
Abstract
Abstract
Background:
Bacterial colonization of spinal implants may cause severe complications in patients with early-onset scoliosis. Correct diagnosis and detection of microbiologic formation is crucial to prevent delayed infections caused by bacterial colonization. The purposes of this study were to estimate the rate and risk factors of colonization of vertical expandable prosthetic titanium rib (VEPTR) implants in children and to compare the different methods for detecting microbiologic formation on the spinal implants.
Methods:
We evaluated prospectively a group of 42 children with spinal deformities with an overall of 95 lengthening surgeries and applied different methods to detect potential bacterial colonization of VEPTR implants: swab of the implant, swab with culture of tissue, analysis of the removed lock, polymerase chain reaction (PCR), and confocal microscopy. Potential risk factors were evaluated.
Results:
Of 42 patients, 17 (40%) were rated positive for bacterial colonization with Propionibacterium acnes and coagulase-negative staphylococci being the most commonly found bacteria. Risk factors for colonization were increasing age, body height, and weight. The swab with culture of removed tissue yielded most positive results, whereas direct microscopy and PCR were the least sensitive detection methods. Furthermore, commonly used infectious blood parameters were inconclusive.
Conclusions:
Although the impact of bacterial colonized implants on the health of the patients is not fully elucidated, clinicians aim for prevention of microbiologic formation on implanted devices. Therefore, reliable, inexpensive, and easy to apply diagnostic tools are indispensable to detect colonization. Based on our data, the swab together with tissue culture has the potential to become the method of choice for future diagnosis.
S
A well-known problem of orthopedic surgery is implant-related infections causing complications such as post-surgical incision healing problems [8–10]. Implant-related delayed incision infections in children have been described previously [11–14] and the role of biofilm-forming bacteria as a cause for these complications has been discussed [15,16]. The ability of some bacteria to produce biofilms on artificial surfaces has been known for many years [17]. Although many of these biofilm-forming species are natural commensal bacteria of the skin [18], their ability to produce biofilms becomes a substantial risk factor in combination with implant-related surgery [19]. In biofilm formation, these bacteria are more resistant against mechanical, chemical, and immunologic destructive influences [20] and specifically against antibiotic treatment [21,22].
The spinal deformity correction in children utilizing the VEPTR system combines two major risk factors for bacterial colonization: the insertion of an implant and repeated surgeries on that implant. Previous work showed that the rate of bacterial colonization is 4.5 times higher than the rate of clinically apparent infections [23]. However, the rate of bacterial colonization for children with the VEPTR system has not been investigated sufficiently. Moreover, an established method to detect a bacterial colonization on implants is currently not available. Laboratory–chemical, histopathologic, and microbiologic examinations are not adequate to indicate possible colonization [24–27]. To improve the microbiologic examination results, sonication of the samples prior to the normal diagnostic was performed and showed higher detection rates than standard workups [28,29].
To establish a sufficient method for detecting bacterial colonization in children with titanium spinal implants, various diagnostic procedures were tested upon their detection rates. In addition to commonly used methods, such as polymerase chain reaction (PCR) and swab of the implant, we also performed confocal microscopy of a removed part of the VEPTR system and swab with culture of removed tissue.
Patients and Methods
Patient characteristics
After ethical committee approval, we conducted a prospective cohort study of 42 children (22 females, 20 males) with spinal deformity and VEPTR correction who had repeated surgical lengthening of the implant with partial implant exchange of the VEPTR lock between September 2013 and August 2015. Written consent was obtained from both the under-age patients and their parents. Ninety-five surgical interventions were performed during this study (average number of surgeries per patient, 2.3). The average age at the surgical intervention was 10.0 (± 2.8) years. The majority of patients involved was diagnosed with neuromuscular scoliosis (n = 31), whereas others had congenital (n = 8) or idiopathic scoliosis (n = 3).
Surgical technique
Expansion procedures were performed in intervals of approximately six months. All documentations were made by the same pediatric orthopedic surgeon. Patient-specific clinical data such as gender, age at each surgery, body height, weight, number of previous VEPTR expansions, pre-existing illnesses, presence of acne, and complications were recorded. Blood samples of the children were drawn to determine concentrations of hemoglobin, C-reactive protein (CRP), and procalcitonin (PCT) as well as count of leucocytes and blood sedimentation rate. During the surgical procedures, two different samples were collected usually from the right and the left side of the patients' back (alternatively medial and lateral at the same side). Single-shot intravenous antibiotic agents (second-generation cephalosporins) were administered after probes were taken. A patient was graded as positive if at least one sample showed bacteria growth in any of the surgical procedures.
