
Abstract
Abstract
Background:
Wound complications remain a significant source of morbidity for patients undergoing open infra-inguinal re-vascularization. The purpose of this study was to determine the impact of several infection-control strategies on post-operative wound complications after open infra-inguinal re-vascularization.
Methods:
A retrospective cohort study was conducted among all patients who underwent an open infra-inguinal re-vascularization procedure before and after 2014. Since 2014, we have implemented strategies to reduce post-operative wound complications, including: (1) Decreasing the use of incisional skin staples, (2) increasing the use of negative pressure wound therapy (NPWT) dressings, and (3) implementing an outpatient elective decontamination protocol for methicillin-resistant Staphylococcus aureus. “Pre-era” is defined as the period between January 2012 and December 2013, before the implementation of infection control strategies; “Post-era” is between January 2015 and August 2016, after implementation. The primary outcome of interest is 30-day wound complications (infection or dehiscence). Multi-variable logistic regression analysis was used to identify significant predictors of wound-related complications between the two cohorts. Propensity score adjustment controlled for baseline patient characteristics, peri-operative variables, and surgeon experience.
Results:
A total of 338 open infra-inguinal procedures were performed: 175 in the pre-era and 163 in the post-era. Chlorhexidine skin preparation was used in the majority (321 [95%]) of cases. Comparing the periods, the post-era is characterized by a significant decrease in the use of groin staples (118 [67%] vs. 51 [31%], p < 0.001), and an increased application of NPWT dressings (6 [4%] vs. 66 [43%], p < 0.001). Thirty-five (37%) outpatient elective cases received the pre-operative decontamination protocol in the post-era. Compared with the pre-era, there was a decrease in the 30-day rate of wound complications (68 [39%] to 42 [26%], p = 0.011), and infection-related re-admissions (31 [17.7%] to 21 [12.9%], p = 0.220). When adjusting for patient characteristics, operative variables, and surgeon experience, post-era had significantly lower wound complications (odds ratio [OR] 0.33, p = 0.002) and re-operations (OR 0.16, p = 0.007). Among outpatient elective cases, the decontamination protocol was also independently associated with these two outcomes (wound complications: OR 0.05, p = 0.006; re-operations: 0.06, p = 0.002). The use of groin staples was an independent predictor of deep groin infections (OR 248, p < 0.001) and re-operations (OR 8.16, p = 0.032).
Conclusions:
Wound complications after open infra-inguinal re-vascularization have decreased significantly after the implementation of several infection-control strategies. Findings suggest that skin staples should be avoided in groin wounds, and anti-staphylococcal decontamination protocols decrease wound complications and prevent re-operations.
W
In a concerted effort to reduce infection-related complications at our institution, strategies were employed throughout the 2014 calendar year to decrease the use of incisional wound staples, increase the application of negative pressure wound therapy (NPWT) dressings, and implement a standardized decontamination protocol for methicillin-resistant Staphylococcus aureus (MRSA) for outpatient elective cases. The goal of this study is to assess the effect of these interventions on infection-related outcomes among patients undergoing open infra-inguinal re-vascularization.
Methods
Study subjects
This retrospective cohort study included all consecutive patients identified through a prospectively maintained registry of institutional operative cases—patients who underwent open infra-inguinal re-vascularization during two mutually exclusive periods before and after the year 2014. “Pre-era” was defined as the period between January 2012 and December 2013, while “post-era” was defined as the period between January 2015 and August 2016. Procedures excluded from this study were: All endovascular interventions, procedures performed primarily for carotid or aortoiliac pathology (including aortobifemoral bypasses), hybrid procedures, all lower extremity amputations without a concomitant re-vascularization procedure, and those lost to post-operative follow-up before 30-day outcomes could be assessed. The study protocol was approved by both the Baylor College of Medicine Institutional Review Board as well as the Michael E. DeBakey Veterans Affairs Medical Center Research & Development Committee. Because this was a retrospective study, the Institutional Review Board did not require informed consent from individual patients.
Primary exposure
During the 2014 calendar year, a series of interventions were implemented throughout our center to reduce post-operative wound complications among vascular surgery patients. These interventions included: (1) Decreasing the use of incisional skin staples in favor of primary sub-cuticular closure, (2) increasing the use of incisional NPWT dressings, and (3) actively implementing a decontamination protocol for outpatient elective cases aimed at reducing MRSA colonization.
