers, making even sensitive pathogens resistant to antibiotics [46,47]. Animal models of polymicrobial infections have shown amplified proliferation of bacterial cells, impaired wound healing, and greater virulence when two organisms co-infect a wound [48,49]. A retrospective case-control study found that the odds of infection recurrence in war wounds were 70 times greater for patients with polymicrobial infection [50]. The findings of our study emphasize the prevalence of polymicrobial wound infections in combat casualties, particularly in patients with a history of Enterococcus colonization and severe extremity injury. This contrasts with studies in the civilian trauma sector, which found much lower rates of polymicrobial wound infection with Enterococcus [25]. Further research is warranted to investigate the microbial communities of acute traumatic wounds of both military and civilian populations and to determine potential synergies between pathogenic micro-organisms in trauma wounds.
Determining the impact of Enterococcus spp. in polymicrobial wound infections is similarly difficult. There are a number of studies indicating that a mixed infection including Enterococcus could be detrimental to wound healing. In in vivo models, Enterococcus exacerbates infections by the gram-negative pathogens E. coli and P. aeruginosa [51–53]. In cases of co-infections with E. coli, a mechanism has been identified whereby E. faecalis constitutively produces a soluble, diffusible metabolite that triggers siderophore expression and increases proliferation of the E. coli even under iron-limited conditions, such as those present in a wound [53]. These studies posit that Enterococcus strains act as enablers, colonizing a wound early and facilitating infection by other, more virulent organisms. Yet the findings of other analyses have suggested that having Enterococcus in a wound might promote better infection outcomes. Specifically, as members of the lactic acid bacterial family, enterococcal species produce a variety of anti-microbial peptides (bacteriocins) with a broad range of activity against other pathogens [54–56]. Strains producing one or more of these peptides have protective, probiotic effects on pathogen control in livestock [57,58]. Moreover, in one study of combat-related wound infections, detection of enteric bacteria (e.g., Enterococcus) in a wound had a significant negative correlation with treatment failure [59]. It may be the case that the impact of Enterococcus in a wound is dependent on both the strain of the Enterococcus and the other organisms present.
In conclusion, the results of our study indicate that for the military trauma population, bacteria of the genus Enterococcus infect patients with severe injuries who require ICU admission and large-volume blood transfusions. A significantly longer duration of hospitalization also was observed with the Enterococcus case subjects. In addition, subjects with enterococcal infections have a higher incidence of multiple infections, and the majority develop at least one polymicrobial infection. Our study did include a large number of unspeciated enterococci because of inconsistencies among the laboratories regarding their speciation capability; these isolates are now undergoing further examination. Future research will include assessing various strains and lineages of enterococcal isolates with differential patient and infection outcomes, screening isolates for antimicrobial peptide genes and expression, and testing for antagonistic or synergistic interactions of Enterococcus with other pathogens (including antibiotic-resistant gram-negative pathogens) in in-vitro and in-vivo models. The role of Enterococcus in combat-related extremity wounds deserves further investigation, particularly in the case of polymicrobial infections. A better understanding of phenotypic differences in enterococcal strains and bacterial interactions between Enterococcus and other pathogens could provide additional tools for infection mitigation in combat-related wound injuries.
Footnotes
Acknowledgments
We thank the Trauma Infectious Disease Outcomes Study (TIDOS) investigators for providing input on earlier versions of this paper. In addition, we thank our collaborators on the TIDOS Multi-Drug Resistant and Virulent Organism (MDR/VO) Program, with special thanks to LTC Kevin Akers, LT Chase Watters, LCDR Mark Simons, and M. Leigh Carson. We also are grateful to Dr. Jonathan Berman of Clinical Research Management for helping to review the background research on this subject.
This work (IDCRP-024) was supported by the Infectious Disease Clinical Research Program (IDCRP), a Department of Defense program executed through the Uniformed Services University of the Health Sciences, Department of Preventive Medicine and Biostatistics. This project has been funded by the National Institute of Allergy and Infectious Diseases, National Institutes of Health, under Inter-Agency Agreement Y1-AI-5072, Military Infectious Disease Research Program, and the Department of the Navy under the Wounded, Ill, and Injured Program.
A portion of these data was presented at the 2016 Military Health System Research Symposium, Kissimmee, FL, August 15–18, 2016.
Author Disclosure Statement
No competing financial interests exist. All material has been reviewed by the Walter Reed Army Institute of Research and the Uniformed Services University of the Health Sciences. They had no objection to its publication.
The views expressed herein are those of the authors and do not reflect the official policy or position of Uniformed Services University of the Health Sciences, Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc., the National Institutes of Health or the Department of Health and Human Services, Brooke Army Medical Center, the Walter Reed Army Institute of Research, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of the Air Force, the Department of the Navy, the Department of the Army, the Department of Defense, or the U.S. Government.
All work involving human subjects was approved by the Uniformed Services University of Health Sciences Infectious Disease Institutional Review Board (IRB No. 351767).