Swab of implant
Sterile culture swabs were used to obtain samples from the open implant during the surgical procedures. The swabs were plunged into nutrient solution (thioglycolate) before being spread onto agar plates. The solution and the plates were cultured for three days at 37°C. Furthermore, after 48 hours additional samples of the same cultivated solutions were taken to be plated onto agar plates. If applicable, identification of bacteria was performed using matrix-assisted laser desorption/ionization (MALDI) mass spectrometer.
Swab with tissue
For the swab with tissue, the swabs together with a piece of tissue, which was routinely removed during surgical procedures, were plunged into thioglycolate. After three minutes of sonication (sonification-bath BactoSonic®, Bandelin, Berlin, Germany), the cultures were kept for 10 days at 37°C. Additionally after eight days, subcultures were started on solid agar media under aerobic or anaerobic conditions to screen for any bacterial growth.
Lock analysis
A small piece of the implant, called the lock, was removed during operation and divided sterilely into four pieces. The largest piece was placed onto an agar plate and turned over several times to enable maximal contact between the piece of the lock and the agar surface. Thereafter, it was added to thioglycolate nutrient broth and sonicated subsequently. Two additional parts of the lock were cultivated in medium (thioglycolate or brain–heart medium) without prior sonication. After eight days, subcultures were started on solid agar media under aerobic or anaerobic conditions and plates were screened for bacteria growth 48 hours later.
Polymerase chain reaction
The samples to be analyzed by means of PCR with 16S primers were taken from the thioglycolate bouillon of the first piece of the implant after sonication. Therefore, SYBR® Green PCR Kit (Qiagen, Hilden, Germany) and the Roche LightCycler® 1.5 (Roche Diagnostic Systems, Indianapolis, IN) were used with following program: 95°C for 15 minutes followed by 40 cycles of 94°C for 15 seconds, 55°C for 30 seconds, and 72°C for 30 seconds. The following primers were used: Forward (DE74): agg gag gtc atc caa ccg ca; Reverse (RW01): aac tgg agg aag gtg ggg at (Sigma-Aldrich, Steinheim, Germany).
Confocal microscopy
The fourth part of the removed VEPTR lock was analyzed for bacterial growth by using confocal laser scanning fluorescence microscopy. The piece was applied to a chambered coverslip, washed carefully several times in Ca2+/Mn2+ phosphate-buffered saline, and incubated light-protected in a dilution of 30 mcg/mL polysaccharide-staining Concanavalin A FITC-conjugate (Sigma-Aldrich, St. Louis, MO), to stabilize carbohydrates in the biofilm, and 30 mcg/mL FM4-64FX (Thermo Fisher Scientific, Waltham, MA), a fixable membrane dye to mark any bacteria. After subsequent washing, the lock was incubated in 4% paraformaldehyde for 10 minutes at 37°C, washed again, and turned with the planar part down before being mounted in Mowiol® (Sigma Aldrich) to allow inverse confocal microscopy. Imaging was performed using a Leica TCS SP5 confocal microscope (Leica Microsystems GmbH, Mannheim, Germany) equipped with a 100 × Leica HCX PL APO OIL STED objective (NA 1.40). For detection of bacterial colonization, Concanavalin A FITC and FM4-64FX were excited simultaneously at 488 nm, and detection was set to 500–600 nm and 630–800 nm, respectively.
Statistical analysis
Obtained data were analyzed statistically using the computer program Statistica 13.0 (Dell, Round Rock, TX). Statistical significance was determined by repeated-measures analysis of variance with Bonferroni post hoc t-test. p values <0.05 were considered significant.
Results
Rate of colonization and risk factors
To detect potential implant colonization, the described five different methods from surgical samples and peripheral blood tests were applied. We evaluated 95 surgeries in 42 patients. Of 42 patients, 17 (40%) were rated positive for bacterial colonization. Of all evaluated lengthening surgeries (n = 95), 30 were rated positive for bacterial colonization, of which 14 were positive in only one examination method per surgery, 8 were positive in two, and 8 were positive in three examination methods. Samples from 65 (68%) evaluated lengthening surgeries could be validated as negative for implant colonization (Fig. 1, Table 1). None of the children had a surgical site infection.

Results of samples obtained in surgical lengthening procedures (n = 95): positive result in at least one examination ( = positive) or only negative results ( = negative). Positive results could be sub-divided depending on the number of examination methods with positive results (one, two, or three methods with a positive result for bacterial implant colonization per samples obtained in surgeries).