These interventions were employed in addition to infection-control measures that were standard at our institution, including: compliance with the Surgical Care Improvement Program (SCIP) guidelines [16]; the use of pre-operative antibiotic agents targeted against both methicillin-resistant and methicillin-sensitive S. aureus (liberal use of vancomycin; cefazolin 1 g for patients <70 kg, 2 g for patients 70–140 kg, and 3 g for patients more than 140 kg); the routine use of 2% chlorhexidine gluconate and 70% alcohol solution (ChloraPrep,™ Becton, Dickson and Company, Franklin Lakes, NJ) for pre-operative antisepsis for intact skin surfaces [17]; and the use of an iodine-based antisepsis for open wounds. Because the three primary exposures of interest were implemented during 2014, this year was excluded from the analysis to allow for sufficient uptake and implementation by the institution.
The decontamination protocol consisted of a three-tiered approach and included the use of 2% chlorhexidine gluconate washcloths, a 0.12% chlorhexidine oral rinse, as well as a 5% povidone-iodine intranasal solution [18]. Patients were instructed to use the washcloths (applied to the neck, torso, and groins) and oral rinse the night before as well as the morning of the operation, while the intranasal solution was applied once the morning of the surgical procedure.
Outcomes of interest
The primary outcome of interest was the total number of 30-day wound complications—a composite end point defined as the number of documented SSIs or wound dehiscences between the two cohorts. Superficial and deep incisional SSIs were defined by established criteria presented by the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) [19]. Superficial wound dehiscence was defined as a separation at the surgical incision site exposing subcutaneous tissue and necessitating wound care. Deep wound dehiscence was total wound disruption as defined by NSQIP [19].
Secondary 30-day outcomes of interest included: Rates of infection-related re-admissions, infection-related re-operations, prosthetic graft infections, and groin infections. All primary and secondary outcomes were also assessed among outpatient elective procedures.
Statistical analysis
Underlying variable distributions were visualized and descriptive statistics were assessed. Continuous variables that did not follow a normal distribution were described using medians with accompanying inter-quartile ranges. Uni-variable logistic regression was used to assess unadjusted differences between the two eras. A propensity score was calculated as the probability of each open infra-inguinal re-vascularization case being in either the pre-era or the post-era. To do this, a logistic regression model was fit using the binary “era” variable (pre-era vs. post-era) as the outcome. Co-variables in the propensity score included surgeon experience as well as all other measured factors that potentially vary with time and could have therefore differed between the pre- and post-era. The inverse probability weight of the propensity score was then included in all subsequent multi-variable models in an attempt to control for baseline differences.
To identify significant differences between the eras among the primary and secondary outcomes of interest, multi-variable logistic regression models were fit using the binary “era” variable as a covariable to denote either the pre- or post-era. Of the variables not included in the propensity score, those that were significantly associated with the outcome of interest at p < 0.10 were entered as covariables into propensity score-adjusted multi-variable models using backward stepwise logistic regression. After the models were established, those in which the era variable was significant (denoting a difference between the pre- and post-eras) were then re-fit after substituting the individual components of the post-era (including: groin staples, distal staples, groin NPWT dressings, and the decontamination protocol for outpatient elective cases) for the era variable. A two-tailed p value <0.05 was considered statistically significant, and all analyses were performed using Intercooled Stata version 13 (StataCorp; College Station, TX).
Results
Descriptive statistics
A total of 277 unique patients accounted for 338 open infra-inguinal re-vascularization procedures divided between the pre-era (n = 175, 52%) and post-era (n = 163, 48%). Baseline and peri-operative characteristics, including the covariables incorporated into the propensity score are provided in Table 1. Statistically significant differences existed in the median age of the two cohorts (64.8 years for the pre-era vs. 66.4 years for the post-era, p = 0.041) as well as the proportion of cases with a history of stroke (9.7% vs. 21%, p = 0.005), both of which became equally distributed after propensity score adjustment. Of each cohort, 99.4% were male, and there were no significant differences among smoking history, mean body mass index (BMI), and proportion of patients with either diabetes mellitus or end-stage renal disease between the two cohorts.
Of each cohort, 95% received operative skin preparation with chlorhexidine gluconate before incision, and there were no significant differences in either the presenting symptom or the urgency of the index operation. Of the 95 outpatient elective cases performed in the post-era, the full decontamination protocol was administered in 35 (37%) cases. The post-era had a significantly higher number of prosthetic grafts placed (30% vs. 17% of cases, p = 0.001) and used more composite or CryoVein grafts (9.8% vs. 2.3%). Nearly 94% of all cases involved a groin incision (Table 2), for which there were no differences in the re-operative groin status of either cohort. Importantly, the post-era involved a significantly decreased use of incisional groin staples (31% of cases vs. 67%, p < 0.001), decreased use of distal lower extremity incisional staples (71% vs. 88%, p = 0.003), and increased use of groin NPWT dressings (43% vs. 4%, p < 0.001).