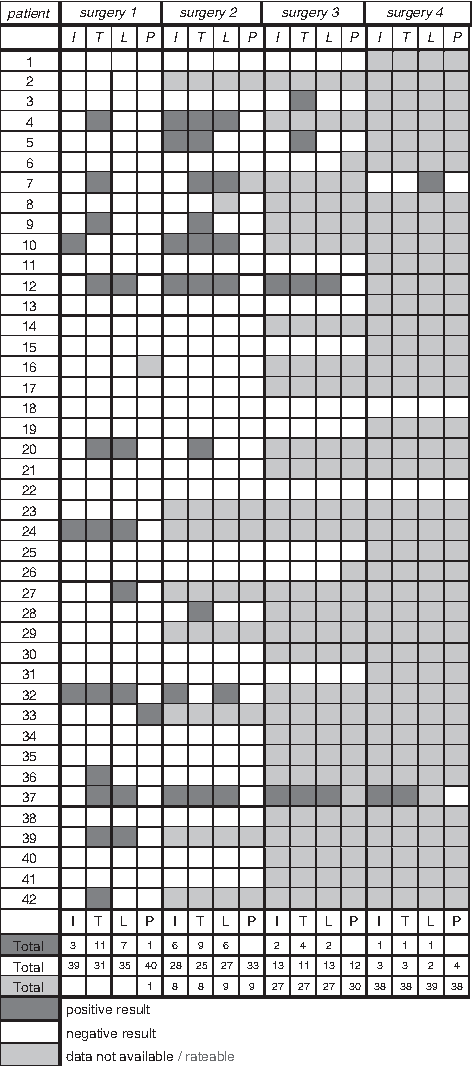
All samples obtained in surgeries are listed and divided into the four different detection methods (I = swab of implant; T = swab with tissue; L = analysis of lock; P = polymerase chain reactin [PCR]). Squares are marked as positive, negative, or not rateable for each detection method.
No significant differences were observed in terms of gender, number of previous surgeries, and previous mechanical or infectious complications in the implant area (Table 2). However, the patients with positive microbiologic results were significantly older (p < 0.001), taller (p = 0.006), and heavier (p < 0.001) than the patients with negative results. The clinical observations and the performed blood tests showed no significant difference between both groups, except for urinary tract infection (p = 0.002). At the first lengthening surgery, 9 of 42 patients showed conspicuous infectious blood parameters, but none had evidence for bacterial implant colonization.
All data given in mean with range if appropriate. Alternative patient count (n) if parameter was not applicable to all patients of the group.
Examination methods
The various diagnostic methods had different detection rates of bacterial colonization. The swab with tissue revealed the most positive results with 83% (n = 25) of all samples obtained in surgeries with at least one positive result (n = 30; Fig. 2). The analysis of the removed lock detected more than half (n = 16) of all positive samples and showed a high overlap with the analysis of tissue swabs (Fig. 3). The swab of the implant detected 40% of all positive samples and showed an overlap with the prior methods to the same extent. Polymerase chain reaction showed only a low detection rate of 3%, however, this method was not applied to all samples obtained in surgery. Also, confocal microscopy was only applied to a subset of samples revealing only poor results and thus was not pursued any further.
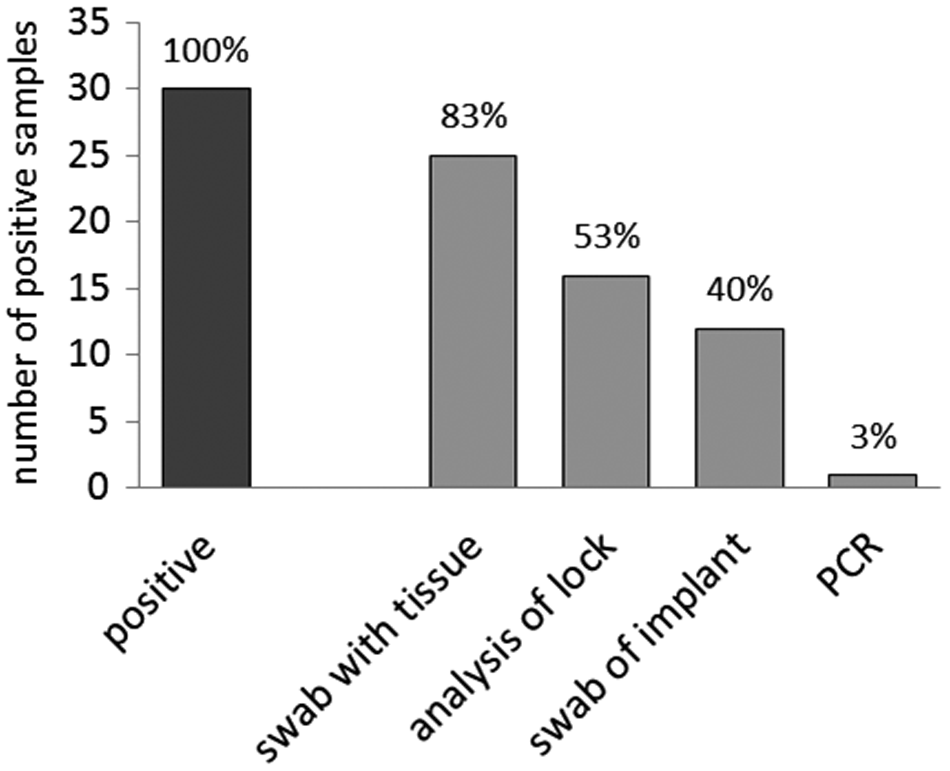
Detection rate of five different examination procedures for implant colonization. Ninety-five surgeries were screened. Positive samples could be obtained in 30 surgeries. The swab with tissue culture and the swab of implant were applied to all 95 samples, of which 25 and 12 samples, respectively, revealed positive results. The analysis of locks was applied to 93 surgical interventions, of which 16 locks were positive. Polymerase chain reaction (PCR; n = 88) yielded positive results in only one case. Percentage numbers refer to the proportion of positive results yielded with the corresponding method to the total number of positive samples (n = 30).