IPTW = inverse probability of treatment weighting; IQR = inter-quartile range; BMI = body mass index; SD = standard deviation; pRBC = packed red blood cell.
Variables used to calculate the propensity score have associated p-values before and after propensity score matching.
2 observations missing.
Primary outcome
There were a total of 110 wound complications among both cohorts, affecting 68 (39%) of cases in the pre-era and 42 (26%) in the post-era (p = 0.011; Table 3). The rate of superficial wound infections decreased from 25% to 14% (p = 0.004) across the two periods, and the rate of deep wound infections decreased from 8.6% to 4.9% (p = 0.093). There were no significant changes in wound dehiscence rates between the two cohorts. Through the propensity score-adjusted multi-variable model, the post-era remained significantly associated with decreased odds of wound complications (odds ratio [OR] 0.33, p = 0.002; Table 4), specifically including decreased odds of SSI (OR 0.19, p = < 0.001).
NPWT = negative pressure wound therapy.
IQR = inter-quartile range; PTFE = polytetrafluoroethylene.
and/or is not used in Surgical Infections. Please choose one or the other—or rewrite.
Similarly, when considering only outpatient elective cases, those in the post-era had a 57% decreased risk of having a wound complication (p < 0.001; Table 3). This association remained significant in the multi-variable model (OR 0.05, p = 0.006; Fig. 1). The rate of superficial wound infections among outpatient elective cases decreased from 33% to 12% (p < 0.001), with the rate of deep infections also decreasing from 7% to 1% (p = 0.035).
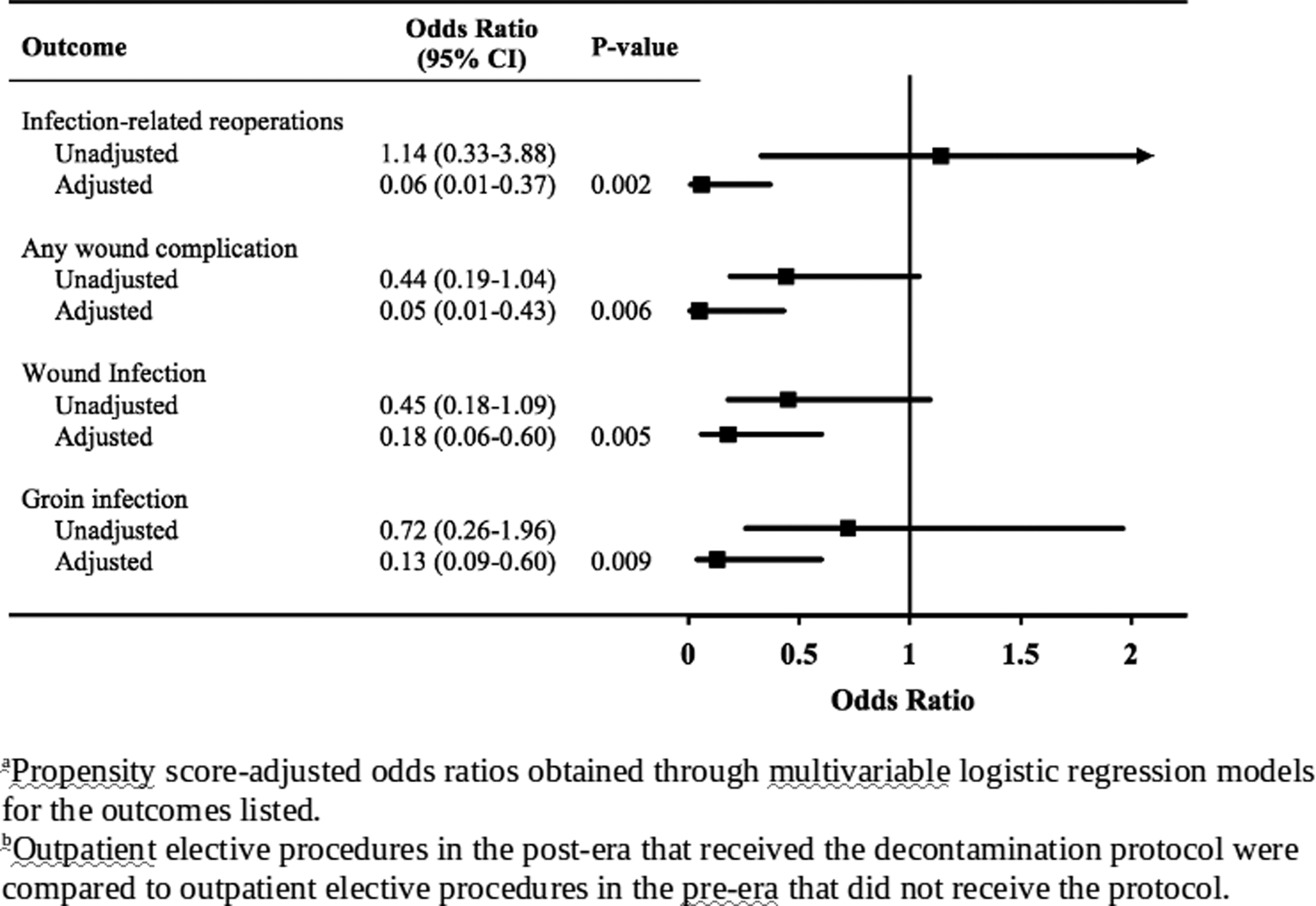
Unadjusted and adjusteda odds ratios of the decontamination protocol in outpatient elective proceduresb across multiple infection-related models.
Secondary outcomes
There was not a significant decrease in infection-related re-admissions by either the uni-variable or multi-variable models. Regardless, the cases in the post-era had a relative risk of re-admission 27% lower than the pre-era (p = 0 .220, Table 3). Further, although there was not a statistically significant decrease in the rate of infection-related re-operations in the uni-variable analysis (p = 0.104), multi-variable adjustment of confounders revealed a significantly decreased risk of re-operation in the post-era (OR 0.16, p = 0.007; Table 4).
A total of 78 procedures were performed that involved the use of prosthetic grafts. Although the rate of prosthetic graft infections decreased from 17% (n = 5) to 8% (n = 4), this was not statistically significant by either uni-variable (p = 0.271) or multi-variable analysis (OR 0.20, p = 0.204). Despite the lack of statistical significance, however, the rate of prosthetic graft infections declined by approximately 50%.
The total number of groin infections (including both superficial and deep infections) decreased from 31 (19%) to 16 (10%) over the two periods. Specifically, the post-era was strongly associated with a decreased rate of deep groin infections in both the uni-variable (p = 0.029) as well as the multi-variable adjusted models (OR 0.10, p = 0.019; see Table 5).
OR = odds ratio; CI = confidence interval.
Impact of individual post-era components on infection-related outcomes
Our analysis up to this point has looked at the overall differences between the two eras. To determine the influence of the individual components of the post-era on our results, however, the propensity score-adjusted multi-variable models were re-fit by substituting the components of the post-era for the binary “era” variable. With this analysis, the use of incisional groin staples was a strong predictor of both 30-day deep groin infections (OR 247.8, p < 0.001; Table 6) as well as infection-related re-operations (OR 8.16, p = 0.032; Table 7). The use of NPWT dressings was not associated with the outcomes studied.
OR = odds ratio; CI = confidence interval; NPWT = negative pressure wound therapy.
Compared with outpatient elective procedures.
Compared with no previous groin incision.
Compared with vein.
OR = odds ratio; CI = confidence interval; NPWT = negative pressure wound therapy.
Compared with vein.
The same analysis was then restricted to outpatient elective cases to assess the role of the decontamination protocol. Uni-variable analysis revealed no association between the decontamination protocol and the outcomes investigated. When adjusted for patient characteristics, operative variables, and surgeon experience, however, the administration of the decontamination protocol was strongly associated with a decrease in infection-related re-operations (OR 0.06, p = 0.002) and wound complications (OR 0.05, p = 0.006), including not only any wound infection (OR 0.18, p = 0.005), but groin infections as well (OR 0.13, p = 0.009; Fig. 1).
Discussion
In this study, wound complication rates and infection-related outcomes were analyzed among cohorts of patients undergoing open infra-inguinal re-vascularization before and after the implementation of strategies that effectively: (1) decreased the use of incisional skin staples, (2) increased the use of incisional NPWT dressings, and (3) implemented a standardized decontamination protocol for outpatient elective cases. Through this effort, wound complications (comprising wound dehiscences and SSI) significantly decreased by 34%. This was accompanied by a 27% reduction in infection-related re-admissions and a 44% decrease in re-operations between the two periods.
Before the implementation of our multi-tiered infection control strategy, our institution had superficial and deep infection rates of 25% and 9%, respectively (Table 3), comparable to those reported in the literature [1–6]. Since 2014, however, those rates have decreased to 14% and 5%, respectively. Similarly, the rates of deep groin infections have decreased from 7% to 2%, as the rate of prosthetic graft infections declined from 17% to 8%, all of which substantially decrease patient morbidity and also help contain post-operative healthcare-associated costs.