Venn diagram shows similar results between the different examination methods.
Figure 3 illustrates relations between the different detection methods and highlights the overlaps. Swabbing with tissue revealed the highest detection rate overlapping in the majority of cases with the analysis of the removed implant lock. Also the simple swab of the implant manifested high overlaps with the swab with tissue and the analysis of lock. The sample tested positively with PCR had no overlap with any of the other detection methods.
For all positive samples, identification of bacteria was performed with the result that propionibacteria (70%) and coagulase-negative staphylococci (47%) were the predominantly found species (Table 3). In eight cases, more than one bacteria strain was detected. Nine children had multiple positive cultures from subsequent surgeries; in all cases except one, the initially identified bacteria species remained the same during subsequent positive cultures.
Discussion
Therapy of spinal deformity in children is based on growing spinal implants such as the VEPTR. After implantation, repetitive growth-promoting lengthening procedures are required every six months. Depending on the age at first implantation a considerable number of patients will undergo surgery at the same location more than 20 times before final spondylodesis [30]. These repetitive surgeries have a high risk of bacterial implant colonization or infection. Bacteria can colonize on implants without acute clinical manifest infection, which can, however, possibly lead to a delayed incision infection over time [12]. Furthermore, colonization of the final spondylodesis implants may lead to a hazardous result with a high morbidity and mortality.
Rate of colonization
Incidence rates of delayed infection after spinal surgery are estimated between 1.7 and 8.3% [12,13,31]. In our study, we identified 17 of 42 (40%) patients as positive for bacterial implant colonization. These incidence rates are considerably higher than reported above [12,13,31]. However, our data represent the rate of implant colonization rather than the infection rate. The rate of bacterial colonization seems to be higher than the rate of clinically apparent infections [23]. Colonization of implants in patients has been proven for many instrumental systems such as hip and knee prostheses, pacemakers, breast, or spine implants [28,32–34]. This colonization often occurs without any acute clinical symptoms and their impact on long-term health of patients with populated implants remains unknown. Some studies show a higher risk of capsular fibrosis [33], implant loosening [35], pain [36], or later apparent infections upon asymptomatic colonization of implants [37]. In contrast, others could demonstrate no clinical relevance of bacterial colonized implants [32].
Propionibacterium acnes was the most common bacteria species detected in the majority (70%) of our positive examinations. Although Propionibacterium acnes is part of the normal human skin flora and is not harmful itself, it is also known to form adherent biofilms on the surface of prostheses possibly causing delayed invasive infections [16,38]. Because bacteria in biofilms are resistant to most antibiotic agents, these infections are difficult to treat and usually require surgical removal of the implants [19]. Skin flora changes in adolescence favoring growth of Propionibacterium acnes [39] may explain the high prevalence of bacterial colonization of implants with Propionibacterium acnes. In our study, the majority of children with positive Propionibacterium acnes culture had acne (57%), whereas children colonized with other bacteria species had acne-prone skin only in rare cases (13%). These and other data [40] indicate an albeit overlooked role of acne as a risk factor for contamination during surgery and subsequent bacterial colonization of the implanted devices, which should be addressed in future studies. To reduce the possible risk, measures should be adopted, for example, dermatologic treatment of patients with acne and skin preparation with antimicrobial lotion before surgery.