Our study indicates that the use of incisional wound staples in the groin is a very strong risk factor for both deep groin infections (OR 248, p < 0.001, Table 5) and re-operations (OR 8.2, p = 0.032, Table 6). The use of staples distal to the groin, however, was not independently associated with an increased risk of SSI, indicating that staples in the groin may have a higher propensity to serve as a nidus for infection. Although the relationship between staples and post-operative wound complications has been mixed and variable throughout the fields of obstetrics [20,21], orthopedics [22], and general surgery [23,24], this study provides evidence to indicate that staples should be avoided in the groin.
In addition to groin staples, other independent predictors for deep groin infections after lower extremity re-vascularization include an urgent or emergent procedure, the use of a prosthetic graft, and a history of a previous groin incision, all of which are consistent with analyses of similar cohorts of patients [4,5]. Other typical risk factors for SSIs, which include age, BMI, smoking, and end-stage renal disease, were propensity score-adjusted and were therefore not assessed individually in our models. Of note, prosthetic graft implantation in our study was also an independent predictor of 30-day infection-related r-operation (OR 6.8, p = 0.014), strengthening the evidence that supports the use of endogenous vein when available.
Similar to the use of skin staples, the data regarding NPWT dressings are also mixed with respect to preventing infections, ranging from no effect [25] to reducing groin infections by as much as 80% [26]. Although the use of NPWT dressings increased in the post-era, we did not appreciate an association with our primary or secondary outcomes of interest. This may be a result of preferentially using NPWT dressings for individuals thought to be at high risk of development of a lower extremity infection. This type of selection bias would push the observed relationship toward the null, thereby masking the benefit of NPWT dressings across the entire post-era cohort. Therefore, the use of NPWT dressings merits further study in a more controlled fashion.
The decontamination protocol against MRSA employed in this study has been described previously and was shown to be significantly associated with a decreased rate of SSI among elective orthopedic cases involving hardware implantation at our institution (OR 0.24, 95% CI 0.08–0.77, p = 0.02) [18]. Limited literature involving vascular surgery cohorts indicates that 2% chlorhexidine gluconate washcloths may potentially be associated with decreased rates of post-operative infections [27]. When our pre- and post-era cohorts were restricted to only outpatient elective cases, 37% of eligible patients received our three-component pre-operative decontamination protocol. Adjusting for confounders, we observed a significant decrease in both wound complications and re-operations after the implementation of the decontamination bundle.
Unlike other studies among vascular surgery patients [27,28], our decontamination protocol includes not only washcloths, but intranasal and oral components as well. This provides a comprehensive approach to pre-operative MRSA decontamination that has been shown previously to be associated with decreased rates of SSIs [29,30]. Given our promising findings, effort should be devoted to increase the proportion of outpatient elective patients who receive the decontamination protocol, and eligibility for the decontamination protocol may be expanded to include both outpatient and inpatient elective cases to maximize the number of patients who may benefit from the decontamination strategy.
The findings of this study should be interpreted in the context of its limitations. Given its retrospective nature and pre-post design, there is certainly the potential for residual confounding that may bias the results. Although baseline characteristics were largely similar between the pre- and post-eras, and despite controlling for clinically relevant covariates and surgeon experience in a propensity score-adjusted multi-variable analysis, unknown or unmeasured confounders may still bias the results. Although we identified substantial decreases in the rates of infection-related re-admissions and prosthetic graft infections, the study was underpowered to capture statistically significant differences among these secondary outcomes. Further, our predominantly male, veteran study population, limits broad generalization of the results.
Conclusion
This study demonstrates that a multi-tiered strategy aimed at decreasing the use of incisional groin staples, increasing the use of NPWT dressings, and implementing a decontamination bundle against MRSA can effectively decrease SSIs after open infra-inguinal re-vascularization in our cohort. The use of incisional staples in the groin should be avoided for vascular surgery patients because they represent a significant risk factor for deep groin SSIs and infection-related re-operations. The decontamination protocol should be considered for outpatient and inpatient elective cases to further minimize infection-related complications, and the use of NPWT dressings deserves further investigation.
Footnotes
Acknowledgment
This study was presented during the Vascular and Endovascular Surgical Society Paper Session at the 2017 Vascular Annual Meeting of the Society for Vascular Surgery; San Diego, CA, May 31–June 3, 2017.
Author Disclosure Statement
No competing financial interests exist.