Other risk factors
Increased rates of bacterial colonization could be found for those patients who were older (p < 0.001), taller (p = 0.006), or heavier (p < 0.001) than negatively tested children. The average age of children in the infected group was above 12 years compared with 9 years in the group of non-colonized implants. Again, this might be because of the development of acne in puberty. Unlike other studies, we did not observe increased incidence of colonization in relation to higher numbers of previous VEPTR expansion surgerical procedures [41].
Examination procedures
To our knowledge there is no reliable gold standard procedure to detect bacteria or bacterial colonization on removed implants. Therefore, we tested various methods to compare their validity among each other. Routine diagnostics include blood and urine tests before surgery, though the value of inflammatory markers such as CRP or the erythrocyte sedimentation rate (ESR) in the diagnosis of infection are controversial [24,25]. White blood cell count and procalcitonin assays are used widely in clinical diagnostics, however, their sensitivity and specificity are insufficient to be used as individual biomarkers [42].
Consistent with other studies, we could not find any correlation between investigated blood values and bacterial colonization rate [23]. Interestingly, we could detect enhanced incidence in patients with a suspicious urine test before surgery (p = 0.002). However, because of the small number of cases, reliable information about urine tests as diagnostic tools require further investigations.
Of all methods used to detect bacterial colonization, culture-based approaches, in particular the swab with tissue and analysis of the removed lock, revealed the highest rates of positive results. Culture-based methods implicate detachment of bacteria from the implant, which may lead to incomplete acquisition of all microbiologic populated devices when bacteria are strongly adherent to the implant and swabbing is insufficient to remove them [43]. Because of the lack of a gold standard method, sensitivity of the examination procedures cannot be defined. The swab with tissue detected 83% of all surgeries with a culture-positive result. However, sensitivity might be lower or higher depending on the rate of false-positive results of the various detection methods. One indicator of high validity of the swab with tissue is given by the high reproducibility in follow-up examinations. Except for only two children, all patients diagnosed with bacterial colonization based on the swab with tissue during the first observed surgery had a second positive swab in the follow-up surgery (Table 1). In addition, the three culture-based approaches (swab with tissue, implant swab, and analysis of lock) showed high rates of overlapping results assuming reliability of these methods. Confocal microscopy and PCR indicated bacterial colonization only in individual cases excluding them as alternative detection methods. In conclusion, swabbing the implant with removal of tissue for microbiologic diagnostics is the method of choice, because it yields the most reliable results and can be performed during surgery without much effort and in a cost-effective manner.
Limitations
The advantage of our data lies in the application of various methods to detect bacterial colonization and to compare their quality between them. However, our study also has some limitations. Because there is no gold standard method to detect bacterial colonization of implants, positive examinations cannot be verified conclusively. Validity of the different proceedings could be only estimated by re-applications and comparison among them.
Furthermore, only a small part of the entire VEPTR implant, namely the lock that was removed during expansion procedures, was available for analysis. However, negative examination of the lock cannot exclude bacterial colonization of any remaining parts of the VEPTR system.
Another limitation of the current study is the sample size of children. A larger number of cases than our 42 patients with 95 observed surgeries might have yielded statistical significance of some factors, such as number of previous surgeries, that showed only trends in our study.
Conclusions
Growth-retaining implants, such as the VEPTR system, are a standard method for children with spinal deformity. Our data indicate higher incidence of bacterial colonization of these implants than initially assumed. Although the health effects of colonized implants are still under debate and require further investigations, the long-term goal should be prevention of bacterial colonization. This implies reliable methods to identify bacteria-contaminated implants. Our study suggests a swab of the implant together with examination of a removed tissue sample in contact with the implant as a cost-effective technique easy to apply during routine diagnostics. Because bacterial colonization is particularly crucial during conversion from the VEPTR system to definitive instrumental spinal fusion, in many clinics a two-stage procedure has been established in adolescence, in which the first surgery comprises only VEPTR removal, whereas instrumented final fusion is performed in a second surgery after some weeks of observation of surgical site conditions and applied antibiotic therapy if necessary. This regimen minimizes the risk of bacterial colonization of the final implant despite potential contamination of the previous growth-retaining spinal devices.
Footnotes
Acknowledgments
The authors thank Silvia Kellner and colleagues from the Department of Medical Microbiology, Goettingen, Germany, for analyzing all microbiologic samples. Confocal microscopy was performed at the Department of NanoBiophotonics, Max Planck Institute for Biophysical Chemistry, Goettingen, Germany.
Author Disclosure Statement
All authors declare that they have no conflict of interest. No funding was received, no competing financial interests exist.